An Overview of Anti-diabetic Efficacy and Biochemical Mechanism of Anisomeles Malabarica (Malabar Catmint): A Review
Diabetes mellitus (DM), which affects a substantial portion of the population and has become more common in modern society, is actually a metabolic condition. The hallmark of diabetes mellitus is excessively high blood sugar levels brought on by a breakdown in glucose homeostasis brought on by a partial or complete lack of insulin in the body or by insulin activity. Hyperglycaemia is caused by changes in insulin levels or activity as well as cell activities that affect the biochemical processes involved in the metabolism of carbohydrates, proteins, and lipids in target organs like the liver function. skeletal muscle, kidney, and adipose tissue. 1.5 million deaths per year are attributed to diabetes, and 48 percent of these fatalities occurring before the age of 70. Premature mortality from diabetes increased by 5% between the years 2000 and 2016. Therefore, it's essential to pick the appropriate diabetic therapy. Professional anti-diabetic medications are available to treat diabetes, however there are significant concerns over their cost and side effects. The drawbacks of currently available drugs necessitate the development of new, less expensive, and safer remedies. While Anisomeles malabarica (A. malabarica), an indigenous medicinal plant, has been shown to have anti-epileptic, anti-diabetic, anti-proliferative, and other qualities, the focus of this review is on AM's anti-diabetic advantages.
Introduction
As per the Diabetes Association, there are 425 million diabetics throughout the planet, with that number estimated to rise to 629 million by 2045 [1]. Diabetes is a disorder in which high blood sugar levels occur as a consequence of a disturbance in glucose homeostasis caused by a problem such as loss of insulin level and insulin action. Changes in insulin levels and/or activity, as well as changes in ß - cell activities, all affect carbohydrate, protein and lipid metabolic biological pathways in various organs such the liver, skeletal muscle, kidney, and adipose tissues, resulting in hyperglycaemia. Glycaemic control and fasting are two incredibly complex and important systems that regulate metabolism in the hepatocytes and peripheral tissues, and both are important in metabolic disorders [2]. Insulin dependency is a complication of type 1 diabetes mellitus, which occurs when the pancreas produces little or no insulin, necessitating the use of an insulin injections supply. Overweight and insufficient physical activity are common causes of type
2 diabetes, which leads to insulin resistance and reduced natural insulin production as the illness advances. DM is caused by a lack of glycemic control, and insulin is required to regulate and utilize glucose from blood to the targeted cells. Continuing to have unusually high glucose levels causes long-term, permanent harm to the human body. Neuropathy and a therosclerosis are two well-known side consequences of persistently elevated glucose levels in blood. End organ damage results, ranging from skin infections, coronary artery disease, and strokes to microvascular consequences such as peripheral neuropathies, diabetic nephropathy, and retinopathies [3, 4]. Drowsiness, hunger, thirst, headaches, impaired vision, frequent urination, discomfort or tingling sensations, loss of weight, and skin infections are all signs of diabetes mellitus. Randomized or fasting blood sugar readings, as well as glycosylated haemoglobin (HbA1c) values, are used to make the diagnosis. Patients are educated on the significance of nutrition, workout, and weight reduction (if relevant) after being diagnosed, and most are ultimately put on medication. Insulin treatment is the very first therapy for people with type 1 diabetes, although the pharmacological choices for patients with type 2 diabetes are significantly wider, encompassing insulin treatment. An HbA1c of more than 6.5 percent, a fasting plasma glucose measurement of more above than 6.9 mmol/L, or a random blood glucose value of more than 11 mmol/L are all used to diagnose diabetes. Glycated hemoglobin values are often used as a reference for glycemic management in diabetics, with a goal of lower than 7% for most individuals and a more flexible target of lower than 8% for older patients as well as those with impairments. Patients with type 1 diabetes are encouraged to monitor their glucose levels at home, including fasting and random blood glucose levels, to evaluate if insulin dosage changes are necessary [5, 6, 7, 8].
With the onset and development of DM, the activity of important governing carbohydrate metabolism involved enzymes in the glycolytic, gluconeogenic, and glycogenolytic processes varies substantially, culminating in chronic hyperglycemia [9]. In those with diabetes (either type 1 or type 2), and to a lesser degree in those with insulin resistance, chronic hyperglycemia causes oxidative stress. Reactive hypoglycemia oxidative stress is caused by a number of metabolic processes, including protein kinase C activation, glucose autooxidation, methylglyoxal production and glycation, sorbitol generation, hexosamine metabolism, and oxidative phosphorylation. The relationship between oxidative stress and diabetic complications has been explored extensively [10, 11, 12], including by our own research. Systemic hyperglycemia causes diabetic nephropathy, retinopathy, neuropathy, and cardiovascular complications. The most often used therapeutic medications in the treatment of diabetes mellitus include insulin, insulin secretagogues (Sulfonylureas), insulin sensitizers (Thiazolidinediones and Biguanides), non- secretagogues (Meglitinides), glycosurics, alpha-glucosidase inhibitors, and peptide analogues [13]. Excess weight, hypoglycemia, digestive disturbances, heart problems, anaemia, kidney ailment, oedema, raised LDL cholesterol and triglycerides (TG), and bladder cancer have all been reported as side effects. Additionally, these drugs are costly [14, 15] and as a consequence, people are moving to sustainable resources and complementary treatments, especially natural products, to assist them control diabetes-related comorbidity. Antihyperglycemic compounds derived from medicinal plants include flavonoids, terpenoids, proteins, glycosides, phenolics, alkaloids, and steroids [16, 17]. Medicinal herbs and organic ingredients have been proven in studies to restore glucose, protein metabolic enzymes, lipid, and improving glycemic control in diabetes patients [18, 19].
From classical era, traditional medicines and their formulations have been used in many traditional medical systems across the globe. Several research have been published on ethnomedicinal strategies to diabetes treatment and the use of natural chemicals obtained from plants. For example, before 1978, Bever and Zahnd investigated hypoglycemic plants [20]. In a similar manner, Atta-Ur-Rahman and Zaman collected a study of the literature on the anti-diabetic effects of 343 traditional medicines that have been used traditionally or have been shown to have a hypoglycemic impact in animal studies [21]. Another research discovered over 1,200 species across 183 families as well as 725 genera are used to treat diabetes symptoms in both conventional and experimental medicine. The most common families among them were Euphorbiaceae, Asteraceae, Fabaceae, Liliaceae, Lamiaceae, and Poaceae [22]. Anacardium occidentale, Momordica charantia, Allium sativum, Allium cepa, Aloe vera, Lupinus albus, Catharanthus roseus, Eucalyptus globules, Syzygium cumini, Tecoma stans, Trigonella foenum- graecum,Urtica dioica and a variety of other plants are used in various nations. Li, Zheng, et al. Looked studied 86 crude medicines utilised in Chinese Traditional Medicine to treat DM (82 crude plant medicines and 4 crude animal medicines) [23]. According to Simmonds and Howes, 656 flowering plants from 111 families and 437 species were used for diabetes therapy in the past [24]. Giovannini et al. looked at the use of 16 species of plants for diabetes therapy in 7 Central American countries, showing experimental evidence for their own use in traditional medicine [25]. Harlev, et al. investigated the traditional medicines used by ethnic groups residing in desert and semi-arid regions to treat diabetes [26]. Moradi, et al. investigated the anti- diabetic effectiveness and function of 30 commonly used medicinal plants to control diabetes [27]. Some other ethnobotanical and ethnopharmacological studies have shown the use of medicinal plants to cure DM. For example, Eddouks et al. discovered that indigenous Moroccans in the south-east region employed 37 medicinal herbs to treat diabetes [28]. Among the most often used plants were Artemisia herba-alba, Amni visnaga, and Trigonalla foeniculum-granum. Tag, et al. discovered 46 traditional medicines used by the ethnic communities of Arunachal Pradesh, in northeast India’s Himalayas, to cure DM [29]. Only a few natural products or mimic compounds have been approved as anti-diabetic medicines, despite hundreds of research on ethnopharmacology or anti-diabetic potential of herbal remedies or natural products. Metformin is the only anti-diabetic medication developed on the basis of galegine, a naturally occurring molecule present in plants Galega officinalis. Despite this, ethnopharmacological approaches, as well as the isolation and characterization of active constituents and their modes of action, are being applied in a rising number of research to produce effective anti-diabetic herbal medications [30].
Lamiaceae belonging medicinal plant Anisomeles malabarica is native to Asia’s tropical and subtropical zones. Anisomeles malabarica, usually known as “Malabarcatmint,” is a South Indian upright plant. Since the time of the ancient Indians, Chinese, Egyptians, and many other nations, medicinal plants have been significant components in traditional medicine and human diet [31, 32]. Medicinal plants are the primary source of care for the large percentage of people on the planet. Herbal teas, infusions, ointments, syrups, liniments, and powders were initially utilised in their basic forms as herbal forms [33]. With 60 percent of the world’s population, Asia is the largest continent. The Asian continent, as well as the islands in the Indian and Pacific Oceans, make up the region. Traditional medicine and a variety of species and aromatic plant have been used since antiquity [34]. Nevertheless, in many nations, the biodiversity of medicinal plant species has yet to be properly investigated. Labiatae, also known as the mint family, is a very popular medicinal plant family. With around 220 genera and nearly 4000 species world - wide, the Labiatae family (Lamiaceae) is among the largest and most unique flowering plant families. Herbs or shrubs having a fragrant scent make up this family of plants. They are widespread in Asia, the Maltese Islands, as well as other Mediterranean nations. The Labiatae family has a large number of members which are used in ancient times medicine. Mints, spearmint, tulsi, thyme, and coleus are examples of culinary and decorative plants [35]. The strong fragrant essential oil, saponins, tannins, and organic acids are all therapeutic components. Sedative, tonic, diuretic, antispasmodic, and antibacterial characteristics are all found in Labiatae plants. Various essential applications have been given for Anisomeles malabarica (A. malabarica). A. malabarica is a fragrant, highly pubescent perennial plant that grows to a height of 1-2 metres. Flowers are purple, in closely packed whorls of somewhat interrupted spikes; fruits are nutlets, carrying ellipsoid and compact seeds [36]. Leaves seem to be simple, opposite, really quite thick, fragrant, oblong-lanceolate, acute, and white below, pale above, crenate-serrate. Peimiratti, Malabarcatmint, Bhutan kusham, and Peyameratti are some of the plant’s common names. The taxonomic classification of A. malabarica Shown in Table 1.
| Division | Spermatophyta |
|---|---|
| Sub-division | Angiospermae |
| Class | Dicotyledone |
| Sub-class | Gamopetalae |
| Series | Bicarpellate |
| Order | Lamiales |
| Family | Lamiaceae or Labiatae |
| Genus | Anisomeles |
| Species | Malabarica |
| Botanical name | Anisomeles malabarica |
Table 1: A. malabarica’s taxonomic classification is given [37].
Since A. malabarica is a medicinal plant, has been used as a folkloric medicine to treat amentia, anorexia, fevers, swellings, rheumatism. The plant A. malabarica is used traditionally in the treatment of intermittent fever, colic dyspepsia and curing wounds [38].
Earlier phytochemical studies of A. malabarica have shown the presence of many chemical constituents as shown in Table 2.
| Plant | Phytochemicals |
|---|---|
| Anisomeles malabarica | Anisomelic acid |
| Anisomelolide | |
| 2-acetoxymalabaric acid | |
| Anisomelyl acetate anisomelin | |
| Betulinic acid | |
| ß-sitosterol, | |
| Gerainic acid | |
| Malabaric acid | |
| Ovatodiolide | |
| Triterpenebetulinic acid | |
| Citral |
Table 2: Shows phytochemical A. malabarica [39,40].
In certain circumstances, medicinal plants’ crude extracts may be utilised as medicines. Medicinal plants may supply physiologically active compounds as well as lead structures for the creation of improved derivatives. Some natural sources botanical substances have a wide variety of chemical active components that may interfere with all of the mosquito’s biological activities, interrupting its life span and dispersion and reducing danger to people and animals. As crude material, particular active components, essential oils, several therapeutic plants were evaluated for its pesticide and repellent capabilities [41]. This study gives an overview of the many kinds of molecules found in plants, and provides examples of the different types of molecules and secondary metabolites that have contributed to the creation of these pharmacologically active extracts. As a result, some information on the importance of A. malabarica against malarial vectors and the therapeutic properties were briefly proven which are anti-anaphylactic, anti-pyretic action, anti- bacterial, anti-allergic, anticancer, anti-pyretic action, anti- carcinogenic, anti-inflammatory, anti-allergic, antiepileptic, antifertility, antispasmodic, and other medicinal properties [42].
Anti-Allergic
As the world’s population grows, so does the prevalence of allergic disorders, and increasing morbidity is a key problem. Several natural compounds have been discovered to have anti-allergic properties. Furthermore, plant preparations have been shown to be beneficial in clinical studies and to have extra benefits when combined with Western drugs, including synergism and immune system regulation [43]. Anti-allergic effects have been discovered in the essential oil of A. malabarica.
Anti-Anaphylactic
Hypersensitivity is a life-threatening allergic response that occurs suddenly. Anaphylaxis is a life-threatening systemic allergic response that happens abruptly after coming into contact with an allergen. Anaphylaxis affects 0.05-2 percent of individuals worldwide however at time in their lives, and the incidence of occurrence seems to be rising [44]. Currently, there is a greater emphasis on plant study across the globe, and there is a growing body of data demonstrating the enormous therapeutic potential employed in diverse traditional systems. Essential chemical components in A. malabarica operate as an anti-anaphylactic agent [45].
Antibacterial
Pathogenic bacteria have developed several defensive mechanisms against antimicrobial treatments, resulting in an increase in drug resistance to both old and new medications. The emergence of antibiotic resistance in pathogenic microbes has necessitated the testing of a number of medicinal plants for possible antimicrobial properties. Chemical constituents from A. malabarica leaves exhibit antibacterial activity over Gram-negative and Gram- positive infectious bacteria such as, Klebsiella pneumoniae, E. coli Staphylococcus aureus, pseudomonas aeruginosa, Vibrio cholerae, and Proteus mirabilis [45, 46, 47].
Antiepileptic Potential
Antiepileptics (also termed as anticonvulsants medications) are a class of pharmaceuticals that are used to treat epileptic seizures. Anticonvulsants are also being used more often to treat bipolar illness. Traditional medicinal herbs used to treat epilepsy have been demonstrated to exhibit potential anticonvulsant effects in experimental animals of anticonvulsant screening, making them a viable source for finding novel antiepileptic chemicals. In folk medicine, A. malabarica possesses a variety of medicinal properties. The ethylacetate extract of the leaves of A. malabarica has been reported to have antiepileptic properties [39].
Anti-Cancer
Cancer is among the world’s most serious health concerns, afflicting both poor and rich nations. Alternative medicine uses medicinal plants and their extracted lead compounds to treat neoplastic cells, which are abnormally proliferating cells in the body that cause cancer. Anticancer drugs have been isolated from a variety of effective chemicals obtained from natural materials. These chemicals are designed to be used in the development of cancer-fighting medications. A. malabarica has a multitude of pharmacological actions, according to Chopra, et al. [48]. Jeyachandran, et al. reemphasized the anticancer properties of A. malabarica in traditional medicine [40].
Antispasmodic: Antispasmodic is a medication used to treat uncontrolled muscular movements, especially in the bowels and stomach. The medicine phenobarbital, which belongs to the barbiturate family of drugs. A. malabarica has important chemical components that act as antispasmodics [40].
Anti-Carcinogenic
Toxins are engaged in mutagenesis, carcinogenesis, and genotoxicity. The usage of medicinal herbs, or natural anticarcinogens, is one of the most effective strategies to reduce the harmful effects of carcinogens. Flavonoids, coumarone, phenolic, anthraquinones, tannins, carotenoids, saponins, and other compounds fall under this category. These natural compounds are beneficial not only in the initial chemoprevention, but also in the prevention of developing cancer, which is the most crucial factor to determine survivability [48]. Anti-carcinogenic agents were discovered in abundance of A. malabarica [45].
Anti-Inflammatory
The quality of a medication or therapy that lowers inflammation is known as anti-inflammatory. Anti- inflammatory medicines, as opposed to opioids, which impact the central nervous system, account for nearly half of analgesics. They relieve the pain by lowering inflammation. The occurrence of chemicals such as tri-terpenoids, flavones, flavonones, and phenols in A. malabarica may explain its anti-inflammatory effect [49].
Antifertility
Refers to the inability to conceive or get pregnant. Many plants have been used to lower fertility in the past, and current scientific study has verified that at least some of the herbs studied have anti-fertility effects. A. malabarica’s antifertility capability was proven by Setty, et al. [50].
Antipyretic Activity
Refers to the ability of medications or plants to lower fever. Antipyretics allow the hypothalamus to counteract a rise in temperature caused by interleukin. The body then strives to bring the temperature down, lowering the fever. Plants utilised as antipyretic agents include Adansonia digitata, Berberis species, Capparis zeylanica, Cleome viscose, Vernonia cinerea including A. malabarica [51, 52].
Epilepsy, Fever, and fever caused by teething in children are all treated with an extract of the leaves in traditional medicine. Rheumatoid arthritis is treated by an external application of a leaf extract and essential oil [53, 54, 55]. Alcohol and aqueous extracts of the leaf have been proven to have significant spermicidal activity in prior studies [56]. The plant also contains antisomelic acid, ovatodiolide, anisomelyl acetate (diterpene), and betulinic acid (triterpene) [57]. Morphologic and anatomic features, physiochemical constants, and phytochemical screening of A. malabarica leaves, as well as the macroscopical properties of A. malabarica, as indicated in Table 3.
In the anatomical characteristics, the lower epidermal part of the leaves is covered by a thick layer of cuticle. The epithelia are all polygonal, which means they seem to be the same size and shape. Paracytic stomata is shown on both surfaces. A layer of extended palisade cells makes up the leaf mesophyll. There are 2 type of collenchymatous cells in the layers of the epidermis of the midrip portion of the leaf. The vessels of the vascular bundles are annular and swirly thickened. The various isolates were found to a preliminary phytochemical screening. Other phytocomponents such as alkaloid, tannin, sugar, saponin, protein, steriod, and others are found [59].
| Character | Observation |
|---|---|
| Colour | Pale green (Upper surface), greenish (Under surface) |
| Odour | Aromatic and enjoyable |
| Size | 5–7 cm in length, 3–4.5 cm in width |
| Surface | Wody and soft |
| Shape | Lanceolate – Oblong |
| Type | Simple |
| Arrangement | Opposite |
| Petiole | 1–1.5 mm in length |
| Margin | Serrate – Crenate |
| Apex | Acute |
| Venation | Pinnate |
| Midrib | Projected lower surface, depressed upper surface |
Table 3: Macroscopic characteristics of _Anisomeles_ _malabarica_ [58].
The leaves of A. malabarica are used to treat intermittent fever, dyspepsia, boils, colic, and tetanus. In Indian traditional medicine, the leaf extract is used for cough, stomach ache, epilepsy, cold, fever, and fever induced by teething in children, and the infusion of the leaf and essential oil is used locally to treat rheumatoid arthritis. A. malabarica has been demonstrated to have high therapeutic potential, including anti-inflammatory, antiepileptic, cold, fever, cytotoxic impact on cancer cells, anti-cancer activities [60] and the focused anti-hyperglycemic and anti-hyperlipidemic activities have been shown in the past [61, 62].
A. Malabarica Anti-diabetic Effects are Mediated by Biochemical Processes
Kotha et al., 2019 tested the anti hyperglycemic activity of different solvent extracts of A. malabarica in STZ-induced diabetic rats and isolated the active fraction of AM (AMAF) from the ethyl acetate extract, which had the best antihyperglycemic activity. AMAF showed a high anti-hyperglycemic impact and improved glucose control in diabetic rats due to the presence of unsaturated fatty acids and phenolic compounds that were extracted and characterised from AMAF [62]. AMAF increased insulin levels while reducing HbA1c in diabetic rats. The effects of the A. malabarica active fraction (AMAF) on key regulatory carbohydrate metabolic enzymes such as hexokinase, glucose- 6-phosphatase, glucose-6-phosphate dehydrogenase, and fructose 1,6-bisphosphatase, as well as oxidative stress and antioxidant enzymes such as catalase, superoxide dismutase, and glutathione-s-transferase were investigated in this A. malabarica was collected and processed as previously described CP Preethy, et al. [61, 62]. In a nutshell, ethyl acetate extract was prepared by soaking A. malabarica leaf powder in a glass jar for 48 hours at room temperature, then filtering the solvent. STZ was generated in ice cold citrate buffer by diabetic mellitus induction in albino males to cause diabetes in overnight fasting mice [61, 62]. The active part and glibenclamide (also referred as glyburide, a sulfonylurea group of drugs) were administered orally to the respective groups each morning over 30 days through stomach intubation. Water was provided to normal and diabetic control rats. On days 8, 15, 22, and 31, all experimental rats had their body weights assessed. On day 31, all five groups of rats were slain by anaesthetizing them with anaesthetic ether and cervical dislocation after an overnight fast. Blood and tissues were collected and stored at -80°C until required.
Discussion
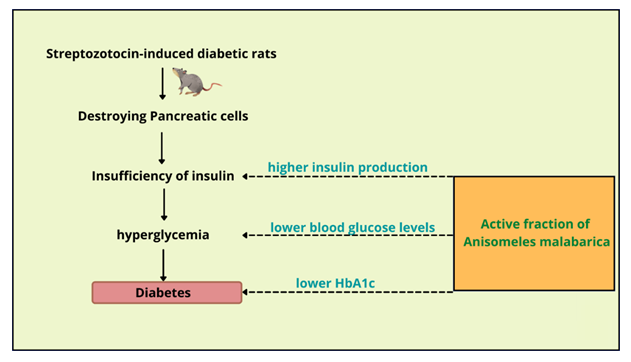
To evaluate the beneficial effects of the active components of A. malabarica leaves on experimentally developed diabetes mellitus rats, Kotha, et al. Utilised streptozotocin-induced diabetic rats [62, 63]. Normal rats were given a single dose of STZ intraperitoneally, which produced hyperglycaemia by selectively killing the pancreatic-cell population, resulting in insulin deficiency and leads to diabetes mellitus. Consistent hyperglycaemia and insufficient glycaemic control, which are distinguishing features of diabetes mellitus, lead to diabetes-related micro- and macrovascular complications, which may be delayed or averted by maintaining rigorous glycaemic control [16, 17]. Figure 1 show that AMAF treatment resulted in significantly lower fasting blood glucose levels, increased insulin production, and a reduced HbA1c in STZ-induced diabetic rats.
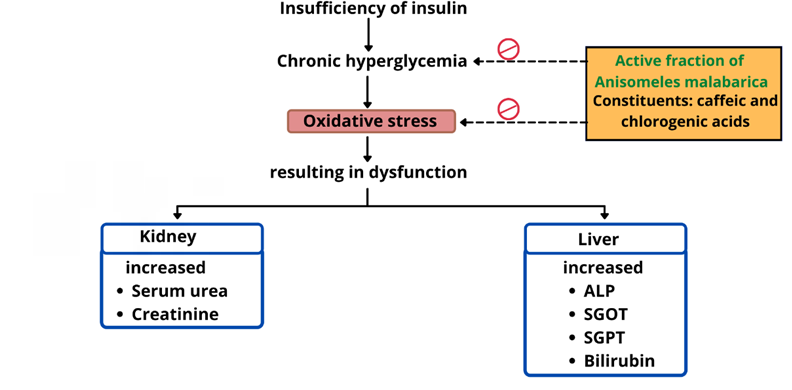
Raised SGOT, SGPT, ALP, and bilirubin are one of the pathophysiological abnormalities in liver function markers in artificially induced diabetic rats [64]. In the diabetic AMAF therapy group, the active fraction lowered these elevated liver function markers to near-normal levels. Diabetic rats had increased serum urea and creatinine levels, suggesting renal failure [65].
Significant decreases in blood urea and creatinine were detected in diabetic rats given the active component, probably owing to AMAF’s direct or indirect glycemic control activities. Chronic hyperglycemia leads to oxidative stress in a number of organs, such as the liver and kidney, leading to malfunction, as seen by elevated hepatic and renal functional markers. Figure 2 shows that AMAF therapy improved glycemic control and lowered oxidative stress.
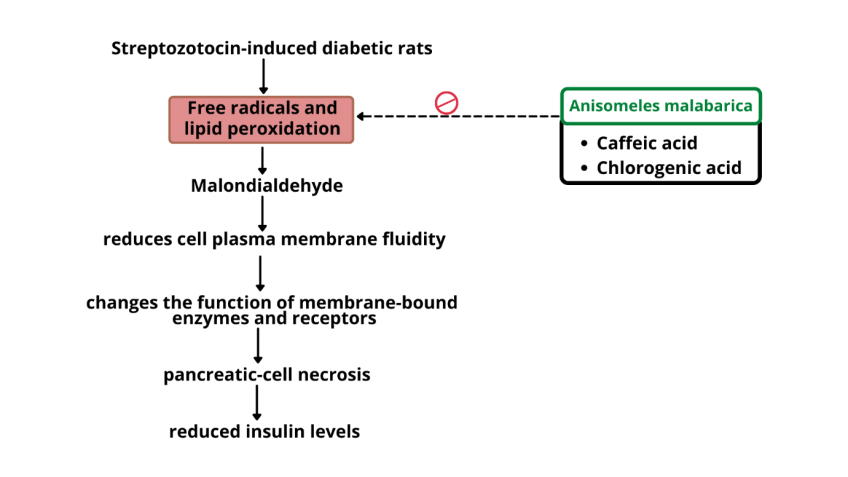
In AMAF, for the first time caffeic acid, luteolin, quinic acid, kaempferol, and chlorogenic acid were identified [62]. Caffeic and chlorogenic acids were discovered to have anti-hyperglycaemic and antioxidant effects in diabetic rats [66, 67]. Phenolic substances such as kaempferol and luteolin have been found as antioxidants [68, 69]. Studies have connected free radical generation, lipid peroxidation, and glycaemic regulation to the development of diabetes mellitus [10, 11, 12]. Malondialdehyde (MDA), a by-product of lipid peroxidation, was discovered in larger levels in diabetic rats as compared to normal rats. MDA levels are proportional to lipid peroxidation, which lowers the fluidity of the cell plasma membrane and alters the function of membrane- bound enzymes and receptors. Vinod, et al. Demonstrated the antioxidant activity of A. malabarica in vitro, but no in vivo studies with plausible mechanisms of action have been established [70]. After treatment with AMAF, MDA levels in both tissues of diabetic rats were reduced, suggesting that free radical generation and lipid peroxidation were avoided. This suggests that A. malabarica active component may have a protective effect against oxidative stress and associated illnesses. A number of phytoconstituents have been demonstrated to have strong antioxidant activities in diabetic rats [71]. As illustrated in figure 3, AMAF activity on chronic hyperglycaemia induces oxidative stress [10, 11, 12].
The actions of antioxidant enzymes such as GPx, SOD, and GST were significantly decreased in diabetic group of rats, although CAT activity increased. These alterations might be caused due to pancreatic-cell necrosis and concomitant lower insulin levels [62], resulting in prolonged hyperglycemia and an imbalanced hepatic antioxidant state and lipid peroxidation, as demonstrated in the study. After receiving AMAF, diabetic rats’ antioxidant enzyme activity was restored. This might be due to the antioxidant potential of the AMAF, which aids in the repair of the antioxidant protecting system by detoxifying and avoiding lipid peroxidation. This finding is supported by A. malabarica’s antioxidant activity in in-vitro [70]. This antioxidant impact might be attributed to improved glycemic control and insulin levels, as well as the consequences of active ingredients such quinic acid, lutetolin, kaempferol, caffeic acid, and chlorogenic acid. The necrosis of the islets of Langerhans was discovered in pancreatic tissue, which could be the underlying cause of the reduced insulin levels seen in diabetic animals [62]. Similar histology in the pancreas of STZ-diabetic rats has been observed by others [72]. AMAF treatment repaired the abnormal architecture of pancreatic tissue in diabetic rats, according to the study. This might be because AMAF contains phytochemicals that help the pancreas regenerate. As a consequence of decreased glycogen levels and fat droplet production, chronic hyperglycemia and hyperlipidemia cause degenerative changes in the histology of the liver, including abnormal location and infiltration of hepatocytic nuclei [73]. AMAF-treated diabetic rats revealed regenerative changes in hepatic tissue, which might be connected to decreased tissue lipid profiles and better antioxidant mechanisms, according to our results. The kidneys of STZ-induced diabetic rats showed renal lesions, cell debris disseminated in tubular lumina, increased tubular epithelial cell thickness, extensive cellular infiltration, areas of bleeding in interstitial tissue, and degeneration with larger Bowman’s capsule. In diabetic rats, however, treatment with AMAF restored these changes, demonstrating that it possesses renoprotective characteristics in hyperlipidemia and hyperglycemia [62, 63]. A partial or complete absence of insulin impairs glucose homeostasis in both humans and rodents, reducing hexokinase levels, glucokinase enzyme activity, and GLUT-2 expression [74]. Insulin also supports the synthesis of hepatic glycogen by mobilising glucose and generating glycogenesis and glycolysis substrate. G6Pase and FBPase, two key gluconeogenesis enzymes, are also inhibited, which prevents hepatic glucose production. These data show that restoring hexokinase and glucose kinase activity improves diabetes management by restoring normal glucose levels [75, 76]. As evidenced by semi-quantitative PCR data and enzyme activities, oral administration of the active fraction of A. malabarica increased hexokinase activity in hepatic and renal tissues, as well as upregulated hepatic glucokinase expression, by stimulating the pancreas’ remnant or regenerated cells to secrete more insulin, promoting glycolysis and glycogenesis while inhibiting gluconeogenesis. Medicinal plant preparations have been shown to have beneficial effects on glucose metabolism enzyme activity in the past [77, 78, 79], which is compatible with our results. PEPCK, G6Pase, and FBPase all play a role in the gluconeogenic pathway. The expression and/or activity of PePCK, G6Pase, and FBPase have been found to be indicators of hepatic glucose production [79, 80].
An ethanolic extract of Artemisia dracunculus inhibited PEPCK expression in STZ-induced diabetic rats, decreasing hepatic glucose production [81]. In diabetic rats, AMAF decreased PEPCK expression, likely reducing hepatic glucose production. Insulin suppresses the activities of G6Pase and FBPase under normal conditions. The insulinogenic activity of AMAF [62], which was complimented by the T-cell regeneration function of AMAF reported in our work, and/or the insulin-sensitizing effect of AMAF [62], might explain why these two enzymes were suppressed when diabetic rats were given AMAF. Glucose-6-phosphate dehydrogenase catalyses the rate-limiting step of the hexose monophosphate shunt. G6PD activity in hepatic and renal tissues was much lower in STZ-induced diabetic rats than in normal rats. Insulin increases glucose 6-phosphate dehydrogenase activity in a dose-dependent manner [82, 83, 84, 85, 86, 87, 88, 89]. AMAF significantly increased glucose 6-phosphate dehydrogenase activity in our mice, likely through boosting insulin production, according to our findings.
Besides that, previous research has shown that people with diabetes lose weight and have lower protein and glycogen substance level in their tissues as a result of insulin deficiency as well as resistance, resulting in excessive breakdown or loss of structural tissue proteins and fat degradation as a result of glucose homeostasis disturbances [83, 84]. STZ-induced diabetic rats exhibited considerably lower body weights, protein, and glycogen content in their tissues than normal control rats, according to this study. AMAF-treated rats, on the other hand, were significantly protected against body weight loss, protein and glycogen breakdown in tissues, indicating that AMAF may have anti- diabetic characteristics. Prior study [85, 86, 87, 88, 89, 90] indicated that diabetic rats’ hepatic and renal organs had increased body weights, protein, and glycogen levels following treatment with medicinal plants or their derivatives. We deduce that the active fraction of A. malabarica leaves (AMAF) has a significant glucose lowering and glycemic control effect based on our previous and current results. It’s also possible that the active portion activates and/or regenerates pancreatic cells, leading the pancreas to produce more insulin. Quinic acid, chlorogenic acid, caffeic acid, luteolin, and kaempferol are some of the phytochemicals involved in AMAF’s anti-diabetic properties [91, 92, 93, 94, 95, 96, 97, 98].
The oral administration of the active fraction of A. malabarica (AMAF) reduced the pathological changes associated with STZ-induced diabetes mellitus in experimental rats, according to Kotha et al. The AMAF has beneficial effects on body weights, glycogen, protein, GLUT- 2, hepatic and renal functional indicators, lipid peroxidation, carbohydrate metabolic enzyme activities, and antioxidant enzyme activities, according to the results of the study. AMAF may have anti-diabetic characteristics in regulating glucose homeostasis and protecting hepatic and renal tissues from oxidative damage, perhaps delaying the development of diabetes mellitus’ secondary complications.
Conclusion
Oral treatment of the active fraction of A. malabarica (AMAF) in experimental rats decreased the pathological alterations associated with STZ-induced diabetes mellitus. According to the findings of the research, the AMAF has favourable effects on body weights, glycogen, protein, GLUT- 2, hepatic and renal functional indicators, lipid peroxidation, carbohydrate metabolic enzyme activities, and antioxidant enzyme activities. AMAF may have anti-diabetic properties in that it regulates glucose homeostasis and protects hepatic and renal tissues from oxidative damage, perhaps delaying the onset of diabetes’ secondary consequences. The antioxidant potential of the AMAF, which aids in the repair of the antioxidant protecting system by detoxifying and avoiding lipid peroxidation. This antioxidant impact might be attributed to improved glycemic control and insulin levels, as well as the consequences of active ingredients such quinic acid, lutetolin, kaempferol, caffeic acid, and chlorogenic acid. The necrosis of the islets of Langerhans was discovered in pancreatic tissue, which could be the underlying cause of the reduced insulin levels seen in diabetic animals. This article, concludes that the AM could be a used as medicinal plant to treat diabetes for its safe and effective anti-diabetic potential.
References
-
IDF (2017) Diabetes Atlas. 8th (Edn.), International Diabetes Federation.
-
Ferre T, Riu E, Bosch F, Valera A (1996) Valera Evidence from transgenic mice that glucokinase is rate limiting for glucose utilization in the liver. Federation of American Societies for Experimental Biology 10(10): 1213-1218.
-
WHO (2018) Diabetes. World Health Organization.
-
Nawale RB, VK Mourya, SB Bhise (2006) Non enzymatic glycation of proteins a cause for complications in diabetes. Indian Journal of Biochemistry Biophysics 43(6): 337-344.
-
Ramachandran A (2014) Know the signs and symptoms of diabetes. The Indian Journal of Medical Research 140(5): 579-58.
-
Hirsch IB (1999) Type 1 diabetes mellitus and the use of flexible insulin regimens. American Family Physician 60(8): 2343-2356.
-
American Diabetes Association (2011) Standards of Medical Care in Diabetes. Diabetes Care 34(1): 11-61.
-
Kirkman MS, Briscoe VJ, Clark N (2012) Diabetes in older adults. Diabetes Care 35(12): 2650-2664.
-
McAnuff MA, Omoruyi FO, Morrison EYSA, Asemota HN (2005) Changes in some liver enzymes in streptozotocin induced diabetic rats fed sapogenin extract from bitter yam Dioscorea polygonoides or commercial diosgenin. West Indian Medical Journal 54(2): 97-101.
-
Kesavulu MM, Giri R, Kameswara RB, Apparao C (2000) Lipid peroxidation and antioxidant enzyme levels in type 2 diabetics with microvascular complications. Diabetes Metab 26(5): 387-392.
-
Kesavulu MM, Rao BK, Giri R, Vijaya J, Subramanyam G, et al. (2001) Lipid peroxidation and antioxidant enzyme status in Type 2 diabetics with coronary heart disease. Diabetes Research and Clinical Practice 53(1): 33-39.
-
Sheweita SA, Mashaly S, Newairy AA, Abdou HM, Eweda SM (2016) Changes in oxidative stress and antioxidant enzyme activities in streptozotocin induced diabetes mellitus in rats role of Alhagi maurorum extracts. Oxidative Medicine and Cellular Longevity, pp: 1-8.
-
American Diabetes Association (2008) Standards of Medical Care in Diabetes. Diabetes care 31(1): 12-54.
-
Rajasekhar MD, Sreelatha A, Apparao C (2006) Treatment of diabetes mellitus plant drugs vs oral hypoglycemic agents and insulin. Recent Progress in Medicinal Plants 14: 279-296.
-
Chang CLT, Lin Y, Bartolome AP, Chen YC, Chiu SC, et al. (2013) Herbal therapies for type 2 diabetes mellitus chemistry biology and potential application of selected plants and compounds. Evidence Based Complementary and Alternative Medicine 2013: 378-657.
-
Nicasio P, Aguilar Santamaría L, Aranda E, Ortiz S, et al. (2005) Hypoglycemic effect and chlorogenic acid content in two Cecropia species. Phytotherapy Research 19(8): 661-664.
-
Rajasekhar MD, Badri KR, Kumar KV, Kassetti RB, Fatima SS, et al. (2010) Isolation and characterization of a novel anti hyperglycemic protein from the fruits of Momordica cymbalaria. Journal of Ethnopharmacol 128(1): 58-62.
-
Marella S, Maddirela DR, Badri KR, Jyothi Kumar MV, Chippada A (2015) Anti hyperlipidemic and biochemical activities of mcy protein in streptozotocin induced diabetic rats. Cellular Physiology and Biochemistry 35(4): 1326-1334.
-
Gurib-Fakim A (2006) Medicinal plant traditions of yesterday and drugs of tomorrow. Molecular Aspects of Medicine 27(1): 1-93.
-
Bever BO, Zahnd GR (1979) Plants with Oral Hypoglycaemic action. Quarterly Journal of Crude Drug Research 17(4): 139-196.
-
Rahman AU, Zaman K (1989) Medicinal plants with hypoglycemic activity. Journal of Ethnopharmacology 26(1): 1-55.
-
Marles RJ, Farnsworth NR (1995) Antidiabetic plants and their active constituents. Phytomedicine 2(2): 137- 189.
-
Li WL, Zheng HC, Bukuru J, De Kimpe N (2004) Natural medicines used in the traditional Chinese medical system for therapy of diabetes mellitus. Journal of Ethnopharmacology 92(1): 1-21.
-
Simmonds MSJ, Howes MJR (2006) Plants used in the treatment of diabetes. In: Soumyanath A (Ed.), Traditional medicines for modern times Antidiabetic plants, CRC Press.
-
Giovannini P, Howes MJ, Edwards SE (2016) Medicinal plants used in the traditional management of diabetes and its sequelae in Central America A review. Journal of Ethnopharmacology 184: 58-71.
-
Harlev E, Nevo E, Mirsky N, Ofir R (2013) Antidiabetic attributes of desert and steppic plants A review. Planta Medica 79(6): 425-436.
-
Moradi B, Abbaszadeh S, Shahsavari S, Alizadeh M, Beyranvand F (2018) The most useful medicinal herbs to treat diabetes. Biomedical Research and Therapy 5(8): 2538-2551.
-
Eddouks M, Maghrani M, Lemhadri A, Ouahidi ML, Jouad H (2002) Ethnopharmacological survey of medicinal plants used for the treatment of diabetes mellitus hypertension and cardiac diseases in the south east region of Morocco Tafilalet. Journal of Ethnopharmacology 82(2-3): 97- 103.
-
Tag H, Kalita P, Dwivedi P, Das AK, Namsa ND (2012) Herbal medicines used in the treatment of diabetes mellitus in Arunachal Himalaya northeast India. Journal of Ethnopharmacology 141(3): 786-795.
-
Rios JL, Francini F, Schinella GR (2015) Natural products for the treatment of type 2 diabetes mellitus. Planta Medica 81(12-13): 975-994.
-
McCurdy CR, Scully SS (2005) Analgesic substances derived from natural products (natureceuticals). Life Sci 78(5): 476-484.
-
Sneader W (2005) Drug Discovery: a History. Chichester, Wiley, UK, pp: 1-468.
-
Samuelsson G (2004) Drugs of natural origin: a textbook of pharmacognosy. In: Samuelson G (Ed.), Journal of Natural Products. 5th(Edn.), Swedish Pharmaceutical Press, Stockholm, pp: 620.
-
Gurib-Fakim A (2006) Medicinal plants: Tradition of yesterday and drugs of tomorrow Review article. Mol Aspects Med 27(1): 1-93.
-
Naghibi F, Mosaddegh M, Motamed SM, Ghorbani A (2005) Labiatae family in folk medicine in Iran:From ethnobotany to pharmacology. Iranian Journal of Pharmaceutical Research 4(2): 63-79.
-
Joshi SG (2000) Medicinal Plants. Mohan Primlone for Oxfordand IBH Publishing Co Pvt Ltd, India, pp: 222.
-
Singh RS, Uvarani M, Raman SR (2003) Pharmacognostical and phytochemicalstudies on leaves of Anisomeles malabarica. Ancient Sci Life 22(3): 106-110.
-
Jeyachandran R, Mahesh A, Cindrella L (2007) DEN- Induced cancer and its alleviation by Anisomeles malabarica (L.) R.Br. ethanolic leaf extract in male albinomice. International journal of cancer research 3(4): 174-179.
-
Bakshi GDN, Sensarma P, Pal DC (1999) A Lexicon of Medicinal Plants in India, Naya Prakash, Calcutta, India, pp: 152.
-
Choudhary N, Bijjem KR, Kalia AN (2011) Antiepileptic potential of flavonoids fraction from the leaves of Anisomeles malabarica. Journal of Ethnopharmacology 135(2): 238-242.
-
Rameshprabu R (2005) Studies on the larvicidal, pupicidal and repellent properties of Anisomeles malabarica (L) for the control of malaria vector Anopheles stephensi Listen. Bharathiar University, Coimbatore,Tamil Nadu, India.
-
Ramaraj R, Unpaprom Y (2013) Medicinally Potential Plant of Anisomeles malabarica (L.)R. Br. Journal of Agricultural Extension and Rural Development 30(3): 29-39.
-
Cota BB, Bertollo CM, Oliveira DM (2013) Anti-allergic potential of herbs andherbal natural products-activities and patents. Recent Pat Endocr Metab Immune Drug Discov 7(1): 26-56.
-
Tintinalli JE, John O, Donald MY, Meckler GD, Stapczynski JS, et al. (2010) Emergency Medicine: A Comprehensive Study Guide. In: Tintinalli JE, et al. (Eds.), Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 9e. 9th (Edn.), McGraw-Hill Companies, New York, USA, pp: 890.
-
Kavitha T, Nelson R, Thenmozhi R, Priya E (2012) Antimicrobial activity andphytochemical analysis of Anisomeles malabarica (L). Journal of Microbiology and Biotechnology 2(1): 1-5.
-
Remya M, Pankaj J, Someshwar N (2012) Bioactivity studies on Anisomeles malabarica (AM) R.Br. Journal of Biotechnology and Biotherapeutics 2(9): 1-8.
-
Chopra RN, Nayar SL, Chopra IC, Asolkar LV, Kakkar KK, et al. (1956) Glossary of Indian Medicinal Plants. Council of Scientific and Industrial Research, New Delhi, India, pp: 487.
-
Bhattacharya S (2012) Anticarcinogenic property of medicinal plants: involvement of antioxidant role Medicinal Plants as Antioxidant Agents: Understanding their Mechanism of Action and Therapeutic Efficacy, Research Sign post, Trivandrum, India, pp: 83-96.
-
Lavanya R, Maheshwari SU, Harish G, Bharath RJ, Kamali S, et al. (2011) Investigation of In-vitro anti- Inflammatory, anti-platelet and anti-arthritic activities in the leaves of Anisomeles malabarica Linn. Research Journal of Pharmaceutical Biological and Chemical Sciences 1(4): 745-752.
-
Setty BS, Kamboj VP, Garg HS, Khanna NM (1976) Spermicidal potential of saponins isolated from Indian medicinal plants. Contraception 14(5): 571-578.
-
Shah BN, Seth AK (2010) Medicinal Plants as a Source of Antipyretic Agents A Review. Archives of applied science research 2(3): 188-195.
-
Srinivasan P, Sudha A, Bharathajothi P, Rajaguru K, Rameshthangam P, et al. (2010) Effects of anti- inflammatory and antipyreticactivity of Anisomeles malabarica R.Br. Journal of Pharmacy Research 3(7): 1598-1601.
-
Sheikh BA, Pari L, Rathinam A, Chandramohan R (2015) Trans-anethole, a terpenoid ameliorates hyperglycemia by regulating key enzymes of carbohydrate metabolism in streptozotocin induced diabetic rats. Biochimie 112: 57-65.
-
Gupta AK, Tandon N (2004) Reviews on Indian Medicinal Plants. Indian Council of Medical Res, New Delhi, India.
-
Pushpangadan P, Atal CK (1984) Ethno-medico-botanical investigations in Kerala I. Some primitive tribals of Western Ghats and their herbal medicine. Journal of Ethnopharmacol 11(1): 59-77.
-
Sudha A, Srinivasan P (2014) Bioassay-guided isolation, identification and molecular ligand-target insight of lipoxygenase inhibitors from leaves of Anisomeles malabarica R.Br. Pharmacognosy magazine 10(3): S596-S605.
-
Choudhary N, Bijjem KRV, Kalia AN (2011) Antiepileptic potential of flavonoids fraction from the leaves of Anisomeles malabarica. Journal of Ethnopharmacol 135(2): 238-242.
-
Mathew KM (1983) Illustrations on the flora of Tamil Nadu Carnatic 4: 482.
-
Britto SJ, Matthew KM (1993) Maiya Thamizhaga KalaVagai Thavaraviyal 574-575.
-
Preethy CP, Alshatwi AA, Gunasekaran M, Akbarsha MA (2013) Analysis of the cytotoxic potential of anisomelic acid isolated from anisomeles malabarica. Scientia Pharmaceutica 81(2): 559-566.
-
Preethy CP, Padmapriya R, Periasamy VS, Riyasdeen A, Srinag S, et al. (2012) Antiproliferative property of nhexane and chloroform extracts of Anisomeles malabarica (L). R. Br. in HPV16- positive human cervical cancer cells. Journal of Pharmacology and Pharmacotherapeutics 3(1): 26-34.
-
Kotha P, Badri KR, Nagalapuram R, Allagadda R, Chippada AR (2017) Anti-diabetic potential of the leaves of _Anisomeles malabarica_ in streptozotocin induced diabetic rats. Cellular Physiology and Biochemistry 43(4): 1689-1702.
-
Kotha P, Badri KR, Chippada AR (2017) Protective effect of _A. malabarica_ leaves against hyperlipidemia and oxidative stress in streptozotocin induced diabetic rats. Medicinal plants and herbal supplements 256-260.
-
Nabi SA, Kasetti RB, Sirasanagandla S, Tilak TK, Kumar MVJ, et al. (2013) Antidiabetic and antihyperlipidemic activity of Piper longum root aqueous extract in STZ induced diabetic rats. BMC complementary and alternative medicine 13: 37.
-
Ramachandran S, Rajasekaran A, Manisenthilkumar KT (2012) Investigation of hypoglycemic, hypolipidemic and antioxidant activities of aqueous extract of Terminalia paniculata bark in diabetic rats. Asian pacific journal of tropical biomedicine 2(4): 262-268.
-
Jung UJ, Lee MK, Park YB, Jeon MS, Choi MS (2006) Antihyperglycemic and Antioxidant Properties of Caffeic Acid in db/db mice. J Pharmacol Exp Ther 318(2): 476- 483.
-
Meng S, Cao J, Feng Q, Peng J, Hu Y (2013) Roles of chlorogenic acid on regulating glucose and lipids metabolism: a review. Evid Based Complement Alternat Med 2013: 801457.
-
L Chen, G Tian, W Tang, W Luo, P Liu (2016) Protective Effect of Luteolin on Streptozotocin-Induced Diabetic Renal Damage in Mice via the Regulation of RIP140 / NF- K B Pathway and insulin signalling pathway. Journal of Functional Foods 22: 93-100.
-
Numair KSA, Chandramohan G, Veeramani C, Alsaif MA (2015) Ameliorative effect of kaempferol, a flavonoid, on oxidative stress in streptozotocin-induced diabetic rats. Redox Report 20(5): 198-209.
-
Vinod G, Ramesh BS, Suvarna MNV, Hanumanthappa KM (2014) In-vitro antioxidant potential of solvent extracts from _Anisomeles malabarica_. Journal of pharmacognosy and phytochemistry 3(3): 99-103.
-
Coman C, Rugina OD, Socaciu C (2012) Plants and natural compounds with antidiabetic action. Notulae Botanicae Horti Agrobotanici Cluj-Napoca 40(1): 314-325.
-
Girija K, Lakshman K, Udaya C, Sachi GS, Divya T (2011) Anti-diabetic and anticholesterolemic activity of methanol extracts of three species of Amaranthus. Asian Pac J Trop Biomed 1(2): 133-138.
-
Prabhakar PK, Prasad R Ali, S, Doble M (2013) Synergistic interaction of ferulic acid with commercial hypoglycemic drugs in streptozotocin induced diabetic rats. Phytomedicine 20(6): 488-494.
-
Prasath GS, Subramanian SP (2011) Modulatory effects of fisetin, a bioflavonoid, on hyperglycemia by attenuating the key enzymes of carbohydrate metabolism in hepatic and renal tissues in streptozotocin-induced diabetic rats. Eur J Pharmacol 668(3): 492-496.
-
Postic C, Burcelin R, Rencurel F, Pegorier JP, Loizeau M, et al. (1993) Evidence for a transient inhibitory effect of insulin on GLUT2 expression in the liver: studies in vivo and _in vitro_. Biochemical Journal 293(Pt 1): 119-124.
-
Matschinsky FM, Magnuson MA, Zelent D, Jetton TL, Doliba N, et al. (2006) The network of glucokinase- expressing cells in glucose homeostasis and the potential of glucokinase activators for diabetes therapy. Diabetes 55(1): 1-12.
-
Kasetti RB, Nabi SA, Swapna S, Apparao C (2012) Cinnamic acid as one of the antidiabetic active principle(s) from the seeds of Syzygium alternifolium. Food and Chemical Toxicology 50(5): 1425-1431.
-
Kondeti VK, Badri KR, Maddirala DR, Thur SKM, Fatima SS, et al. (2010) Effect of Pterocarpus santalinus bark, on blood glucose, serum lipids, plasma insulin and hepatic carbohydrate metabolic enzymes in streptozotocin- induced diabetic rats. Food and Chemical Toxicology 48(5): 1281-1287.
-
Hanson RW, Reshef L (1997) Regulation of phosphoenolpyruvate carboxykinase (GTP) gene expression. Annu Rev Biochem 66: 581-611.
-
Nordlie RC, Foster JD, Lange AJ (1999) Regulation of glucose production by the liver. Annu Rev Nutr 19: 379- 406.
-
Ribnicky DM, Poulev A, Watford M, Cefalu WT, Raskin I (2006) Antihyperglycemic activity of TarralinTM, an ethanolic extract of _Artemisia dracunculus_ L. Phytomedicine 13(8): 550-557.
-
Weber G, Convery HJH (1966) Insulin: inducer of glucose 6-phosphate dehydrogenase. Life Sciences 5(12): 1139- 1146.
-
Dice JF, Walker CD, Byrne B, Cardiel A (1978) General characteristics of protein degradation in diabetes and starvation. Proc Natl Acad Sci USA 75(5): 2093-2097.
-
Musabayane CT, Mahlalela N, Shode FO, Ojewole JAO (2005) Effects of _Syzygium cordatum_ leaf extract on plasma glucose and hepatic glycogen in streptozotocin- induced diabetic rats. Journal of Ethnopharmacol 97(3): 485-490.
-
Kondeti VK, Badri KR, Maddirala DR, Thur SKM, Fatima SS, et al. (2010) Effect of _Pterocarpus santalinus_ bark, on blood glucose, serum lipids, plasma insulin and hepatic carbohydrate metabolic enzymes in streptozotocin- induced diabetic rats. Food and Chemical Toxicology 48(5): 1281-1287.
-
Prabakaran D, Ashokkumar N (2012) Antihyperglycemic effect of esculetin modulated carbohydrate metabolic enzymes activities in streptozotocin induced diabetic rats. Journal of Functional Foods 4(4): 776-783.
-
Kritikar KR, Basu BD (1993) Indian Medicinal Plants. Orient Enterprises, Dehradun, pp: 496-498.
-
Longman O (1994) Indian Medicinal Plants. Orient Longman Ltd., Madras, India, pp: 157-159.
-
Nadkarni AK (1954) Indian Materia Medica. 3rd(Edn.), Popular Prakashan, Bombay, India, pp: 114.
-
Puspangadan P, Atal CK (1984) Ethno-medico-botanical investigations in Kerala I. Some primitive tribals of Western Ghats and their herbal medicine. Journal of Ethanopharmacol 11(1): 59-77.
-
Setty BS, Kamboj VP, Garg HS, Khanna NM (1976) Spermicidal potential of saponins isolated from Indian medicinal plants. Contraception 14(5): 571-578.
-
Devi G, Kapil RS, Popili SP (1978) Chemical Investigation of _Anisomeles malabarica_. Indian journal of chemistry 15: 441.
-
S Reitman, S Frankel (1957) A colorimetric method for the determination of serum glutamic oxalacetic and glutamic pyruvic transaminases. American journal of clinical pathology 28(1): 56-63.
-
Bessey OA, Lowky OH, Brock MJ (1946) A method for the rapid determination of alkaline phosphatase with five cubic millimeters of serum. The Journal of Biological Chemistry 164: 321-329.
-
Powell WN (1944) A method for the quantitative determination of serum bilirubin with the photoelectric colorimeter. American journal of clinical pathology 14: 55-88.
-
Slot C (1965) Plasma creatinine determination a new and specific Jaffe reaction method. Scandinavian Journal of Clinical and Laboratory Investigation 17(4): 381-387.
-
Wybenga DR, Giorgio JD, Pileggi VJ (1971) Manual and automated methods for urea nitrogen measurement in whole serum. Clinical chemistry 17(9): 891-895.
-
Fraga CG, Leibovitz BE, Tappel AL (1988) Lipid peroxidation measured as thiobarbituric acid-reactive substances in tissue slices: characterization and comparison with homogenates and microsomes. Free Radical Biology and Medicine 4(3): 155-161.
- Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review