Potential of the Combination of a Systemic Enzyme Complex and Probiotics administration to Combat COVID-19: A Randomized Open Label Prospective Analysis
Background: Enzymes have been used for therapeutic applications for decades owing to their anti-inflammatory and immunomodulatory effects. Probiotics are well known to reduce the incidence and severity of several health-related conditions. To our knowledge, no clinical trial has evaluated the effects of a combination of systemic enzyme and probiotic supplementation in Covid-19 patients infected with the SARSCoV-2 virus. Objective: We investigated the safety and efficacy of the health supplements ImmunoSEB (systemic enzyme complex) and ProbioSEB CSC3 (probiotic complex) as supplemental therapy in confirmed mild to moderate COVID-19 patients. Methods: A randomized, open label, 2-arm, prospective study in patients with an RT-PCR confirmed diagnosis of COVID-19 with a mild to moderate condition was conducted. The control arm (n=30) received standard of care (SOC) treatment and the test arm (n=30) received the oral supplements ImmunoSEB (500 mg/cap.) + ProbioSEB CSC3 (5 billion CFUs /cap.) for 14 days in addition to SOC. The efficacy and safety of the experimental regimen was compared with the control arm at various timepoints from days 1 to 21. Results: A significantly higher proportion of patients in the test arm showed clinical improvement on day 10 vs the controls (93.33% vs 60%; p<0.05). No adverse events were reported in the test arm at any time during the study suggesting the safety of supplementation with ImmunoSEB + ProbioSEB CSC3. Patients in the test arm also had a shorter duration of hospitalization, quicker recovery and faster reduction in CRP levels as compared to the control arm. Conclusions: The present study concludes that supplemental therapy with ImmunoSEB + ProbioSEB CSC3 accelerates clinical improvement in mild to moderate COVID-19 patients. While there is no vaccine or specific drug to completely cure SARS CoV-2 infection, the proposed supplemental therapy could be a potential tool to aid in the recovery of COVID-19 of patients.
Neha Shah1*, Rohit Parate2 and Abhay Vispute3
Keywords: COVID-19; ImmunoSEB; ProbioSEB CSC3; RT-PCR; SARSCoV-2; Supplement therapy Abbreviations: RT-PCR: Reverse transcription polymerase chain reaction; SARSCoV-2: Severe acute respiratory syndrome coronavirus 2; ImmunoSEB- Systemic enzyme complex; ProbioSEB CSC3: Probiotic complex
Introduction
SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2) is known to cause pneumonia like symptoms, affecting the lungs and other organs of the patient to create a severe condition which is potentially life threatening in many cases. In January 2020, WHO declared the infection to be a global public health emergency, calling on all countries to find ways to contain and treat the respiratory disease caused by this virus. According to the World Health Organization (WHO), as of October 23, 2020, 41,570,883 confirmed cases of COVID-19 have been recorded worldwide, with 1,134,940 confirmed deaths.
Although broad spectrum anti-viral drugs are being used currently to alleviate the infection, to date, no vaccine or specifically designed anti-virals have shown proven efficacy against SARS-CoV-2. Hence, the medical community has used available medications, oxygen therapy and mechanical ventilation to decrease the number of patients requiring prolonged hospitalization as well as to decrease mortality: hydroxychloroquine, chloroquine, remdesivir, umifenovir, favipiravir and a lopinavir/ritonavir combination. These are most extensively used due to their immunomodulatory properties, anti-viral activity and capability of mediating anti-inflammatory responses [1]. Unfortunately, the current drugs have shown limited efficacy in the treatment of Covid-19 and further studies are still in progress [2].
Considering the important role of enzymes in therapeutics, it is worthwhile to evaluate their potential in the management of COVID-19. The anti-inflammatory, antiviral and antibacterial potential of systemic enzymes is well documented in literature [3, 4, 5, 6, 7]. A recent report has suggested the potential of the anti-oxidant enzyme, catalase, for the treatment of COVID- 19 as it minimizes the reactive oxygen species distinctly produced during infection and inflammatory processes [8]. Protease serratiopeptidase, lysozyme and lactoferrin are biologically active molecules that play a vital role in enhancing immunity [9]. Serratiopeptidase is known for its anti-inflammatory, anti- biofilm, and fibrinolytic properties [10]. It has also shown immunomodulatory effects [11, 12]. Further, proteases have been proposed to treat immune diseases due to their unique immunomodulatory action [13]. Immunomodulatory and anti-inflammatory properties of another protease, papain, are well described in the review published by Pandey, et al. [14]. Thus, it is rational to speculate that a combination of proteolytic enzymes may potentially be useful in the management of COVID-19.
Probiotics are known to reduce the incidence and severity of several health conditions and are being studied for a possible role in the management of COVID-19. Probiotics are live microorganisms that confer health benefits when consumed in adequate amounts. Clinical studies have proven the immunomodulatory effects of the probiotics Bacillus clausii [15], Bacillus coagulans [16] and Bacillus subtilis [17, 18] in the treatment of respiratory tract infections. Present scientific evidence demonstrates the ability of probiotics to heighten human immunity and to maintain normal flora of the gastrointestinal tract [19]. In the perspective report published by Olaimat, et al. [19], the authors highlighted the necessity to evaluate the efficacy of probiotics in combating COVID-19.
The multi-enzyme formulation ImmunoSEB contains Peptizyme SP an enteric coated serratiopeptidase, bromelain, amylase, lysozyme, peptidase, catalase, papain, glucoamylase and lactoferrin to exert necessary therapeutic effects. ProbioSEB CSC3 is a combination of three probiotic strains: Bacillus coagulans LBSC (DSM 17654), Bacillus subtilis PLSSC (ATCC SD 7280), and Bacillus clausii 088AE (MCC 0538). We hypothesized that a combination of therapeutic enzymes (ImmunoSEB) and probiotics (ProbioSEB CSC3) would be beneficial in the management of COVID-19. To confirm the proposed hypothesis, we have designed an open-label, randomized, comparative, parallel-group, controlled study as proof of concept to evaluate the effect of the combination of ImmunoSEB and ProbioSEB CSC3 as supplemental therapy in confirmed mild to moderate COVID-19 patients.
Methods
Ethical considerations
The present study was conducted as per the ethical principles contained in the current revision of the “Declaration of Helsinki 2013”, ICH harmonised guideline integrated addendum to ICH E6 (R1): Guidelines for Good Clinical Practice ICH E6(R2) and following the “Ethical Guidelines for Biomedical Research on Human Subjects” issued by the Indian Council of Medical Research and all other applicable laws and regulations of the country. No vulnerable subject participated in the study.
Inclusion criteria
Patients who provided written informed consent; males or non-pregnant, non-lactating females aged ≥ 18 and ≤ 75 years (both inclusive); RT-PCR confirmed diagnosis of COVID-19; able to take the drug orally and comply with study procedures; and women of childbearing potential with a negative urine pregnancy test were included in the study.
Exclusion criteria
Patients with severe to critical health condition such as prior known respiratory distress (RR≥30 times/min), finger oxygen saturation ≤93% in a resting state, arterial partial pressure of oxygen (PaO2)/concentration of oxygen inhalation (FiO2) ≤300mmHg (1mmHg=0.133kPa), respiratory failure or on mechanical ventilation, in shock; patients with other viral pneumonia; patients who have received tumor immunotherapy (such as PD-1/L1, CTLA4, etc.) in the past 1 month or inflammatory factor modulators such as Ulinastatin; patients who have received organ transplantation or surgery in the past 6 months; patients unable to consume food or medications due to coma or intestinal obstruction; patients who have severe underlying diseases that affect survival, including uncontrolled malignant tumor with multiple metastases that cannot be resected (blood diseases, dyscrasia, active bleeding, severe malnutrition); women who are pregnant or lactating, or subjects (including male subjects) having a pregnancy plan (including plans for sperm donation or egg donation) during the study period; patients allergic to systemic enzyme supplements; patients whose ALT/AST levels are 5 times higher than the normal upper limit and total bilirubin is 3 times higher than the upper limit of normal or patients with child-Pugh grade C cirrhosis; patients on extracorporeal life support (ECLS) such as extracorporeal membrane oxygenation (ECMO), extracorporeal carbondioxide removal (ECCO2R), renal replacement therapy (RRT); patients facing imminent death in the opinion of the clinical team; and patients who have participated in any other clinical study within 2 weeks prior to randomization were considered ineligible to participate in the study.
Study design
An open-label, randomized, comparative, parallel-group, controlled study was conducted at two centers in India (S. R. V. Hospital, Mumbai & Chirayu Medical College & Hospital, Bhopal), by qualified investigators for a duration of 21 days. The study was registered with Clinical Trial Registry of India as per Indian regulations with the following registration numbers: CTRI/2020/09/027685 (Chirayu Medical College & Hospital, Bhopal) & CTRI/2020/08/027168 (S. R. V. Hospital, Mumbai).
A total of 60 subjects were randomized. A sample size of 30 in each group had 80% power to detect a difference of 15%, assuming that the proportion of patients with clinical improvement in the test arm is 90% and reference arm 75%. Due to various reasons, the attrition rate was factored up to 5%, and the allocation ratio was 1:1.
On day 1, patients were randomized in a 1:1 ratio to either the control arm (n=30) that received standard of care as per institutional practice (SOC) or the test arm (n=30) that received the oral supplements ImmunoSEB (500 mg/cap.) + ProbioSEB CSC3 (5 billion CFUs /cap.) for 14 days in addition to SOC. The SOC at both centers comprised an antibiotic Azithromycin (500mg/day), multivitamins, supplemental oxygen, as needed and paracetamol for fever, as needed.
Dose
Patients in the test arm received four capsules of ImmunoSEB daily (two capsules in the morning and two in the evening) on an empty stomach (1 hour before or 2 hours after a meal) with 1-2 cups of warm or room temperature water. They also received 2 capsules of ProbioSEB CSC3 daily, to be taken with lunch.
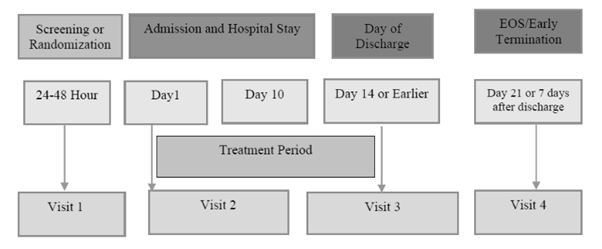
Screening schedule
• Visit 1: Initial screening (24-48 hrs).
• Visit 2: In-hospital stay (Day 1 to 10).
• Visit 3: Day of discharge (Day 14 or earlier if patients were RT-PCR negative or asymptomatic).
• Visit 4: Follow up visit (Day 21).
After obtaining informed consent, patients were screened as mentioned in the schedule of Assessment (Table 1). After confirmation of eligibility, patients were randomized to either receive supplemental therapy for a 14-day treatment period with standard of care as per institutional practice (test arm) or only standard of care (control arm). All patients were initially hospitalized. During the study, specimen collection, packaging, and transport of nasopharyngeal swab & oropharyngeal swab were done as per details provided in Table 1. During the study, assessments were performed as mentioned in the Schedule of Assessment (Table 1). Patients were discharged from the hospital based on the discharge criteria. Hospital discharge criteria was defined as resolution of symptoms and/or radiological improvement with a documented virological clearance in 2 samples at least 24 hours apart. Patient were discharged on Day 14 or earlier, based on their clinical condition. Day 21 was considered as the end of the study period.
| Parameters | Screening | In-hospital Stay | EOT/ Discharge1 | Follow up visit (Telephonic)2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Visits | 1 | 2 | 3 | 4 | |||||||||
| Day (±days) | 24-48 hours | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 14 | 21 |
| Written Informed Consent | X | ||||||||||||
| Hospitalisation/admission to study facility | X | X | X | X | X | X | X | X | X | X | |||
| Inclusion/Exclusion Criteria | X | ||||||||||||
| Clinical Status Assessment Scale | X | X | X | X | X | X | X | X | X | X | X | X | X |
| Medical and Surgical History | X | ||||||||||||
| Physical Examination | X | X | X | X | X | X | X | X | X | X | X | X | |
| Vital signs | X | X | X | X | X | X | X | X | X | X | X | X | |
| ECG | X | X | X | X | |||||||||
| Body Temperature | X | X | X | X | X | X | X | X | X | X | X | X | X3 |
| Demographic Information | X | ||||||||||||
| PCR for COVID viral load | X | X4 | X4 | X4 | |||||||||
| IP administration | X | X | X | X | X | X | X | X | X | X | X5 | ||
| Hematology | X | X | X | X | |||||||||
| Biochemistry (ALT/AST, S. creatinine, BUN, ALP) | X | X | X | X | |||||||||
| PT/APTT, INR | X | X | X | X | |||||||||
| Urinalysis (R/M) | X | ||||||||||||
| CRP & IL-66 | X | X | X | X | |||||||||
| X-RAY CHEST/ CT Scan | X | X | X | X7 | |||||||||
| Urine pregnancy test (In case of a female subject) | X | ||||||||||||
| Patient Diary | X | X | X | X | X | X | X | X | X | X | X8 | ||
| Adverse events | X | X | X | X | X | X | X | X | X | X | X | X | |
| Concomitant Medications | X | X | X | X | X | X | X | X | X | X | X | X | |
| 1. Day of discharge could be day 14 OR before/later as per the patient’s clinical condition | |||||||||||||
| 2. Follow up was done on Day 21 (7 days after the last dose on Day 14) | |||||||||||||
| 3.At the follow-up visit, body temperature recorded by the patient at home was conveyed to the site | |||||||||||||
| 4. During the hospital stay, if PCR results were negative for COVID viral load, another PCR after 24 hours was required to be performed | |||||||||||||
| 5. If a patient was discharged prior to 14 days, a telephonic call was conducted by the site every 3rd day until the 14th day to follow-up on IP compliance and Patient Diary completion. The record was documented in the patient source. | |||||||||||||
| 6. IL-6 was measured/evaluated in patients with CRP ≥10mg/L | |||||||||||||
| 7. EOT X-Ray was only required if the patient remained hospitalized | |||||||||||||
| 8. If discharge occurred before Day 14, subjects were required to continue taking the study treatment until day14 and record it in the patient diary |
Table 1: Schedule of Assessments.
Statistical Analysis
The categorical variables were expressed as frequencies and percentages, and continuous variables as mean and standard deviation. The data were analysed using ANCOVA followed by Dunnett’s test. *P< 0.05 was considered statistically significant.
Results
A total of 60 Asian healthy males and non-pregnant, non- lactating females were randomized to the control (n=30) and test arms (n=30). The mean ages of subjects in the control arm and test arm were 46.47 years and 47.10 years, respectively. Both genders were equally distributed in both the arms. There was no statistically significant difference in any demographic characteristics (e.g., age, gender, comorbidities or BMI) across study treatment groups.
Analysis of Efficacy
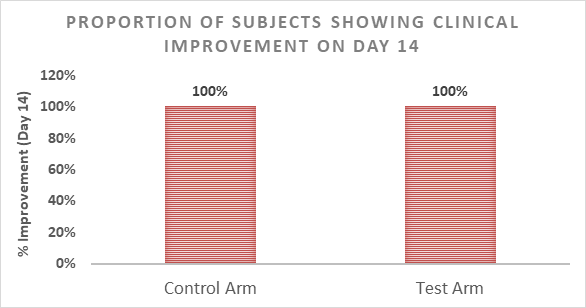
By day 14, 59 of 60 subjects were discharged from the hospital. As subjects in the control arm recovered by 14 days, there was no scope of improvement for the test arm in view of the primary end point (time frame of 14 days). Further, all the subjects in the test arm also recovered by 14 days suggesting there was no adverse/negative effect of supplementation on clinical symptoms (Figure 2).
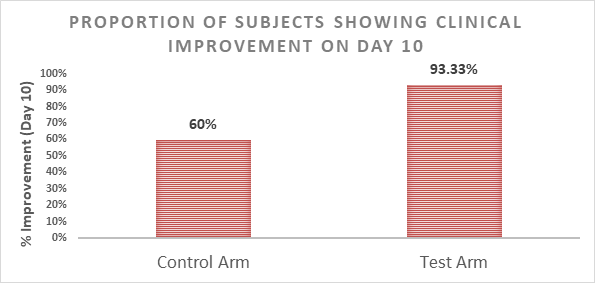
Further, analysis of patients on day 10 (abbreviated primary endpoint) was performed. Supplementation with ImmunoSEB + ProbioSEB CSC3 had a significant effect (p=0.0489) on clinical improvement on day 10, with 18 of
30 (60%) subjects in the control arm vs 28 of 30 (93.33%) subjects in the test arm showing clinical improvement (Figure 3).
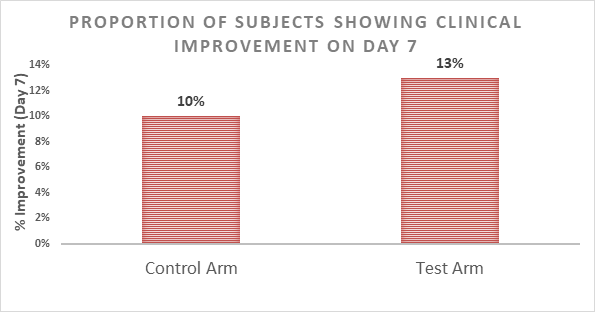
On day 7, only 7 of 60 subjects were discharged from the hospital. Supplementation with ImmunoSEB + ProbioSEB CSC3 had no significant effect on clinical improvement on day
7, with 3 of 30 (10%) subjects in the control arm vs 4 of 30 (13%) subjects in the test arm showing clinical improvement (Figure 4).
In both study arms 100% of patients showed clinical improvement on Day 21 (data not shown).
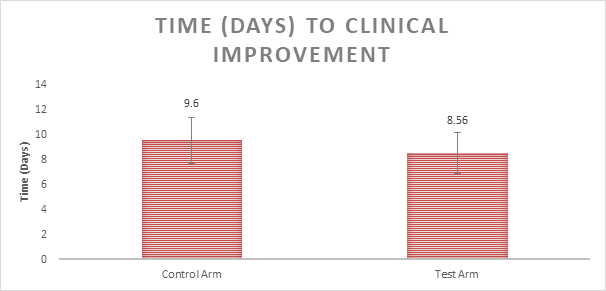
The mean time to clinical improvement was 9.6 days and 8.56 days in the control and test arms, respectively (Figure 5). These results, though not statistically significant, suggest that supplementation may result in faster clinical improvement (p=0.1941).
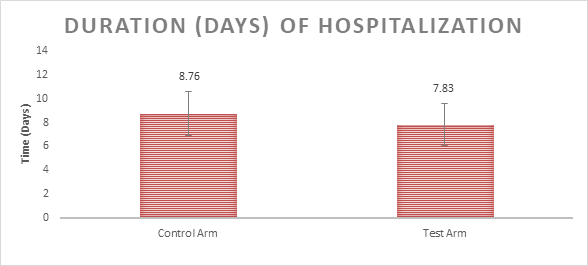
The mean days of hospitalization were 8.76 and 7.83 days in the control and the test arms, respectively (Figure 6). These results, though not statistically significant, suggest that supplementation may reduce hospital stay by approximately 1 day (p=0.1759).
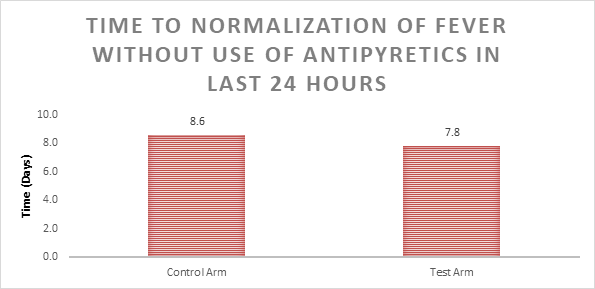
Mean days to normalization of fever without the use of antipyretics in the previous 24 hours was 8.6 days and 7.8 days in the control and the test arms respectively (Figure 7).
These results, though not statistically significant, suggest that supplementation may reduce fever faster by approximately 1 day (p=0.1105).
The mean improvement in SpO2% was 0.74 + 2.50 and 0.92 + 2.53 % in the control and the test arms respectively. The intervention had little to no effect on SpO2 levels (data not shown).
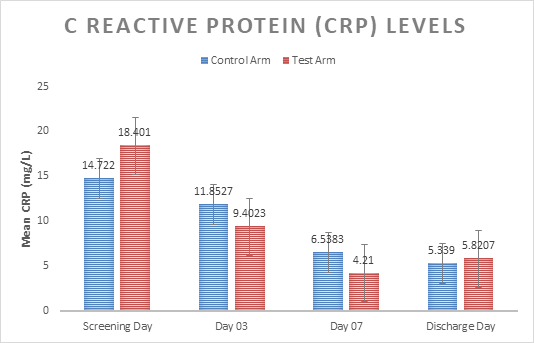
The mean reduction in CRP levels on Day 3 as compared to baseline was 20% and 49% in the control and the test arms respectively. The mean reduction in CRP levels on Day 7 was 56% and 77% in the control and the test arms respectively (Figure 8). The mean reduction in CRP levels on the day of discharge was 63% and 68% in the control and the test arms respectively. These results suggest that supplementation with ImmunoSEB + ProbioSEB CSC3 may cause a more rapid decline in the inflammatory marker. Supplementation with ImmunoSEB + ProbioSEB CSC3 had a significant effect (p=0.0349) on reduction of CRP levels on discharge day vs baseline.
Analysis of Safety
At the time of discharge, no patient in the control or the test arms showed any deterioration in clinical condition. No subject in either arm reported any adverse event at any time during the study. No subject in the test arm reported nausea, vomiting, diarrhea or rashes, suggesting the safety and tolerability of supplementation with ImmunoSEB + ProbioSEB CSC3. All laboratory parameters were in the normal ranges or were not clinically significant, as assessed by the treating physician.
Discussion
The rapid spread of the SARSCoV-2 virus resulting in the worldwide COVID-19 pandemic has created an urgent need to develop safe and effective therapeutic approaches. In view of this, the present clinical study focused on dietary supplements. We examined the effect of a combination of systemic enzymes and probiotics in the management of COVID-19.
In the first reported study of supplemental therapy with systemic enzymes and probiotics in mild to moderate patients with COVID-19, we report evidence for the following: (i) supplementation with ImmunoSEB + ProbioSEB CSC3 significantly improves clinical status; (ii) the supplements are safe and well-tolerated in adults; and (iii) a trend towards faster clinical improvement, reduced days of hospitalization, quicker normalization of fever and faster reduction in the inflammatory marker (CRP) levels.
Day 14 was chosen as the primary endpoint because at the time of study planning, the Government of India guidelines for the clinical management of COVID-19 required a minimum 14 day hospital stay for patients with a confirmed diagnosis of COVID-19. Since then, treatments and management of the disease evolved and patients were discharged earlier, based on negative COVID-19 tests and clinical condition. Hence, we used 10 days as an abbreviated primary end point and observed statistically significant clinical improvement in the patients that received the supplemental treatment.
Faster recovery, improved clinical status and a reduction in days of hospitalization highlight the benefits of the supplemental treatment in COVID-19 patients. This could potentially lead to significant cost savings and also free up hospital resources to accommodate the more severely ill patients. The recovery was 100% in both control and test arms (after 14 days) indicating the supplementation did not cause any negative impact on clinical symptoms in COVID -19 patients.
Further, CRP is an inflammatory marker and its levels are elevated in chronic conditions or during infections. Supplementation with ImmunoSEB + ProbioSEB CSC3 resulted in a faster decline in CRP levels. The shorter time to clinical improvement in the test arm may possibly be attributable to an ImmunoSEB-mediated reduction in CRP levels. Serratiopeptidase, a component of the ImmunoSEB complex, has been reported to have anti-inflammatory properties [10]. Probiotics have also been shown to reduce levels of inflammatory markers, including CRP [20]. Thus, ProbioSEB CSC3 may also have contributed to the reduction in CRP and hence, the faster clinical improvement. Though this data was not prospectively collected, at follow up, subjects in the test arm reported feeling better, less fatigued and were able to resume their daily activities. This information, though anecdotal, may be very relevant as a large number of people who contract the SARSCoV-2 virus do not fully recover in a few weeks. Chronic fatigue has been reported to be a long- term effect of COVID-19 [21].
The clinical improvement observed in this study may be attributable to the immunomodulatory effects of the various components of the supplements. Serratiopeptidase is a proteolytic enzyme with anti-edemic, analgesic, fibrinolytic and caseinolytic properties and is used therapeutically for its anti-inflammatory properties [22]. A combination of lysozyme and lactoferrin has demonstrated immunomodulatory effects in the treatment of tuberculosis in a 120 patient clinical study [23]. Additionally, the antiviral effect of a combination of lysozyme and lactoferrin is well illustrated in the study done by Malczewska, et al. [24]. The role of probiotics in the management of inflammatory response, severe pneumonia, endotracheal colonization and ventilator-associated pneumonia, has been explored in various studies in terms of decreasing the length of ICU and hospital stay [25, 26]. Oral consumption of probiotics has also been suggested to prevent antibiotic-associated diarrhoea owing to the normalization of unbalanced gastrointestinal flora [27]. Thus, supplementation with probiotics, in addition to potential immunomodulatory effects, could also contribute to protecting against the adverse effects of antibiotics and other drugs used in the management of COVID-19.
Conclusion
In conclusion, the present study supports the use of a combination of ImmunoSEB and ProbioSEB CSC3 to improve the clinical condition of COVID-19 patients. The findings also confirm the safety and tolerability of these oral supplements in these patients. Further longer-term studies to give stronger evidence about the efficacy and safety of these supplements, possibly in patients with moderate to severe clinical condition, are warranted
Acknowledgements
The authors would like to thank Advanced Enzyme Technologies Ltd. for sponsoring the clinical study, Specialty Enzymes & Probiotics for providing the supplements, Dr. Abhijit Rathi for his invaluable contribution in the planning and implementation of the study and Dr. Swati Jadhav for her help in preparing and reviewing the manuscript.
Author’s contribution
Dr. Rohit Parate and Dr. Abhay Vispute acted as principal investigators of this study and Dr Neha Shah was involved in study design, planning, protocol writing, data analysis and manuscript preparation.
References
-
Scavone C, Brusco S, MBertini M, Sportiello L, Rafaniello C, et al. (2020) Current pharmacological treatments for COVID-19: What’s next? Br J Pharmacol 177(21): 4813- 4824.
-
Gioia M, Ciaccio C, Calligari P, De Simone G, Sbardella D, et al. (2020) Role of proteolytic enzymes in the COVID-19 infection and promising therapeutic approaches. Biochem Pharmacol 182: 114225.
-
Craik CS, Page MJ, Madison EL (2011) Proteases as therapeutics. Biochem J 435(1): 1-16.
-
Al Kassa I (2016) Antiviral probiotics: A new concept in medical sciences. New Insights on Antiviral Probiotics, pp: 1-46.
-
Marzin T, Lorkowski G, Reule C, Rau S, Pabst E, et al. (2017) Effects of a systemic enzyme therapy in healthy active adults after exhaustive eccentric exercise: a randomised, two-stage, double-blinded, placebo-controlled trial. BMJ Open Sport Exerc Med 2(1).
-
Farhadi SA, Bracho-Sanchez E, Freeman SL, Keselowsky BG, Hudalla GA (2018) Enzymes as immunotherapeutics. Bioconjug Chem 29(3): 649-656.
-
Liu Y, Alookaran JJ, Rhoads JM (2018) Probiotics in autoimmune and inflammatory disorders. Nutrients 10(10): 1537.
-
Qin M, Cao Z, Wen J, Yu Q, Liu C, et al. (2020) An antioxidant enzyme therapeutic for COVID-19. Adv Mater 32(43).
-
Mann JK, Ndung’u T (2020) The potential of lactoferrin, ovotransferrin and lysozyme as antiviral and immune- modulating agents in COVID-19. Future Virol 15(9): 2217.
-
Jadhav SB, Shah N, Rathi A, Rathi V, Rathi A (2020) Serratiopeptidase: Insights into the therapeutic applications. Biotechnol Rep 28: e00544.
-
Fadl NN, Ahmed HH, Booles HF, Sayed AH (2013) Serrapeptase and nattokinase intervention for relieving Alzheimer’s disease pathophysiology in rat model. Hum Exp Toxicol 32(7): 721-735.
-
Rajinikanth B, Venkatachalam VV, Manavalan R (2014) Investigations on the potential of serratiopeptidase- a proteolytic enzyme, on acetic acid induced ulcerative colitis in mice. Int J Pharm Pharm Sci 6(5): 525-531.
-
Rani K (2020) Immunomodulatory effects of proteolytic enzymes: meteoric brief review. Adv tissue Eng Regen Med 6(2): 44-45.
-
Pandey S, Cabot PJ, Shaw PN, Hewavitharana AK (2016) Anti-inflammatory and immunomodulatory properties of _Carica papaya_. J Immunotoxicol 13(4): 590-602.
-
Marseglia GL, Tosca M, Cirillo I, Licari A, Leone M, et al. (2007) Efficacy of _Bacillus clausii_ spores in the prevention of recurrent respiratory infections in children: a pilot study. Ther Clin Risk Manag 3(1): 13-17.
-
Baron M (2009) A patented strain of _Bacillus coagulans_ increased immune response to viral challenge. Postgrad Med 121(2): 114-118.
-
Lefevre M, Racedo SM, Ripert G, Housez B, Cazaubiel M, et al. (2015) Probiotic strain _Bacillus subtilis_ CU1 stimulates immune system of elderly during common infectious disease period: a randomized, double-blind placebo-controlled study. Immun Ageing 12: 24.
-
Elshaghabee FMF, Rokana N, Gulhane RD, Sharma C, Panwar H (2017) Bacillus as potential probiotics: status, concerns, and future perspectives. Front Microbiol 8: 1490.
-
Olaimat AN, Aolymat I, Al-Holy M, Ayyash M, Ghoush MA, et al. (2020) The potential application of probiotics and prebiotics for the prevention and treatment of COVID-19. NPJ Sci Food 4(17).
-
Mazidi M. Rezaie P, Ferns GA, Vatanparast H (2017) Impact of probiotic administration on serum C - reactive protein concentrations: Systematic review and meta- analysis of randomized control trials. Nutrients 9(1): 20.
-
Mayo clinic (2020) COVID-19 (coronavirus): Long-term effects.
-
Tiwari M (2017) The role of serratiopeptidase in the resolution of inflammation. Asian J Pharm Sci 12(3): 209-215.
-
Mohanty KC, Bendre S, Sarangdhar N, Fadia R (2012) Efficacy of lysozyme-lactoferrin as a bioenhancer (immunomodulator) in the treatment of Tuberculosis. RGUHS J Med Sci 2(2): 91-95.
-
Małaczewska J, Kaczorek-Łukowska E, Wojcik R, Siwicki AK (2019) Antiviral effects of nisin, lysozyme, lactoferrin and their mixtures against bovine viral diarrhoea virus. BMC Vet Res 15: 318-330.
-
Cook DJ, Johnstone J, Marshall JC, Lauzier F, Thabane L, et al. (2016) Probiotics: prevention of severe pneumonia and endotracheal colonization Trial-prospect: a pilot trial. Trials 17: 377.
-
Johnstone J, Heels-Ansdell D, Thabane L, Meade M, Marshall J, et al. (2019) Evaluating probiotics for the prevention of ventilator-associated pneumonia: a randomised placebo-controlled multicentre trial protocol and statistical analysis plan for Prospect. BMJ Open 9(6).
-
Blaabjerg S, Artzi DM, Aabenhus R. Blaabjerg S (2017) Probiotics for the prevention of antibiotic-associated diarrhea in outpatients-A systematic review and meta- analysis. Antibiotic 6(4): 21.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells