Clinical and Protein Biomarkers in Sepsis: Insights from Hospital-Based Case Studies
Background: Sepsis is a severe life-threatening state of infection with a high incidence in clinical settings and is one of the most common causes of hospitalization and deaths in the Critical Care Unit (CCU). The current research work was carried out to investigate the aetiology and pathophysiology of sepsis in the in-patients of Mahavir Hospital, Hyderabad, Telangana, India. This study aims to identify clinical and protein biomarkers that can effectively diagnose and predict the risk outcomes of sepsis in hospitalized patients. Patients and Methods: Observations are based on 20 case studies of patients including male and female subjects. All the parameters studied were investigated using standard protocols by collecting blood samples from the patients and estimating blood and clinical parameters and the protein markers such as procalcitonin (PCT), D-Dimer and C-Reactive Protein (CRP), which are considered as important biomarkers of sepsis. Demographic details were collected in a questionnaire and tabulated. Results: This study identified several clinical parameters and protein biomarkers that were significantly associated with sepsis. It was found that key biomarkers had elevated levels of procalcitonin, C-reactive protein, and specific cytokines. Additionally, clinical parameters such as heart rate, respiratory rate, and white blood cell count were found to be critical indicators. The combination of these biomarkers provided a robust model for the early diagnosis and prognosis of sepsis. The results demonstrated that PCT rapidly rises in almost all tested patient’s blood. Further correlation with demographic parameters and the disease's etiology across various stages revealed that some of these proteins could serve as significant biomarkers for the early detection of sepsis. Conclusion: The identification of these clinical and protein biomarkers offers valuable insights into the pathophysiology of sepsis and can enhance early diagnosis and personalized treatment strategies. Further validation in larger, diverse cohorts is warranted to confirm these findings and facilitate their integration into clinical practice.
K Jamil1*, N Chaitanya2, M Al Saiqali3, Irfana1, B Fatima1, M Asimuddin1 and MA Zahid2
Abbreviations
SIRS: Systemic Inflammatory Response Syndrome; SOFA: Sequential Organ Failure Assessment; WHO: World Health Organisation; UTI: Urinary Tract Infections; PAMPs: Associated Molecular Patterns; PRRs: Pattern Recognition Receptors; IEC: Institutional Ethics Committee.
Introduction
The World Health Organisation (WHO) [1, 2] has declared that yearly around 31.5 million people suffer from sepsis with six million annual mortalities worldwide. Sepsis is one of the most leading causes of CCU hospitalization, and its frequency continues to increase. Sepsis is a life-threatening organ dysfunction condition, mainly due to dysregulated host response to many types of infections [3]. Infections can happen when the immune system overreacts to the infection and starts to damage the tissues and organs. Sepsis is sometimes called septicaemia or blood poisoning [4]. The causes of sepsis include bacterial, fungal, and/ or viral infections. Sepsis does not arise on its own, it stems from another medical condition, such as an infection in the lungs, urinary tract, abdomen (e.g., appendicitis) or other part of the body. With pneumonia and urinary tract infections (UTI) being common illnesses that cause sepsis including invasive medical procedures like the insertion of a vascular catheter can introduce bacteria into the bloodstream and bring on the condition [5].
Sepsis or Septicemia is more common in people who are admitted in the hospital for various treatments or those who had recent surgery, especially those who have catheters or IVs or ventilators or all other devices attached to the body of the patients, or those who are old and vulnerable or even very young, or those that have infections or other chronic medical conditions (for example, lung diseases, COPD, diabetics, CVD, or neoplasia) or have severe injuries, such as extensive burns or open wounds, or have weak immune system. While the exact pathophysiology of sepsis remains largely unknown, a variety of factors interfere to modulate the response of the host to an infectious stimulus and this has direct implications both on clinical severity and outcome [6, 7].
Sepsis is a life-threatening condition it can be classified into three stages based on severity: sepsis, severe sepsis, and septic shock.
Sepsis
Sepsis is the body’s extreme response to an infection. It occurs when an infection triggers a chain reaction throughout the body. The initial stage of sepsis is characterized by systemic inflammation, known as the systemic inflammatory response syndrome (SIRS), which occurs in response to infection. Common symptoms include fever, chills, rapid breathing, increased heart rate, and confusion. The infection can be localized to a specific area but starts to affect the whole body.
Severe Sepsis
Severe sepsis is a progression of sepsis where the body’s response to infection begins to cause organ dysfunction. This stage indicates that the sepsis is affecting vital organs and systems. Symptoms are similar to sepsis but more severe, with additional symptoms specific to the organ systems affected, such as significant drops in blood pressure, severe shortness of breath, or marked confusion.
Septic Shock
Septic shock is the most severe form of sepsis, characterized by persistent hypotension (low blood pressure) that does not respond adequately to fluid replacement and requires vasopressor therapy. It also involves profound organ dysfunction and is associated with a higher risk of death. Patients with septic shock often exhibit severe hypotension, cold extremities, rapid and shallow breathing, severe anxiety or confusion, and reduced urine output. This stage requires immediate and aggressive treatment in an intensive care unit (ICU).
However, not all patients with sepsis develop a clinical condition of the same severity. This is partly due to the variations in genetic susceptibility, and the fact that the quantitative characteristics of the Pathogen Associated Molecular Patterns (PAMPs) and Pattern Recognition Receptors (PRRs) interaction are not similar in all patients. However, it may even be the case that the qualitative characteristic of this interaction is largely different between patients [8]. PRRs and mediators of inflammation are mostly protein molecules encoded by genes.
The diagnosis of sepsis is clinically based on several parameters, including qSOFA, SOFA, and SIRS, combined with information from the patient’s history, physical examination, laboratory tests, and imaging studies [9]. The diagnostic terminology is explained as follows: I. Quick Sequential (Sepsis-Related) Organ Failure Assessment (qSOFA): Assessment of altered mentation, systolic blood pressure and respiratory rate. II. Sequential Organ Failure Assessment (SOFA): A more detailed scoring system that includes measurements of respiratory, cardiovascular, hepatic, coagulation, renal, and neurological function. III. Systemic Inflammatory Response Syndrome (SIRS): Criteria that include temperature, heart rate, respiratory rate and white blood cell count. Immediate or early recognition and prompt treatment are crucial to improving outcomes in sepsis patients.
Sepsis diagnosis is a dynamic process that requires continuous re-evaluation as new information becomes available and the patient’s condition evolves [10].
Research showed that protein biomarkers such as Procalcitonin (PCT) combined with other proteins like C-reactive protein (CRP), D-dimer (DD) and few other markers including acute physiological condition and chronic health evaluation are also effective at diagnosing sepsis [11]. D-dimer (DD) is an indicator of coagulation function where coagulation dysfunction often occurs in sepsis patients, especially in septic shock patients, indicating the severity and prognosis of sepsis [12]. Procalcitonin, a 12.6-kD and 114-amino-acid polypeptide, is a precursor of calcitonin hormone produced in medullary C-cells of the thyroid gland and serves as a biomarker of bacterial infection and sepsis [13, 14]. During the recent years a relationship was established between serum levels of PCT and the severity of injury to various organs in sepsis. These studies have shown that PCT might be a suitable marker to monitor the inflammatory status of patients who have been injured and are at risk [15].
PCT levels on admission of patients were reported to be useful for predicting the severity, specificity and outcome of patients with pneumonia [16]. It has a low serum level (0.033 ng/ml) in all healthy individuals, but it increases up to 1000 times of normal level in acute inflammatory conditions. Also, it has been proved that D-dimer, a factor of coagulation, is significantly increased during sepsis. D-dimer has been used as a biomarker of sepsis severity and many researchers have shown that D-dimer is a potent indicator of mortality in sepsis and it is related to acute physiology and chronic health condition such as II (APACHEII) and simplify acute physiology score II (SAPSII) scores. This study investigated the levels of PCT, DD and CRP in sepsis patients along with severity and prognosis of sepsis [17].
In order to evaluate these parameters in assessing sepsis severity for prognosis, this study proposed to understand and determine the pathophysiology of sepsis. Furthermore, current research proved that biomarkers can have an important role in the disease process because they can indicate the presence or absence or severity of sepsis and have the potential to serve a crucial role by providing important information to clinicians to determine their treatment strategies beyond the standard therapy. To the best of our knowledge there are only a few clinical studies that combine these three biomarkers as major indicators for the diagnosis and prognosis of sepsis patients.
Materials and Methods
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Ethics Committee (IEC) of Bhagwan Mahavir Medical Research centre. Informed consent was obtained from the patients after explaining them the aim of the study, and patient confidentiality was strictly maintained. The aim of the study was explained to the patients and a written consent was taken from patients under study.
Study Design
This investigation is a hospital-based study on sepsis and was conducted to investigate the role of biomarkers and correlate with epidemiology and demographic parameters of the patients, through a detailed analysis of twenty case studies. The inclusion criteria for the cases were those patients diagnosed with sepsis and admitted to Critical Care Unit of Mahavir Hospital and research. Exclusion criteria included those who had CVD, cancer or other illnesses.
Questionnaire was used to record the demographic and clinical characteristics of the patients. Comparative analysis was performed to identify common patterns and differences among the cases. Primary Data were collected from questionnaire and Blood samples of patients collected for biochemical analysis, whereas, secondary data from patients’ medical records.
Epidemiology and Data Recording
Patients’ demographic data and vital signs were recorded, to study their epidemiology and aetiology. A questionnaire was prepared which formed the basis of data collection on epidemiology and demographic details. On the other hand, biochemical and haematological tests were carried out to support the data obtained. The general protocol for each patient was collection of baseline clinical data, Sepsis-related Organ Failure Assessment (SOFA) score and Acute Physiology and Chronic Health Evaluation (APACHE II) score and blood sampling. Each procedure was performed within the first 24 hours of admission. During the days of hospital stay the patients were monitored with daily recording of any relevant data registered in medical records, using a standardized case report form.
Protocols for Studies on Biomarkers
Procalcitonin Test and Its Procedure Serum from the blood sample was collected and used to determine the levels of procalcitonin, using kit-method. In this method the microplate reader provided in the kit was pre- coated with the antibody specific to procalcitonin. Samples were added to the microplate wells with a biotin-conjugated antibody specific to procalcitonin. Then, Avidin conjugated to Horseradish Peroxidase (HRP) was added to each microplate well and incubated, lastly, TMB substrate solution was added. Change in colour was observed only in the wells that contain procalcitonin, biotin-conjugated antibody and enzyme- conjugated Avidin. To terminate the enzyme-substrate reaction, sulphuric acid solution was added and the colour change was measured spectrophotometrically at a wavelength of 450nm ± 10nm (Table 1). The concentration of procalcitonin in the samples was then determined by comparing the O.D. of the samples to that of the standard [18].
| Procalcitonin value PCT (μg/L) | Interpretation |
|---|---|
| <0.05 | Healthy adult |
| 0.05 - <0.5 | Systemic infection is unlikely although localized infection is possible |
| 0.5 - <2 | Systemic infection is possible but other conditions (e.g. major trauma, recent surgery, severe cardiogenic shock) may also induce significant PCT rises. |
| 2.1 – <10 | Systemic infection is likely. |
| ≥ 10 | High likelihood of severe bacterial sepsis or septic shock. |
Table 1: Interpretation of Procalcitonin values.
Determining the Levels of C- Reactive Protein (CRP) CRP was measured quantitatively by slide agglutination test using latex particles coated with CRP antiserum which were allowed to react with test serum as per the manufacturer’s protocol. Agglutination was observed if CRP was present in a concentration of 6 mg/L or above in the patients’ serum samples (Table 2). The normal cut off value for CRP was between (0.8 – 1) (Ridker eyal and Rifai N) [19, 20].
| Value (mg /L) | Indication |
|---|---|
| 0.8 -1 | Normal |
| 1-2.9 | Intermediate risk |
| >3 | Higher risk of heart ailments |
| >10 | High level of inflammation in the body |
Table 3: Values of CRP tests and risk levels.
D-DIMER Test and Its Procedure Blood samples were centrifuged for 15 minutes at 1,000xg at 2-80 Celsius within 30 minutes of collection. The freshly prepared plasma was immediately used or stored in aliquots at -200 Celsius for later use. The assay determined the competitive inhibition enzyme immunoassay technique, as a monoclonal antibody specific to D2D has been pre- coated onto a micro plate. A competitive inhibition reaction is launched between biotin labelled D2D and unlabelled D2D [Standard or samples] with the pre-coated antibody specific to D2D. After incubation the unbound conjugate was washed off, followed by avidin conjugated to Horse Radish Peroxidase [HRP] was added to each micro-Plate well and incubated. The amount of bound HRP Conjugate is reversely proportional to the concentration of D2D in the sample. After addition of the substrate solution the intensity of colour developed was reversely proportional to the concentration of D2D in the sample. The kit was a competitive inhibition enzyme immunoassay technique for in-vitro quantitative measurement of D2D in human plasma (Table 3).
| Type | Gender | Age group | Value |
|---|---|---|---|
| D-Dimer | Both male and female | All age groups | <250 ng/ mL |
Table 2: showing D-Dimer normal values.
Blood Differential Test The blood differential test was performed to measure the percentage of each type of white blood cell (WBC) in the blood samples. It also reveals the existence of any abnormal or immature cells. A drop of blood is smeared onto a glass slide. The smear is stained with a special dye, which helps to differentiate between various types of white blood cells. Five types of white blood cells, also called leukocytes, normally appear such as: Neutrophils, Lymphocytes (B cells and T cells), Monocytes, Eosinophils and Basophils, each type of cell were counted, the test results will vary based on cell counts, the normal results for adults are shown in Table 4 but different labs may show slight variations.
| Blood component | Normal levels |
|---|---|
| Haemoglobin | In male 14 – 18.0 g/dL |
| In female 12.0 - 16.0 g/dL | |
| Haematocrit | In male: 38.8% - 50.0% |
| In female: 34.9% - 44.5% | |
| White Blood Cell count | 3.5 x103 to 10.5 x103 cells /mcL |
| Platelet count | 15x104 to 45x104 platelets/mcL |
Table 4: Range of normal WBC count.
Statistical Analysis
The patients were divided into four groups as follows; the first group consisted of low risk sepsis, second group, possible of developing sepsis, third one, moderate risk of sepsis, and fourth group was sever sepsis/higher progression of sepsis according to the severity of the sepsis.
Descriptive analysis of the data was carried out using mean values and standard deviation (SD). Normality of the variables was assessed with the Shapiro-Wilk-test. Comparisons between groups were performed with unpaired two-tailed t-test, Mann-Whitney-test or chi- squared-test with continuity correction, as appropriate. In order to investigate the gender difference between male and female patients’ blood sugar and blood urea a Simple Linear Regression were performed.
Wherever possible a p-value of <0.05 was considered statistically significant. Analyses were performed using the R open-source statistical software and the SPSS statistical package (version 23 for Windows. SPSS, Inc. Chicago, Ill).
Results
In the present study, a total of twenty cases with clinical suspicion of sepsis were included. The patient’s demographic details and past history of the disease were evaluated and recorded. A questionnaire was prepared to collect the required data from the patients with the approval of ethics committee and with patient consent. Patients were divided into four groups based on their age i.e., 50% male and 50% female patients, and among these 60% were in the age group of 60 to 80 years (Table 5). It was observed that elderly patients of the age group between 60-80 years were severely affected.
| Age Group of Patients | Percentage |
|---|---|
| 20-40 YRS | 5% |
| 40-60YRS | 25% |
| 60-80 YRS | 60% |
| 80 -90 YRS | 10% |
Table 6: Age- wise distribution of patients.
Symptoms and Severity
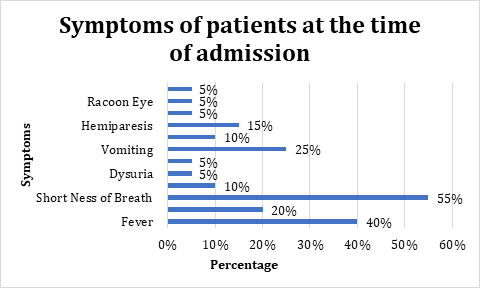
Clinical information, and laboratory-tests data were recorded and also symptoms at the time of admission to Hospital-Critical Care Unit and presented in Figure 1 & Table 6.
| Sl.No | Symptoms | No. of Patients | Percent Severity of Symptoms (%) |
|---|---|---|---|
| 1 | Shortness of Breath | 11 | 55 |
| 2 | Fever | 8 | 40 |
| 3 | Vomiting | 5 | 25 |
| 4 | cough | 4 | 20 |
| 5 | Hemiparesis | 3 | 15 |
| 6 | Chest Pain | 2 | 10 |
| 7 | Loose motions | 2 | 10 |
| 8 | Dysuria | 1 | 5 |
| 9 | Head Ache | 1 | 5 |
| 10 | Hematoma | 1 | 5 |
| 11 | Racoon Eye | 1 | 5 |
| 12 | Facial Oedema | 1 | 5 |
Table 5: Symptoms of patients according to severity.
Figure 1 showed that, on admission to the hospital, common symptoms that show evidence of the disease includes: high fever in 40% cases, high heart rate plus tachycardia. It was observed that about 55% of patients exhibited shortness of breath, whereas symptoms of vomiting recorded in 25% of sepsis patients, in addition, chest pain and loose motions were noted in 10% of patients. These observations are quite interesting as it clearly demonstrated the progression and the development of sepsis as well as complication of the cases.
Co-Morbidities at the Time of Admission
The co-morbidities that existed in sepsis patients at the time of admission in hospital are listed in the Table 7 & Figure 2. It is observed that, about 70% were hypertensive, and 65% were Diabetics, 40% were having urinary tract infection (UTI) and about 40% to 50% had fever and shortness of breath. Further, for each patient, a complete blood analysis (CBP), including assessment of the biomarkers (CRP, PCT and D-dimer) was performed within the first 48 hours after admission.
| Sl.no | Co-Morbidity | Number of Patients | Percentage % |
|---|---|---|---|
| 1 | Hypertension | 14 | 70 |
| 2 | Diabetes | 13 | 65 |
| 3 | Urinary Tract Infection (UTI) | 8 | 40 |
| 4 | Lower respiratory tract infection | 7 | 35 |
| 5 | Chronic Kidney Disease (CKD) | 5 | 25 |
| 6 | Chronic obstructive pulmonary disease (COPD) | 5 | 25 |
| 7 | Acute kidney Infection | 4 | 20 |
| 8 | Cerebro vascular accident | 4 | 20 |
| 9 | Multiple Organ dysfunction Syndrome | 4 | 20 |
| 10 | Hypotension | 3 | 15 |
| 11 | Aspiration Pneumonia | 3 | 15 |
| 12 | Urosepsis | 3 | 15 |
| 13 | Post-Operative Cases | 2 | 10 |
| 14 | Ischemic Stroke | 2 | 10 |
| 15 | Evans Syndrome | 1 | 5 |
| 16 | Cellulitis | 1 | 5 |
| 17 | Chronic Bronchitis | 1 | 5 |
| 18 | Ischemic Stroke | 2 | 10 |
Table 7: Co-morbidities of sepsis patients: Table arranged in descending order of the number of patients with each co-morbidity.
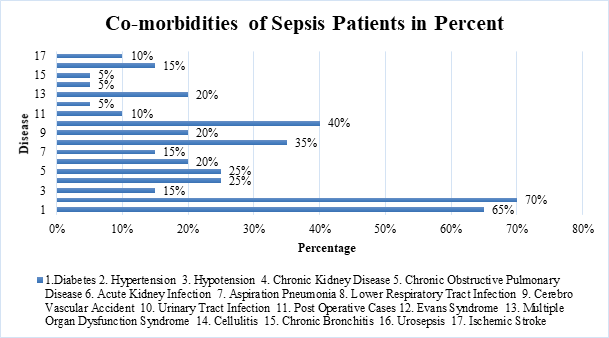
The correlation of haematological data with protein biomarker is expressed in Table 8 & Figure 3. The data indicates a single sepsis patient exhibited more than one co- morbid condition at the time of admission to the hospital. The data indicates that a single patient had more than one co-morbid condition (Table 6).
| Increased Blood Biochemical Parameters | No of Patients | Percentage |
|---|---|---|
| C-RP Levels | 5 | 25% |
| Procalcitonin Levels (PCT) | 17 | 85% |
| D-Dimer Levels (DD) | 7 | 35% |
| WBC Counts | 17 | 85% |
| Blood Urea Levels | 13 | 65% |
| Blood Sugar Levels | 13 | 65% |
Table 8: Protein Biomarkers from blood and serum samples of patients.
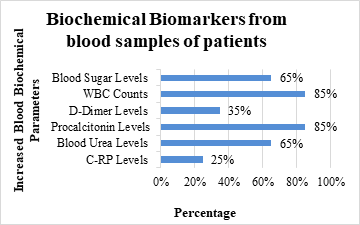
In sepsis patients the sugar level and urea level were found to be up to 65% higher than the controls, a few authors have shown similar pattern [21, 22], similarly, 85% rise in PCT indicates that this protein can be a very useful biomarker for sepsis. Several studies have also endorsed this parameter as a useful Biomarker [23, 24, 25]. Similarly, a simple WBC test can also predict a disease condition but may not be specific for sepsis.
The best cut-offs points for CRP, DD, and PCT are presented in the methods and materials section (Tables 2 & 3). The analysis identified a “cluster” of patients with several characteristics this suggests a more severe condition due to high infections. Our data demonstrated that there is a positive correlation between PCT and CRP which reached 90%. Whereas, such correlation was not found with regard to DD test (Table 8). The CRP levels in the sepsis patients were found to vary from 0.60 to 9.60 mg/dl. D-dimer is a fibrin degradation product (FDP) a small protein fragment present in the blood after a blood clot is degraded by fibrinolysis. It contains two D fragments of the fibrin protein joined by a cross link hence forming a protein dimer. The blood of a healthy individual contains very low levels of D-Dimer, but in sepsis cases we found high levels of D -Dimer. Hence, D-dimer can be considered as a significant prognostic factor in patients with suspected infection and sepsis. Peripheral blood cultures are generally used for investigating the infectious aetiology of sepsis and for managing appropriate antimicrobial treatment as described elsewhere by the authors. The level of D-Dimer can be high if there is a large clot, or it can be high when the body is producing many tiny clots, as can happen in sepsis. It is one of the indicators to check for blood clotting problems. D-Dimer levels varied from 250 to 1000 mg in sepsis patients. With regards to PCT and DD results, observation of the present study confirmed that there was no correlation between PCT and DD with the period of patients stay in hospital.
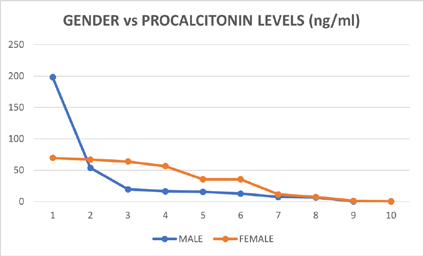
The data obtained showed that procalcitonin level was less than 0.5 µg/L and is an indicator to suspect that there is an infection. Procalcitonin level between 0.5-2 µg/L can indicate the possibility of a systemic infection. Whereas, procalcitonin levels of 2-10 µg/L indicate that sepsis is likely the cause and procalcitonin level of 10 µg/L or greater indicates a very high possibility of severe sepsis leading to septic shock. Data evidences showed that women and men could have different normal values however men have a higher value. In current study, the procalcitonin levels varied from 0.42 to 69.73 ng/ml, indicating a higher severity of bacterial infection in sepsis patients.
The baseline characteristics of patients were recorded and the origins of sepsis were identified by organs affected, as summarized in Table -9. This study showed that the aetiology of the patients admitted with sepsis had no common symptoms and no common history at the time of admission however gross differences between male and female patients could be observed as shown in Table 9a & 9b.
| Male Patient Sample | Male Patient’s age (Years) | Blood Pressure mm/hg | Heart rate | Pulse | Respiration | Past History |
|---|---|---|---|---|---|---|
| MP-01 | 70 | 95/60 | 72/min | 149/min | 20/min | smoker since 20 years, Fever, cough short ness of breath, chest pain, Dysuria |
| MP-02 | 65 | 140/90 | 120/bpm | 80/min | 28/min | Type 2 diabetes, hypertension, Fever, short ness of breath, right leg pain with oedema, hypo –glycemia |
| MP-03 | 62 | 140/90 | 66/bpm | 76/min | 24/min | Diabetes, hypertension, gutka chewer, Headache, giddiness, Vomiting, Left-hand weakness |
| MP-04 | 62 | 100/60 | 98/bpm | 78/min | 16/min | Type 2 diabetes, Hypertension, chronic kidney disease, Hyperglycaemia, Vomiting |
| MP-05 | 56 | 160/90 | 75/bpm | 103/min | 18/min | Hypertension, Seizures hemiparesis, slurred speech |
| MP-06 | 63 | 110/70 | 110/bpm | 80/min | 24/min | Diabetic cholestasis, Fever, Abdominal -distension, nausea |
| MP-07 | 53 | 110 /70 | 70 /bpm | 60 /min | 22 /min | Chronic airway disease, Diabetes, Hypertension, Aspiration pneumonia, Short ness of breath, Acute pulmonary edema, Urinary tract infection |
| MP-08 | 71 | 140/90 | 72/bpm | 100/min | 24/min | Hypertension, diabetes, severe shortness of breath, weakness of all 4 limbs. |
| MP-09 | 80 | 180/90 | 80/bpm | 90/min | 35/min | Alcoholic, Type 2 diabetes, hypertension, Aphasia right sided weakness in limbs. |
| MP-10 | 58 | 130/90 | 95/bpm | 75/min | 20/min | Hypertension, chronic smoker, chronic alcoholic, fever, shortness of breath cough with sputum |
Table 9(a): Male Patient’s aetiology: physical condition, symptoms and past history.
| Female Patient Sample | Female Patient’s age (Years) | Blood Pressure mm/hg | Heart rate | Pulse | Respiration | Past History |
|---|---|---|---|---|---|---|
| FP-11 | 45 | 110/82 | 72/bpm | 78/min | 14/min | Fever, cough head ache, bleeding from gums, Anaemia, Haematuria, pain in right hypochondrium |
| FP-12 | 56 | 130/80 | 76/bpm | 92/min | 16/min | Hypertension and diabetic since 10 years, Fever, short ness of breath, back ache, pain in the right pelvic region |
| FP-13 | 63 | 140/90 | 96/bpm | 80/min | 28/min | Type 2 diabetes, chronic kidney disease, Fever, shortness of breath, racoon’s eye, facial oedema eye pain, hematoma, pain in legs |
| FP-14 | 75 | 80/60 | 96/bpm | 76/min | 14/min | spine surgery, diabetic since 20 yrs and Hypertension since 5 years, Cough, loose stools, swelling on hands, vomiting, giddiness |
| FP-15 | 62 | 112/80 | 105/ bpm | 72/min | 22/min | Diabetes, Hypertension, Fever, Cough, Shortness of breath, Chest pain, vomiting |
| FP-16 | 60 | 120/70 | 72/bpm | 80/min | 20/min | Diabetes, hypertension, Chronic obstructive pulmonary disease, Short ness of breath, hyperglycaemia |
| FP-17 | 73 | 100/60 | 98/bpm | 76/min | 13/min | Hypertension since 10 yrs., Diabetes since 30 yrs, cholecystectomy 2 yrs back, Hernia 2 yrs back, Shortness of breath, Giddiness, Hypotension, Blood in stool |
| FP-18 | 65 | 90/50 | 81/bpm | 80 /min | 25 /min | Acute kidney infection, Fever, Shortness of breath, Hypotension, Loose stools and vomiting |
| FP-19 | 21 | 110/70 | 80/bpm | 115/min | 31/min | Fever, shortness of breath and abdominal pain. |
Table 9(b): Female Patient’s Aetiology: Physical condition, Symptoms and Past history.
These biochemical parameters, when combined with clinical assessment and other biomarkers, provided valuable information for the diagnosis and prognosis of sepsis. Monitoring these parameters helped in early identification of organ dysfunction, useful for guiding treatment decisions, and improving patient outcomes.
Gender Difference in the Various Parameters Tested
Male sex is a well-known possible risk factor for sepsis
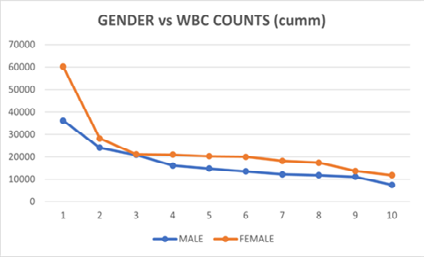
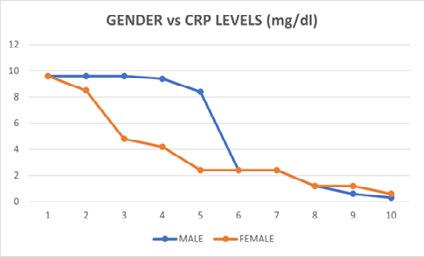
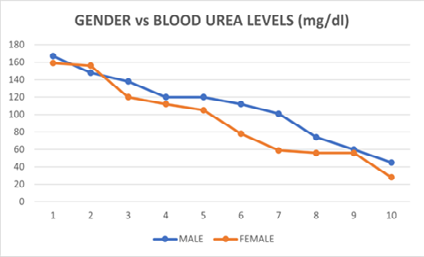
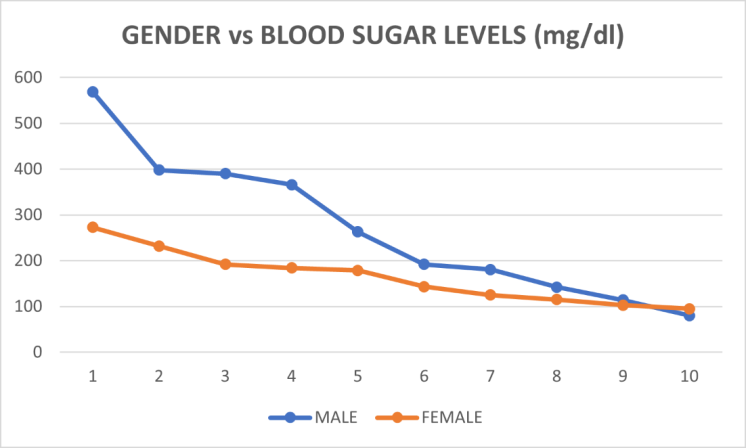
and septic shock. The results did not show any significant difference between male and female patients with respect to their WBC and urea levels. However, there was significant variation in blood sugar levels between the sexes as shown in Figure 1. Difference in CRP and PCT were also found to be significantly different between the sexes. Sepsis occurs more frequently in men, with an annual relative risk 1.3 times higher than in women. Additionally, among septic shock patients admitted to CCUs, males were more prevalent than females.
Understanding these sex-related differences is crucial for tailoring sepsis diagnosis, treatment, and management to improve outcomes for both men and women. It was observed from the results presented in Figure 4 which showed that there was a difference in gender versus biochemical parameters of sepsis patients. Further analysis on the gender difference in biochemical parameters are also presented in tables 10and 11. This data also confirms our belief that the difference between the sexes is to be marked as important and their affects could impact treatment strategies. The gender difference between the various biomarkers such as CRP and PCT, and blood chemistries, such as WBC’s, Urea and Sugar levels in sepsis patients are presented in Tables 10 & 11. In order to investigate the gender difference a Simple Linear Regression were performed.
| Male Patient Sl. No. | Male Patients’ BLOOD SUGAR (mg/dl) | Female Patient Sl No | Female Patients’ BLOOD SUGAR (mg/dl) |
|---|---|---|---|
| 1 | 181 | 11 | 125 |
| 2 | 125 | 12 | 179 |
| 3 | 179 | 13 | 232 |
| 4 | 390 | 14 | 184 |
| 5 | 184 | 15 | 115 |
| 6 | 263 | 16 | 273 |
| 7 | 366 | 17 | 192 |
| 8 | 115 | 18 | 103 |
| 9 | 142 | 19 | 95 |
| 10 | 80 | 20 | 143 |
Table 11: Male Patients’ Blood Sugar VS Female Patients’ Blood Sugar.
Simple Linear Regression Regression Line Female Patients’ Blood Sugar (Mg/Dl) = 0.2619. Male Patients’ Blood Sugar (Mg/Dl) + 111.0612 Correlation: r = 0.4705; whereas R-squared: r2=0.2213
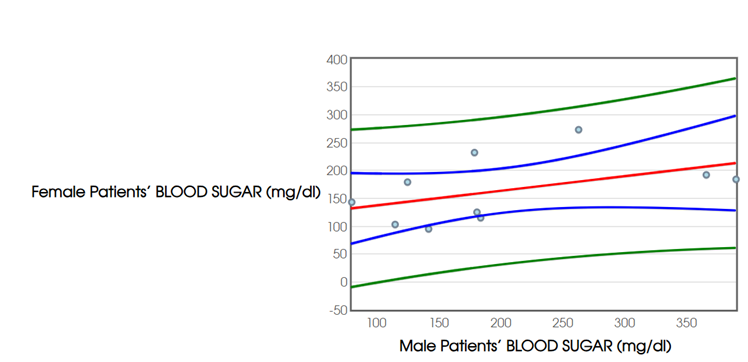
Regression Inference: y=α+βx𝑦=𝛼+𝛽𝑥. Whereas, Degrees of Freedom: 𝑑𝑓 = 𝑛−2 = 88; Estimate of Slope: b=0.2619; Standard Error Slope: SEb=0.1737; Regression Standard Error: s=54.7165; 𝑡-Statistic: t=1.5079; 95% Confidence Interval for 𝛽: (−0.1386,0.6625); p-value=0.17.
Interpretation for Male Patients’ Blood Sugar VS Female Patients’ Blood Sugar
Assuming that the True slope is β = 0, the probability of seeing a test statistic as far out as t =1.5079 is 0.17.That is, assuming that there is no straight-line relationship between MALE PATIENTS BLOOD SUGAR (mg/dl) and FEMALE PATIENTS BLOOD SUGAR (mg/dl), 17% of all similarly collected samples would have a test statistic as far away from 0 as t = 1.5079.Hence, suggest to keep the null hypothesis. (0.17 = p-value ≥ α =0.05)
| Male Patients Sl no | Male Patients’ BLOOD UREA (mg/dl) | Female Patients Sl no. | Female Patients’ BLOOD UREA (mg/dl) |
|---|---|---|---|
| 1 | 148 | 11 | 56 |
| 2 | 56 | 12 | 59 |
| 3 | 59 | 13 | 156 |
| 4 | 138 | 14 | 159 |
| 5 | 159 | 15 | 105 |
| 6 | 101 | 16 | 112 |
| 7 | 167 | 17 | 120 |
| 8 | 105 | 18 | 78 |
| 9 | 45 | 19 | 56 |
| 10 | 120 | 20 | 28 |
Table 12: Male Patients’ Blood Urea VS Female Patients’ Blood Urea.
Simple Linear Regression Regression Line Female Patients’ Blood Urea (Mg/Dl) = 0.1599. Male Patients’ Blood Urea (Mg/Dl) + 75.34 Correlation: r = 0.1596; whereas R-squared: r2 = 0.0255
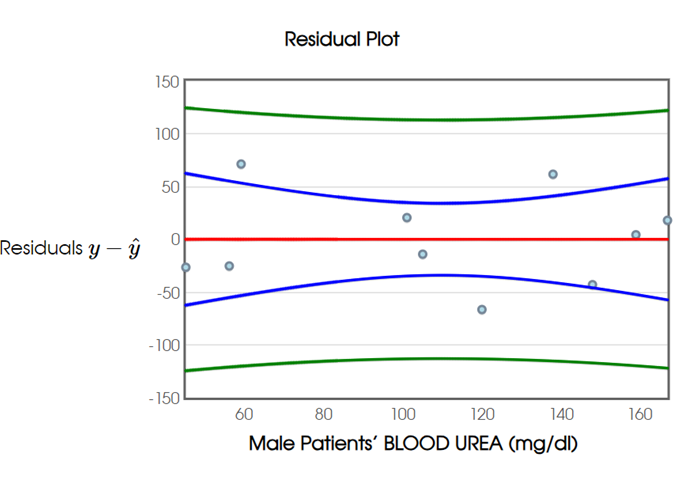
Regression Inference: y=α+βx𝑦=𝛼+𝛽𝑥. Where, Degrees of Freedom: 𝑑𝑓=𝑛−2=88; Estimate of Slope: 𝑏=0.1599; Standard Error Slope: SE𝑏=0.3498; Regression Standard Error: 𝑠=46.6998; 𝑡-Statistic: 𝑡=0.4572; 95% Confidence Interval for 𝛽: (−0.6467,0.9665); p-value=0.6597
Interpretation for Male Patients’ Blood Urea VS Female Patients’ Blood Urea
Assuming that the true slope is β = 0, the probability of seeing a test statistic as far out as t =0.4572 is 0.6597.That is, assuming that there is no straight-line relationship between Male Patients’ Blood Urea (mg/dl) and Female Patients’ Blood Urea (mg/dl), 66 % of all similarly collected samples would have a test statistic as far away from 0 as t =0.4572. Hence, suggest keeping the null hypothesis. (0.6597 = p-value ≥ α = 0.05).
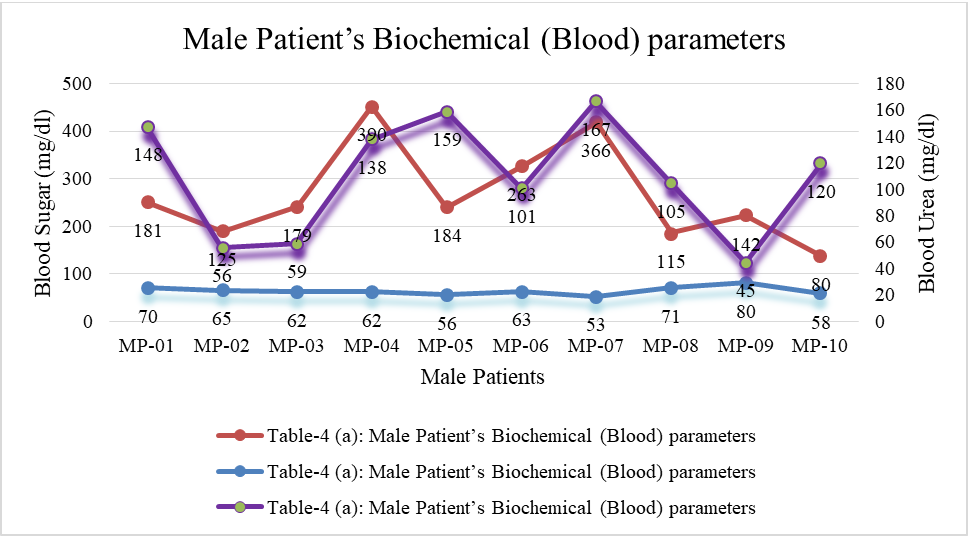
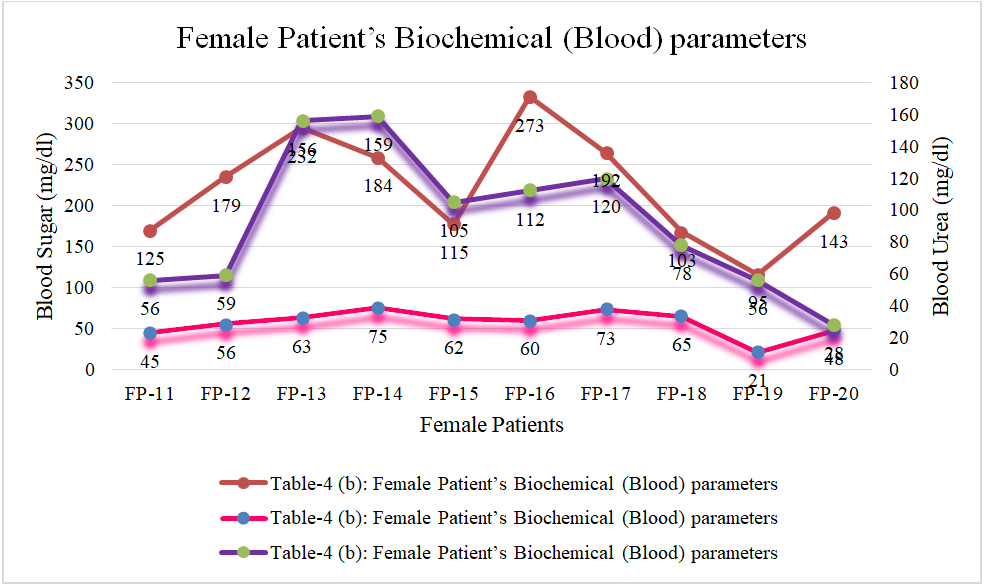
Additionally, Male Patient’s Biochemical (Blood) parameters (Figure 5) and Female Patient’s Biochemical (Blood) parameters (Figure 6) were individually analyzed and presented. These show the impediments are related to age group and gender based.
Sepsis, a life-threatening condition is marked by a dysregulated pathological condition. The above data shows that the sugar levels in blood and urine of sepsis patients were much high when compared to controls. Further there is vast significant difference between the male and female patients. Thus, remains a pressing global healthcare challenge characterized by high mortality rates and significant economic consequences.
Discussion
Sepsis is a life-threatening condition characterized by a dysregulated immune response to infection, leading to organ dysfunction and potentially death. Accurate and timely diagnosis and prognosis are crucial for effective management.
Our findings are consistent with previous studies that have emphasized the demographic characteristics of sepsis patients. Similar study reported a median age of 69 among adult sepsis patients, where 52% were males and their median hospital stay was of 9 days [23]. Another study found that total sepsis cases had a mean age of 65 years (SD ±18.1), with 50.8% of the patients being female [24]. These findings align with the present study, where 60% of the patients were in the age group between 60-80 years, emphasizing the severe impact of sepsis on elderly patients.
Symptoms of Patients Upon Admission to the Hospital
However, another study reported that the mean duration of signs and symptoms starts prior to hospitalization for sepsis was 4.1 ± 1.8 days; nevertheless, the starting time showed a bimodal distribution. A significant proportion of patients with symptoms such as pain, dyspnea, weakness, cough, and hypertension experienced a subacute onset. In contrast, symptoms with a higher proportion of patients reported acute onset (within 7 days) included altered mental status (82.8%), fever (85.3%), nausea (84.4%), vomiting (86.8%), and chills (85.8%) [25].
Comorbidity of Sepsis Patients
At the time of hospital admission, it is crucial to consider co-morbidities issues, as they can significantly impact patient outcomes. In the present study, 70% of patients were hypertensive, and 65% Diabetics. This was consistent with previous findings, where nearly 97% of sepsis patients had atleast one comorbidity while 35% had diabetes mellitus, 32% had cardiovascular disease (including coronary artery disease, peripheral vascular disease, or congestive heart failure), 23% had chronic kidney disease, and 20% had chronic obstructive pulmonary disease. Likewise, other research studies have also reported that 55.5% to 65% of sepsis patients had underlying comorbidities [26, 27]. Certainly, chronic diseases may impact sepsis outcomes, assessing pre-existing comorbidities which is crucial for improving mortality predictions [28]. The most common illnesses leading to sepsis include pneumonia (35%), urinary tract infections (25%), gastrointestinal infections (11%), and skin/soft tissue infections (11%). Pathogens were isolated from blood cultures in 30% patients and from urine cultures of 28%, as these groups were not mutually exclusive [23]. Our study was closely similar with these findings, as 40% of sepsis patients had urinary tract infection.
It is important to mention here that their cytohistologic studies can be projected only in murine or animal models. This study was strictly monitored by the rules and regulation of the Ethical guidelines, and patients’ information were regarded as highly confidential.
Previous epidemiological studies have observed that chronic comorbid conditions, such as end-stage renal disease, malignancy, liver cirrhosis were associated with an increased risk of sepsis and sepsis-related mortality [29]. However, comprehensive analysis using significant epidemiological data are still limited, highlighting the necessity for further research on the prevalence and outcomes of several common comorbidities in sepsis patients using a nationwide magnitude of epidemiologic data.
Role of Biomarkers
Biomarkers play a pivotal role in grading sepsis, assisting in the differentiation between sepsis, severe sepsis, and septic shock, and thereby improving patient outcomes. They are essential for early diagnosis, severity assessment, and prognosis. Biomarkers help assess the severity of the condition, monitor the progression of the disease, and guide treatment decisions. In our study we have determined protein biomarkers which are very widely used. However, there are some other biomarkers associated with sepsis:(i) Elevated lactate levels in the blood indicate tissue hypoperfusion and anaerobic metabolism, which can occur in sepsis due to impaired oxygen delivery to tissues. (ii) High IL-6and Elevated TNF-α levels are indicative of severe sepsis and can be used to monitor the progression of the disease. (iii) HMGB1, suPAR and IL-8 can provide insight into the inflammatory and immune response and may predict the severity and outcome of the condition.
While no single biomarker is definitive, a combination of these markers, along with clinical signs and symptoms, helps in diagnosing sepsis, to assess its severity, and guide treatment.
Traditional biomarkers such as C-Reactive Protein (CRP), procalcitonin (PCT), and D-Dimer (DD), along with emerging biomarkers like presepsin, interleukin-6 (IL-6), and Pancreatic Stone Protein (PSP), provide valuable information that enhances patient management and treatment strategies. Hence our studies were based on the three important biomarkers (PCT, CRP and D-D). Integrating these biomarkers into clinical practice along with other diagnostic tools, can significantly enhance the accuracy of sepsis diagnosis and prognosis, ultimately leading to improved patient care. In this study, sepsis diagnosis was performed using laboratory- based methods following standard protocols. Recently, an increasing number of studies have focused on evaluation and prognosis of sepsis using specific biomarkers [9]. These studies have demonstrated that procalcitonin (PCT) can serve as an effective indicator of infection severity, and have confirmed its suitability as a key biomarker in the diagnosis of sepsis [10].
Serum C-reactive protein (CRP) is an acute-phase protein synthesized exclusively in the liver in response to cytokines, particularly interleukin-6 (IL-6). CRP levels begin to raise 4–6 hrs. after an inflammatory stimulus, doubling every 8 hours, peaking at 36–50 hours, and having a half-life of 19 hours [30]. Our study demonstrated a strong positive correlation between PCT and CRP which a correlation reaching 90%. An 85% rise in PCT further suggests that this protein can be a very useful biomarker for sepsis. Whereas, the CRP levels in our sepsis patients ranged from 0.60 to 9.60 mg/dl.
A similar finding was observed in a study of community- acquired bloodstream infections (BSI), where CRP concentration begins to rise in the three days leading up to a definitive diagnosis of bloodstream infections [31]. However, in a prospective observational study assessing the performance of 53 biomarkers in the discrimination between sepsis and non-septic systemic inflammatory response syndrome (SIRS) it was found that no biomarker or combination performed better than CRP alone, and better than PCT [32].
Procalcitonin is a prohormone that serves as a precursor to calcitonin. PCT is produced by nearly all organs and macrophages, with its levels starting to increase at 3–4 hours after an inflammatory stimulus, peaking around 24 hours and having a half-life of 22–35 hours [33]. In our current study, procalcitonin level were found to be less than 0.5 µg/L with variations ranging from 0.42 to 69.73 ng/ml, this indicates the degree of severity of the infection in sepsis patients.
However, previous study stated that a clinical approach algorithm based on the concept of “alert PCT” (PCT ≥ 1 ng/mL and not decreasing more than 10% per day) in a randomized controlled trial (RCT). This approach showed no mortality benefit but was associated with increased consumption of broad-spectrum antibiotics, more days on antibiotics, prolonged mechanical ventilation and extended ICU stays [31].
PCT clearance within the first 24 and 48 hours has proven to be good and suitable prognostic tool in monitoring sepsis. Some previous studies just measured the PCT randomly found no significant correlation with clinical cases. On the other hand, studies that assessed serum PCT levels serially demonstrated significant changes in PCT level among sepsis patients. Our study concludes that the PCT, D-dimer and CRP levels are effective biomarkers for predicting and monitoring the prognosis including mortality in sepsis patients. Although CRP is not a specific biomarker but it plays a vital role in the monitoring of bacterial infection, inflammation tissue injury and recovery. In contrast, significantly rise in the PCT levels in the third and fourth weeks were observed in the group of patients who did not survive [28]. Our present study concluded that PCT is a good prognostic biomarker for mortality in sepsis.
D-dimer, a biomarker that can be rapidly analysed at low cost and widely available, also appears to be a valuable tool in reflecting the dysregulated host response in sepsis patients. The sequential organ failure assessment (SOFA) score is used to quantify the number of failed organs and severity of the sepsis cases, this remains a key tool in clinical practice. The recent investigations have expressed the role of biomarkers in providing biological insights and predicting a clinically relevant outcomes for the diagnostic and prognostic assessment of sepsis. However, no current clinical measure or parameter fully captures the concept of “dysregulated host response”.
The patient’s medical records revealed the significant variations in the symptoms of the sepsis. The results showed that many patients were immune-suppressed and several had diabetic conditions, as indicated by their varying WBC count, fluctuating blood and urine sugar levels. Therefore, this vast heterogeneity in patient profiles suggests that treatment was personalized to each individual case.
Several biomarkers indicating a strong fibrinolytic shutdown, including low D-dimer levels, they were found to be associated with a reduced survival rates in patients with sepsis. In fact, nearly all patients admitted with sepsis had elevated D-dimer levels, which were very closely related to organ dysfunction. As sepsis progresses, it can severely impaired blood flow to vital organs such as the heart, brain and kidney, leading to their dysfunction. Sepsis is also a common cause of abnormal blood clotting, resulting in burst of blood vessels or small clots that damage or destroy tissues. This often leads to complications including permanent brain damage, tissue damage or death. Additionally, sepsis can cause kidney failure, permanent lung damage due to mechanical ventilation and damage to the heart valve.
Biomarkers have been shown to improve infection diagnosis, help in early risk stratification and provide prognostic information which helps to optimize therapeutic decisions particular in the context of antibiotic stewardship. In this context, the use of the blood infection marker procalcitonin (PCT) has gained significant attention. While, there is still no gold standard for the detection of sepsis and conventional diagnostic approaches have limitations. Therefore, additional tests like PCT are necessary to enable early and reliable diagnosis. PCT has strong discriminatory properties, effectively differentiate between bacterial and viral infections with rapidly available results. Additionally, PCT contributes to risk stratification and prognostication, which can influence the appropriate use of healthcare resources and therapeutic options. Monitoring PCT kinetics over time also improves the management of critically ill sepsis patients and aiding in decisions regarding the de- escalation of antibiotics. Importantly, PCT plays a key role in guiding antibiotic use in patients with respiratory infection and sepsis, helping to limit unnecessary limiting initiation and shortening treatment duration. To date, PCT is the best studied biomarker in relation to antibiotic stewardship. However, further research is needed to determine the optimal use of PCT, particularly in combination with other remerging diagnostic tests to achieve the most efficient sepsis care.
We found that procalcitonin is a useful marker for diagnosis of sepsis in critically ill patients. However, it cannot be relied upon as the single definitive test for sepsis diagnosis, but rather it must be interpreted in context with information from careful medical history, physical examination, and when feasible, microbiological assessment. Moreover, continuing re-evaluation throughout the course of the disease is advisable to ensure accurate diagnosis and effective treatment.
Age and Gender Difference
Despite advancements in sepsis detection and treatment, sepsis remains a major cause of morbidity and mortality for the majority of people with sepsis. The annual occurrence of sepsis varies significantly, ranging from 3x102 - 103 cases per 1x105people. Most sepsis patients are admitted to hospitals and present with a complex aetiology with an increasing frequency especially among the elderly [22, 23]. Our data indicate that the majority of sepsis patients were over the age of 50. Their demographic and health conditions were summarized in tables. Our data showed that the patients had shortness of breath and high fever at the time of their admission to the CCU in the Hospital. Cough and vomiting sensation were common in these patients. Sepsis decreases circulating platelets and adversely affects haemostatic function by maintaining adhesion molecule expression and secretion capability, and modulates growth factor production. These observations suggest that sepsis alters the haemostatic function of the platelets. Patients with severe sepsis have lower platelet count, higher MPV, and increased PDW [24]. Our findings are in accordance with these observations. The typical platelet count in adults is 15x104 – 45x 104 (μL) of blood. Our study proposed that patients who died from organ failure and sepsis were significantly older than those who survived. It is obvious that elderly patients have more comorbidities compared to younger ones. Therefore, they are more susceptible to mortalities and morbidities caused by organ failures in septic shock.
Our study observed significant difference between male and female patients in terms of blood sugar and blood urea levels. Correspondingly, our data reported that these differences are important and could potentially impact treatment strategies. Another study emphasized that, sepsis and septic shock are known risk factors more prevalent in males with an annual relative risk of 1.3 times that of females [27]. Gender-based differences in regards to symptoms, illness presentation, or diagnostic bias may contribute to variations in hospital mortality and infection site differences as well [34, 35].
Conclusion
Sepsis is a major cause of morbidity and mortality in patients admitted to the intensive care unit (ICU).In these case studies we found that sepsis patients had significantly higher levels of WBC, C-reactive (CRP), procalcitonin (PCT), and D-Dimer levels. Both low and extremely elevated DD values are associated with higher risk of death. The protein biomarkers which we studied are recommended as important for detecting early the sepsis cases and organ failure conditions. Hence it can be concluded that DD value may be an independent prognostic factor for in-hospital mortality in sepsis patients, and its prognostic accuracy is influenced by vasopressor therapy and WBC count. The differences between sexes in various parameters analyzed in sepsis patients, such as Procalcitonin (PCT), C-Reactive Protein (CRP), and D-dimer, can be attributed to several biological and physiological factors between the sexes.
Other tests, including CBC and chemistries, provide a baseline to assess therapeutic response. The biomarkers study showed much variations in all the parameters indicating the patient heterogeneity due to various co- morbid conditions. It was found that the clinical application of PCT combined with DD and CRP are valuable in predicting the severity of sepsis therefore, its worthy of further study and application.
Declarations
Acknowledgements
We are thankful to the Chairman and Research Directors of Mahavir Hospital, Hyderabad for their encouragement and support. We acknowledge the help of Dr. Majid Mohiuddin, HOD of Microbiology, Anwarul Uloom College, Hyderabad for his help in statistical analysis and valuable suggestions.
Conflict of Interest
The authors declare that they have no conflict of interests regarding the publication of this paper. Ethics committee Approval: this project was approved by the Institutional Ethics committee (IEC) of BMMRC
Financial Support
No funds were received for this project from any sources.
References
-
WHO (2020) Global Report on the Epidemiology and Burden of Sepsis: Current Evidence, Identifying Gaps and Future Directions, pp: 55.
-
WHO (2020) Calls for Global Action on Sepsis - Cause of 1 in 5 Deaths Worldwide.
-
Chaitanya N, Jamil K, Zahid MAA (2023) Confronting Sepsis: A Call for Urgent Action. European Journal of Pharmaceutical and Medical Research 10(7): 200-202.
-
Gyawali B, Ramakrishna K, Dhamoon AS (2019) Sepsis: The Evolution in Definition, Pathophysiology, and Management. SAGE Open Medicine 7: 1-13.
-
Kalil AC, Opal SM (2015) Sepsis in the Severely Immunocompromised Patient. Curr Infect Dis Rep 17(6): 487.
-
Stearns-Kurosawa DJ, Osuchowski MF, Valentine C, Kurosawa S, Remick DG (2011) The Pathogenesis of Sepsis. Annu Rev Pathol 6: 19-48.
-
Jarczak D, Kluge S, Nierhaus A (2021) Sepsis- Pathophysiology and Therapeutic Concepts. Front Med (Lausanne) 8: 628302.
-
Zehnbauer BA, Freeman BD, Buchman TG (1999) Genetic Predisposition to Sepsis and Organ Failure. Sepsis and Organ Dysfunction pp: 49-53.
-
Evans T (2018) Diagnosis and Management of Sepsis. Clin Med (Lond) 18(2): 146-149.
-
Duncan CF, Youngstein T, Kirrane MD, Lonsdale DO (2021) Diagnostic Challenges in Sepsis. Curr Infect Dis Rep 23(12): 22.
-
Choe EA, Shin TG, Jo IJ, Hwang SY, Lee TR, et al. (2016) The Prevalence and Clinical Significance of Low Procalcitonin Levels among Patients With Severe Sepsis or Septic Shock in the Emergency Department. Shock 46(1): 37-43.
-
Kinasewitz GT, Yan SB, Basson B, Comp P, Russell JA, et al. (2004) Universal Changes in Biomarkers of Coagulation and Inflammation Occur in Patients with Severe Sepsis, Regardless of Causative Micro-Organism. Crit Care 8(2): R82-90.
-
Becker KL, Snider R, Nylen ES (2008) Procalcitonin Assay in Systemic Inflammation, Infection, and Sepsis: Clinical Utility and Limitations. Crit Care Med 36(3): 941-952.
-
Nakamura A, Wada H, Ikejiri M, Hatada T, Sakurai H, et al. (2009) Efficacy of Procalcitonin in the Early Diagnosis of Bacterial Infections in a Critical Care Unit. Shock 31(6): 586-591.
-
Dolatabadi AA, Memary E, Amini A, Shojaee M, Abdalvand A, et al. (2015) Efficacy of Measuring Procalcitonin Levels in Determination of Prognosis and Early Diagnosis of Bacterial Resistance in Sepsis. Niger Med J 56(1): 17-22.
-
Krüger S, Ewig S, Marre R, Papassotiriou J, Richter K, et al. (2008) Procalcitonin Predicts Patients at Low Risk of Death from Community-Acquired Pneumonia Across All CRB-65 Classes. Eur Respir J 31(2): 349-355.
-
Kim MH, Choi JH (2020) An Update on Sepsis Biomarkers. Infect Chemother 52(1): 1-18.
-
Bürgi W, Briner M, Franken N, Kessler AC (1988) One- Step Sandwich Enzyme Immunoassay for Insulin using Monoclonal Antibodies. Clin Biochem 21(5): 311-314.
-
Ridker PM, Rifai N, Clearfield M, Downs JR, Weis SE, et al. (2001) Measurement of C- Reactive Protein for the Targeting of Statin Therapy in the Primary Prevention of Acute Coronary Events. N Engl J Med 344(26): 1959- 1965.
-
Rifai N, Tracy RP, Ridker PM (1999) Clinical Efficacy of an Automated High-Sensitivity C- Reactive Protein Assay. Clin Chem 45(12): 2136-2141.
-
Liu S, Yang G, Tian J, Qu D, Wang Q (2020) The Correlation between Procalcitonin and D-Dimer and the Prognoses of Emergency Sepsis Patients. Int J Clin Exp Med 13(2): 1002-1007.
-
Amaral A, Opal SM, Vincent JL (2004) Coagulation in Sepsis. Intensive Care Medicine 30(6): 1032-1040.
-
Novosad SA, Sapiano MR, Grigg C, Lake J, Robyn M, et al. (2016) Vital Signs: Epidemiology of Sepsis: Prevalence of Health Care Factors and Opportunities for Prevention. MMWR Morb Mortal Wkly Rep 65(33): 864-869.
-
Paoli CJ, Reynolds MA, Sinha M, Gitlin M, Crouser E (2018) Epidemiology and Costs of Sepsis in the United States- An Analysis Based on Timing of Diagnosis and Severity Level. Critical Care Medicine 46(12): 1889-1897.
-
Liu VX, Bhimarao M, Greene JD, Manickam RN, Martinez A, et al. (2021) The Presentation, Pace, and Profile of Infection and Sepsis Patients Hospitalized Through the Emergency Department: An Exploratory Analysis. Crit Care Explor 3(3): e0344.
-
Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, et al. (2001) Epidemiology of Severe Sepsis in the United States: Analysis of Incidence, Outcome, and Associated Costs of Care. Crit Care Med 29(7): 1303- 1310.
-
Martin GS, Mannino DM, Eaton S, Moss M (2003) The Epidemiology of Sepsis in the United States from 1979 through 2000. N Engl J Med 348(16): 1546-1554.
-
Pittet D, Thiévent B, Wenzel RP, Li N, Gurman G, et al. (1993) Importance of Pre-Existing Co-Morbidities for Prognosis of Septicemia in Critically Ill Patients. Intensive Care Med 19(5): 265-272.
-
Arulkumaran N, Annear NM, Singer M (2013) Patients with End-Stage Renal Disease Admitted to the Intensive Care Unit: Systematic Review. Br J Anaesth 110(1): 13- 20.
-
Povoa P, Salluh JI (2012) Biomarker-Guided Antibiotic Therapy in Adult Critically Ill Patients: A Critical Review. Ann Intensive Care 2: 32.
-
Garvik OS, Povoa P, Magnussen B, et al. (2020) C-Reactive Protein and Albumin Kinetics before Community- Acquired Bloodstream Infections-A Danish Population- Based Cohort Study. Epidemiol Infect 148: e38.
-
Parlato M, Philippart F, Rouquette A, et al. (2018) Circulating Biomarkers May be Unable to Detect Infection at the Early Phase of Sepsis in ICU Patients: The CAPTAIN Prospective Multicenter Cohort Study. Intensive Care Med 44: 1061-1070.
-
Reinhart K, Karzai W, Meisner M (2000) Procalcitonin as a Marker of the Systemic Inflammatory Response to Infection. Intensive Care Med 26(9): 1193-1200.
-
Lee OY, Mayer EA, Schmulson M, Chang L, Naliboff B (2001) Gender-Related Differences in IBS Symptoms. Am J Gastroenterol 96(7): 2184-2193.
-
Samsudin I and Vasikaran SD. Clinical Utility and Measurement of Procalcitonin. Clin Biochem Rev. 2017 Apr; 38(2):59-68. PMID: 29332972; PMCID: PMC5759088.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells