Cost-Effectiveness Analysis of Biologics in the Treatment of Moderate-to-Severe Plaque Psoriasis from a Health Care Provider's Perspective
Introduction: Psoriasis (psoriasis) is a chronic disease with a number of significant comorbidities and often with a very significant impact on the quality of life of patients. Recently, a relatively large number of biological treatment products with a significant effect have entered the market, but they are also significantly more expensive than systemic conventional treatment. In the context of the published long period of inadequate treatment of patients with psoriasis in the Czech Republic, the health care system and the limited costs of center drugs, it is necessary to make the greatest possible effort at the level of the provider of this health care to effectively spend financial resources and provide highly effective treatment to the greatest possible number of patients. Method: With a model-set amount of the unit prices of the packaging of preparations according to the maximum reimbursements in the Czech Republic in 2021, a fictitiously set amount of bonuses for only two selected preparations (this is a model example that does not reflect the real state of business policy at the University Hospital Olomouc), and the conditions for reimbursement of biological treatment preparations psoriasis in the Czech Republic in 2021, a cost-effectiveness analysis (CEA) was carried out in the selected PASI 100 efficiency parameter. The analysis was carried out and processed interactively in the Excel software into the graphical form of the outputs, especially in the form of forest plot graphs (in the CER and ICER parameters) and in a two-dimensional efficient frontiers graph (costs vs. efficiency). Results: The differences in the cost-effectiveness of individual preparations according to the point values of the CER and ICER parameters are up to several times. Taking into account the 95% confidence intervals, some of the differences between the preparations are also statistically significant. With the most cost-effective sequence of treatment for a gradually more effective drug in one patient during the induction period of treatment, we can, based on the saved costs, start induction treatment with a less effective biologic in two more patients than when using the second cost-effective sequence of treatment escalation. Conclusion: The cost-effectiveness analysis (CEA) of biological drugs in the treatment of psoriasis at the level of the health service provider has great potential in the effort to make the treatment as effective as possible with limited financial resources, or in the effort to provide effective treatment to additional patients with the same limitations.
Introduction
Psoriasis (psoriasis) is a chronic inflammatory disease with typical skin symptoms. We include it in the group of immune-related diseases. From an etiopathogenetic point of view, psoriasis is viewed not only as a purely skin disease, but rather as a systemic disease [1]. Worldwide, the prevalence of psoriasis varies between 0.5-11.4 % in adults and 0-1.4 % in children. Prevalence increases with increasing geographic distance from the equator [2]. According to the NZIS report [3], a total of 97,450 patients were treated for psoriasis in the Czech Republic in 2017. However, the total number of patients in the Czech Republic may be up to 300,000, which is also due to the complexity of the exact determination of the diagnosis [4]. It is reported [5, 6] that approximately 70 – 80 % of patients with plaque psoriasis (see below) have a mild form of the disease that can be managed with topical treatment.
The basic manifestation of psoriasis is a slightly raised, bordered papule of red color, which is covered with easily identifiable silvery scales [1]. Hyperproliferation of the skin in patients with psoriasis is characterized in particular by an accelerated renewal of the epidermis (4 days in psoriasis vs. 27 days in normal skin). Psoriatic skin also has abnormal differentiation of keratinocytes manifested by different ratios of individual types of keratin compared to healthy skin. The main clinical types of psoriasis are:
- Chronic focal (plaque) psoriasis (is the most common form, accounting for 55 - 79 % of cases).
- guttate psoriasis.
- pustular psoriasis.
- erythrodermic psoriasis [2].
Psoriasis patients also often have various comorbidities, e.g.: psoriatic arthritis (may be present in up to 30 % of psoriasis patients), depression (up to 10 % of patients), metabolic syndrome, type 2 diabetes mellitus, chronic renal insufficiency (in moderate severe to severe psoriasis), ocular manifestations (e.g. blepharitis, conjunctivitis, uveitis) [2, 7].
Psoriasis is a genetically determined disease, other risk factors are certain environmental and lifestyle factors (e.g.: smoking, obesity, alcohol use, certain medications). In the past, psoriasis was perceived as a disease caused by hyperproliferation, now it is understood as a complex disease with a complex interaction (controlled by cytokines - eg: TNFα, IL-12, IL-17, IL-22, IL-23) between the cells of the immune system (especially dendritic cells and T-lymphocytes) and keratinocytes [1, 2, 8].
The following scoring systems [6, 9, 10] are most often used to assess the severity of psoriasis – the first three (listed below) are assessed by healthcare professionals, the last is assessed by the patient:
- PASI (Psoriasis Area and Severity Index), the value ranges from 0 to 72, a value above 10 means moderate to severe psoriasis, above 20 means very severe psoriasis.
- BSA (Body Surface Area), a value above 10 % means severe psoriasis.
- PGA (Physician Global Assessment), the value usually ranges from 0 to 7, possibly up to 6 or 5, a value of 3 or more usually means moderate to severe psoriasis.
- DLQI (Dermatology Life Quality Index), the value ranges from 0 to 30, a value higher than 5 means a moderate effect on the quality of life, a value above 10 means a large impact of psoriasis on the patient’s quality of life.
The PASI score is also used as a parameter of treatment response [11] in this case the value is then reported as a percentage response rate (e.g. PASI 75 means achieving a 75 % or greater reduction in the initial PASI score before treatment, PASI 100 means achieving complete healing of skin lesions). Achieving PGA 0/1 is also often used as a parameter for successful treatment [10].
In mild forms of psoriasis, treatment is usually started with local agents (e.g. corticosteroids, vitamin D3 derivatives, tars, ichthamol, cignolin), in moderate to severe psoriasis, light treatment (NBUVB, PUVA or re-PUVA) or systemic treatment with combination of local therapy [9] (Figure 1).
Systemic treatment can be divided into [8, 10]:
- conventional (e.g. cyclosporine, methotrexate, acitretin).
- targeted via “small molecules” (e.g. PDE4 inhibitor (e.g. apremilast), JAK inhibitors (e.g. deucravacitinib, tofacitinib).
- targeted through biological drugs (currently: anti-TNFα, anti-IL 12/23, anti-IL 17 and anti-IL 23 preparations).
According to the recommendations of the EuroGuiDerm group [10], it is now possible to start the treatment of severe psoriasis with so-called “first-line” biologics, if the insufficient effect of conventional systemic treatment can be assumed (Figures 2 & 3).
![Figure 1: Algorithm for the first-line treatment of moderate to severe focal (plaque) psoriasis without comorbidities (modified according to the French recommendation [12] note CSA (ciclosporin), MTX (methotrexate), NBUVB (narrowband UVB phototherapy), PUVA (psoralen UVA phototherapy), re-PUVA (retinoid, psoralen UVA phototherapy).](/fulltextimages/11334/fig_1.png)
![Figure 2: overview of treatment options for moderate to severe focal (plaque) psoriasis (modified according to the EuroGuiDerm recommendation from 2020 [10] note: phototherapy is not addressed in this recommendation, therefore it is not shown in the picture).](/fulltextimages/11334/fig_2.png)
An explanation must be attached to Figure 2 that apremilast is not (as of 18/09/2021) reimbursed for psoriasis in the Czech Republic [13] and according to the reimbursement conditions in the Czech Republic (as of 18/09/2021) biologics cannot be used for psoriasis alone, without meeting the conditions listed below, can be used as 1st line systemic treatment [13] they can be used in the treatment of psoriasis with a PASI of more than 10 in adults where two of the following conventional systemic treatments cannot be used: acitretin, methotrexate, ciclosporine or phototherapy (PUVA or NBUVB) due to lack of effectiveness, intolerance or contraindications. The conditions for treatment termination or direct transfer to another biologic (except for termination due to an adverse effect) are as follows in the Czech Republic [13] failure to reach the PASI 50 value (for anti-TNFα and ustekinumab) or PASI 75 (for anti-IL 17 and anti-IL 23) after 16 weeks of treatment (after 12 weeks only for etanercept) or a decrease in the effectiveness of the established treatment below PASI 50 or with effectiveness in the PASI 50-75 interval, if the DLQI value is > = 5 at the same time.
![Figure 3: evidence for the use of specific systemic treatment in psoriasis under different clinical conditions (modified according to the Belgian recommendation [36]).](/fulltextimages/11334/fig_3.png)
Anti-IL 12/23, anti-IL 17 and anti-IL 23 preparations can also be used in the Czech Republic as next-line biological treatment preparations for psoriasis with a PASI of more than 10 in adults [13] under the condition that a PASI value of 50 has not been reached after 3 or 4 months (depending on the type of product) of previous biological treatment; or there has been a decrease in the effectiveness of the established biological treatment below PASI 50 or with effectiveness in the interval PASI 50-75, if at the same time the DLQI value is >= 5; or another biological treatment is contraindicated, or the previous biological treatment is discontinued due to an adverse effect.
Anti-TNFα preparations, as well as secukinumab with ixekizumab, are additionally reimbursed in the Czech Republic as of 18/09/2021 [13] for adult patients with psoriasis with a PASI of more than 10 who simultaneously have active psoriatic arthropathy, where methotrexate cannot be used due to insufficient effectiveness, intolerance or contraindications. Ustekinumab and guselkumab can also be used in patients with psoriasis and current active psoriatic arthropathy according to the SPCs as of 18/09/2021 [13], but this option is not explicitly stated in the reimbursement conditions for the given product in the Czech Republic.
As of 31 December 2020, a total of 2,474 patients were treated with biological or targeted treatment for psoriasis in the Czech Republic, a total of 366 patients [14] started their first biological or targeted treatment in 2020.
Due to the wide portfolio of biological treatment products that can be used in the Czech Republic for moderate to severe psoriasis (hereinafter referred to as “psoriasis”), and also due to the fact that their price is higher than that of conventional products, and that their prescription is tied to specialized care centers, only the biological treatment preparations themselves were selected for our cost- effectiveness evaluation. The perspective of the health care provider was chosen due to the different methodology used for pharmacoeconomic analyzes carried out by SUKL (State Institute for Drug Control in Czech Republic - this is the perspective of the insurance payer) [5], the maximum reimbursement amount of the product set by SUKL may also exceed the real prices at a specific provider due to, for example, individually agreed bonuses falling under trade secrets [15]. Biological treatment preparations are billed as a separately billed preparation to the health insurance company only by specialized workplaces, on the basis of a contract concluded between them and the health insurance company [13], these centers of specialized care also have a limited annual budget determined by the reimbursement legislative [15].
The aim of our work is to verify the hypothesis that the model chosen by us for the analysis of the cost-effectiveness of biological drugs indicated and reimbursed for psoriasis (in the context of modeled prices and health care provider bonuses) can clearly quantify the effectiveness of the limited financial resources spent and will allow the creation of a proposal for a treatment escalation algorithm with the aim of enabling the most effective treatment for the greatest possible number of patients at limited costs.
Method
A cost-effectiveness analysis (hereafter referred to as “CEA”) was chosen for the pharmacoeconomic evaluation of biological treatment of psoriasis [16]. The PASI 100 parameter was chosen for mutual comparison of the treatment effect of individual preparations, separately after the induction period (10-16 weeks depending on the preparation) and separately after long-term use (48-52 weeks depending on the preparation) based on the results of an indirect comparison through a network meta-analysis (further just “NMA”), including the indicated 95 % confidence intervals (hereafter “95% CI”) [17]. For etanercept after an induction period of 100 mg weekly for 12 weeks, a PASI 100 value was used based on the results of an indirect comparison through another NMA [18]. Due to the unavailability of data on the efficacy of certolizumab and infliximab after long- term use (48–52 weeks) in the sought-after NMAs, for the purposes of this analysis, the values from PASI 100 achieved after the induction period were taken for these products - the limitations of this assumption are listed below in the Discussion section. Although the reimbursement conditions for biological treatment preparations in the Czech Republic [13] are determined by achieving a PASI value of 50 or 75, only the PASI 100 parameter was selected for this CEA – the reasons for its selection and limitations are given below in the Discussion section.
Comparisons of the effectiveness of individual preparations in the parameter PASI 100 (especially after the induction period and especially after long-term use) were processed in the form of forest plot graphs [19] in the parameter number needed to treat (hereinafter referred to as “NNT”) [20] for PASI 100 and that including 95 % CI. As a supplement to the results from the above-mentioned NMA, an overview of the total number of patients assigned to a given biologic as the 1st, 2nd, or 3rd choice was also processed and the % of patients assigned who were transferred to another biologic, or have completed treatment with the given biologic, based on the data of the Dermatologic Clinic of University Hospital in Olomouc from 2016 to 8/27/2021.
For the purposes of modeling this CEA, the prices for the unit packaging of the preparations were taken from the values of the maximum reimbursements set by SÚKL as of 18/09/2021 [13], and for the purposes of the modeling we used a fictitious bonus of 30% only for Zessly and Hyrimoz brands preparations (this is a model example of a price reduction based on an agreement between the manufacturer and the hospital not reflecting the current situation!). Packages registered, paid for and traded in the Czech Republic as of September 18, 2021 [13] were used as unit packages of preparations. For individual preparations, the total treatment prices for the induction period (i.e. the first
16 weeks of treatment (for etanercept for the first 12 weeks) were calculated, due to the need to evaluate the achievement of a certain percentage PASI after the end of the induction period as a condition for further reimbursement according to the conditions set by SUKL (see above). The total price for treatment with individual preparations was also calculated separately after long-term use (i.e. for one year of treatment (52 weeks), with the dosage maintained in the maintenance regimen throughout this period).
The dosage used to calculate the prices was taken from the recommendations in the SPCs [13] of the individual products and according to the corresponding data on effectiveness [17, 18], in the case of the products listed below with more options, the following dosage was used:
- Stelara (only a dose of 45 mg was chosen for patients up to 100 kg due to reimbursement in the Czech Republic only for dose 45 mg).
- Enbrel (a higher induction dosage of 100 mg per week until the 12th week was chosen because its effectiveness (according to the PASI 100 parameter) is almost 2x higher than with a lower dosage of 50 mg per week).
- Cimzia (both dosage variants chosen, i.e. 200mg or 400mg after the initial 3 doses).
- Humira and Hyrimoz (after an initial dose of 80 mg, a dosage of 40mg every 2 weeks was chosen).
- Inflectra and Zessly (selected 70kg patient weight to calculate the dose of 5mg/kg and also assuming the possibility of dividing doses from one bottle of the preparation).
The results of CEA were processed in Excel software in the form of forest plot graphs [19] in parameters CER [21] and ICER [16] including 95% CI according to PASI 100, separately after the induction period and separately after long-term use. The results of CEA (point values only) were also shown together both after the induction period and after long-term use in a two-dimensional graph (cost vs. effectiveness) with the efficient frontiers lines [22] marked, separately for the induction period and separately for long-term use with with the exception of preparations containing infliximab - because of its specific position among biologic drugs (i.e. administration by IV infusion and the highest frequency of discontinuation of treatment of all compared biologics due to adverse effects - see above). All the above graphs correspond in the Excel software with the corresponding table of unit prices of preparations and bonuses. This enables immediate interactivity and graphic visualization during any change in input variables (i.e. unit prices, bonuses, efficiency data, or addition of a new product). Based on these results, an algorithm of recommended lines of individual biologics was proposed both for patients with only plaque psoriasis and for patients with simultaneously active psoriatic arthropathy, and individual preparations were also compared in terms of advantages vs. disadvantages according to clinical [6, 13, 17, 18, 23] and pharmacokinetic-dynamic parameters [13, 24].
Results
As the most effective biologics in the PASI 100 parameter after the induction period, ixekizumab, risankizumab and brodalumab are very likely (Figure 4) – their NNT point value of 2.5 is approximately the same for all of them (the difference from secukinumab and guselkumab is, however, only on the border of statistical significance), the least effective is most likely etanercept Figure 4. In the PASI 100 parameter after long-term use, risankizimab is very likely the most effective preparation - the NNT point value is 1.5 (the difference from brodalumab and guselkumab is also only at the limit of statistical significance) (Figure 5).
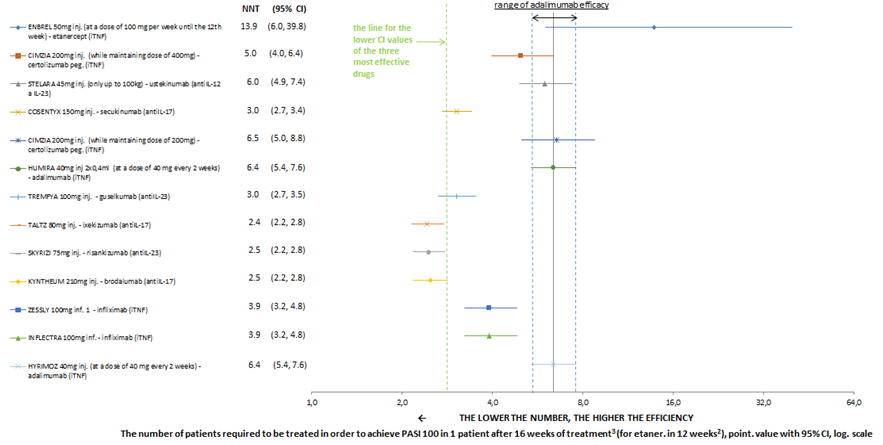
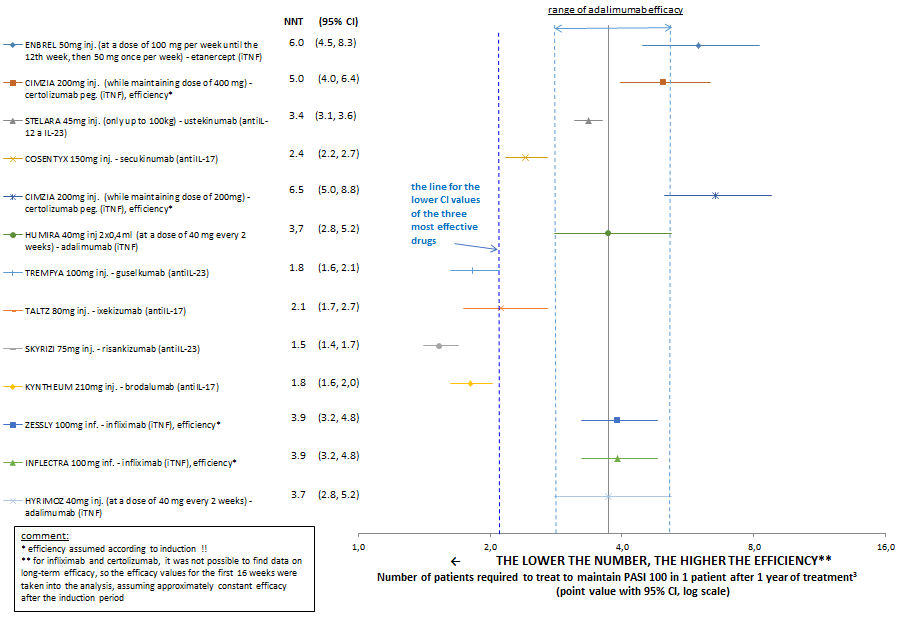
According to the point values, only these three above the listed preparations reach an NNT below 2. The least effective is most likely, as well as after the induction period, etanercept Figure 5. Although certolizumab has NNT values similar to etanercept, the informative value of the result is limited by taking long-term efficacy values as values after the induction period of therapy. Risankizumab (Skyrizi) and brodalumab (Kyntheum) are therefore probably the preparations with the highest efficacy in the PASI 100 parameter both after the induction period and after long-term use. Both charts show that anti-IL-17 and anti-IL-23 preparations are statistically significantly more effective than anti-TNFα preparations (except infliximab) and also than anti-IL 12/23 preparations. Of the anti-TNFα preparations, etanercept is probably the least effective.
product (except for cases of transfer to a biosimilar product and when evaluating only original products for those substances that already have biosimilar alternatives) or from the rates of treatment termination given as 1st- 3rd choice of biologic drug Table 1 follows the following order of patient persistence on treatment (arranged in descending order - for preparations with a small number of patients, a high probability of result distortion must be assumed):
- anti-IL 23 preparations (so far but there are few patients on them, especially on risankizumab).
- anti-IL 17 ixekizumab and brodalumab (he also has few patients so far).
- anti-IL 17 secukinumab, anti-IL 12/23 ustekinumab and anti-TNFα infliximab.
- anti-TNFα adalimumab.
- anti-TNFα etanercept. Certolizumab was not ranked because of the small number of patients.
- From the overview of the number of patients switched at the Olomouc University Hospital to another biological
- 1st choice of witch: number of paitents
- Switch (%) approx. median time to switch
- Termination of treatment (%)
- Switch to biosimilar
- ENBREL (etanercept) inhibiltor TNF alfa
- 34
- 62%
- 16 months
- 15%
- HUMIRA (adalimumab) inhibiltor TNF alfa
- 30
- 57%
- 13 months
- 7%
- 33%
- HYRIMOZ (adalimumad) inhibiltor TNF alfa
- 22
- 14%
- 16 months
- REMICADE (infiliximad) inhibiltor TNF alfa
- 11
- 55%
- 19 months
- 45%
- REMSIMA (infliximmad inhibiltor TNF alfa
- 6
- 67%
- 13 months
- 33%
- INFLECTRA (infliximab) inhibiltor TNF alfa
- 0
- CIMZIA (certolizumab) inhibiltor TNF alfa
- 8
- 25%
- 6 months
- STELERA (ustekinumab) inhibiltor IL-12a
- IL-23
- 12
- 42%
- 22 months
- 17%
- COSENTYX (secukinumab) inhibiltor IL- 17A
- 28
- 25%
- 15 months
- 4% cannot be oounted-only 1 patient switched -
- 15 months
- TALTZ (ixekizumab) inhibiltor IL- 17A
- 9
- 11%
- KYNTHEUM (brodalumab) inhibiltor IL- 17A
- IL-17F a IL-25
- 6
- 33%
- 17 months
- TREMFYA (guselkumab) inhibiltor IL-23
- 8 median usage: 8 months
- 50%
- SKYRIZI (risankizumab) inhibiltor IL-23
- 3 median usage: 21 months
Table 1: Overview of patients placed on biological treatment as 1st, 2nd or 3rd choice at the University Hospital in Olomouc.
According to the total price of drug therapy for the induction period of treatment (i.e. the first 16 weeks of treatment (with etanercept for the first 12 weeks), the cheapest drug is Hyrimoz (adalimumab) in the amount of CZK 42,318 (Table 2), the cheapest drug other than anti- TNFα of preparations is Kyntheum (brodalumab) in the amount of CZK 120,721 (i.e. almost 3 times more expensive than Hyrimoz), the most expensive preparations are Taltz (ixekizumab), Cosentyx (secukinumab) and Skyrizi (risankizumab) in the amount of approximately CZK
210,000 for the first 16 weeks of treatment. According to the total price of therapy with the product after long-term use (i.e. for a year of treatment (52 weeks) with a dosage in the maintenance regimen maintained throughout this time), the cheapest product is Zessly (infliximab), but due to the specific position of infliximab among biologics (i.e. administration in the form of i.v. infusion and the highest frequency of discontinuation of treatment of all compared biologics due to adverse effects) will be the most commonly used preparation in terms of frequency of administration, second in order Hyrimoz (adalimumab), in the amount of CZK 110,027 Table 2. The cheapest product other than anti- TNFα preparations is Stelara (ustekinumab) in the amount of approx. 270,000 CZK (i.e. it is approx. 2.5 times more expensive than Hyrimoz), followed by other non-anti-TNFα preparations in the same amount of approx. 310,000 CZK.
| The Name of the Drug | Active Substance | Mechanism of Action | Price of Maintainance Treatment for 1 Patient/ Year Including Crediting of Bonuses (According to Doses in the SPCs or in Parenthesis Next to the Name of the Drug) | Price for the First 16 Weeks of Treatment (Etanercept for 12 Weeks) for 1Patient Including Crediting of Bonuses (According to Doses in SPC s) |
|---|---|---|---|---|
| HYRIMOZ 40 mg inj. (at a dose of 40 mg every 2 weeks after an initial dose of 80 mg) | adalimumab | inhibitor TNF-alfa | 110 027 Kc | 42 318 Kc |
| INFLECTRA 100mg inf. 1x100mg (prices are for a 70 kg patient, when dividing inj. Bottle) | infliximab | inhibitor TNF-alfa | 133 363 Kc | 82 070 Kc |
| KYNTHEUM 210 mg. inj. 2x1,5ml | brodalumab | inhibitor IL-17A, IL-17F a IL-25 | 313 874 Kc | 120 721 Kc |
| TALTZ 80mg inj. 2x1 ml | ixekizumab | inhibitor IL-17A | 313 879 Kc | 217 301 Kc |
| ZESSLY 100mg inf. 1x100mg (prices are for a 70 kg patient, when dividing inj. Bottle) | infliximab | inhibitor TNF-alfa | 93 354 Kc | 57 449 Kc |
| TREMFYA 100mg inj. 1x1ml | guselkumab | inhibitor IL-23 | 313 876 Kc | 144 866 Kc |
| COSENTYX 150 mg inj. 2x1ml | secukinumab | inhibitor IL-17A | 314 737 Kc | 209 824 Kc |
| HUMIRA 40mg inj 2x0.4ml (at a dose of 40mg every 2 weeks after an initial dose of 80 mg) | adalimumab | inhibitor TNF-alfa | 157 181 Kc | 60 454 Kc |
| ENBREL 50mg inj. 4x1ml ( at a dose of 100mg per week until the 12th week, 50 mg once per week) | etanercept | inhibitor TNF-alfa | 158 178 Kc | 72 543 Kc |
| STELARA 45 mg inj. 1x0.5ml (only a dose of 45 mg was chosen for patients up to 100 kg due to reimbursement a dose of only 45 mg in the Czech Rep) | ustekinumab | inhibitor IL-12 a IL-23 | 267 809 Kc | 185 421 Kc |
| CIMZIA 200 mg inj. 2x1ml (while maintaining dose of 400mg) | certolizumab pe gol | inhibitor TNF-alfa | 157 179 Kc | 72 544 Kc |
| CIMZIA 200 mg inj. 2x1ml (while maintaining dose of 400mg) | certolizumab pe gol | inhibitor TNF-alfa | 314 357 Kc | 108 816 Kc |
| SKYRIZI 75mg inj. 2x0.83ml | risankizumab | inhibitor IL-23 | 305 076 Kc | 210 397 Kc |
Table 2: Therapy prices for the induction period and for maintenance treatment for 1 year (Hyrimoz is listed first (for the reaso
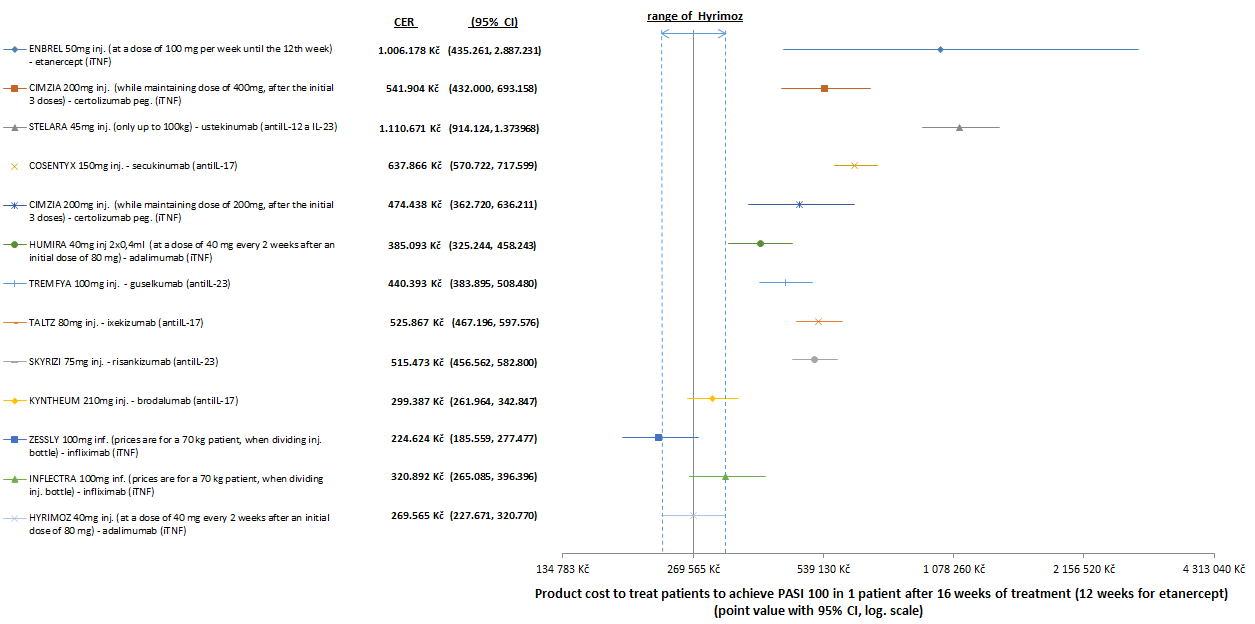
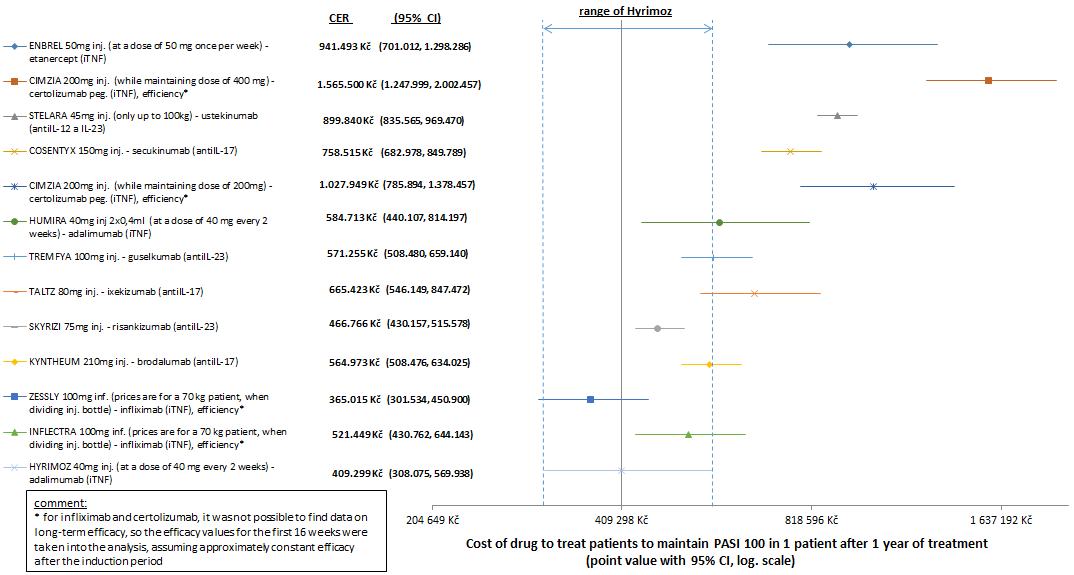
When comparing the cost-effectiveness of the preparations in the CER parameter (i.e. the total price spent on treating patients with a given preparation to achieve PASI 100 in 1 patient after 16 weeks of treatment (for etanercept in 12 weeks), respectively the total price for maintaining PASI 100 in 1 patient after 1 year of treatment) is the most cost-effective according to the point values, after excluding products with infliximab, always Hyrimoz (adalimumab), both after the induction period (CER = 269,565 CZK / PASI100 Figure 5 and after long-term use (CER = CZK 409,299 / PASI 100 Figure ). After the induction period, Hyrimoz (adalimumab), after excluding products with infliximab, is statistically significantly more cost-effective in the CER parameter than the other products, except for Kynthea (brodalumab) - but this is almost 3 times more expensive than Hyrimoz Figure 10. After long-term use, Hyrimoz (adalimumab), after excluding infliximab preparations and other adalimumab preparations, is statistically only insignificantly more cost-effective in the CER parameter than Skyrizi (risankizumab), Kyntheum (brodalumab), Tremfya (guselkumab) and Taltz (ixekizumab) - those but they are almost 3 times more expensive than Hyrimoz (Table 2) and (Figures 6 & 7).
Hyrimoz (adalimumab) is therefore the cheapest and most cost-effective preparation in the CER parameter in our model, after excluding preparations with infliximab. When comparing the cost-effectiveness of the preparations through ICER to Hyrimoz, namely to its point value of effectiveness in PASI 100, after the induction period, excluding preparations with infiximab, Kyntheum is statistically significantly more cost-effective (brodalumab – its point value ICER = CZK 318,400 / PASI 100 (Figure 8). Next in order, Tremfya (guselkumab), Skyrizi (risankizumab) and Taltz (ixekizumab) have an ICER point value for Hyrimoz approx. 2x higher than Kyntheum. In terms of costs for the duration of induction treatment, however, Tremfya is only about 24,000 CZK more expensive than Kyntheum, while Skyrizi and Talz are about 90,000 CZK, respectively CZK 96,000 more expensive than Kyntheum Table 2.
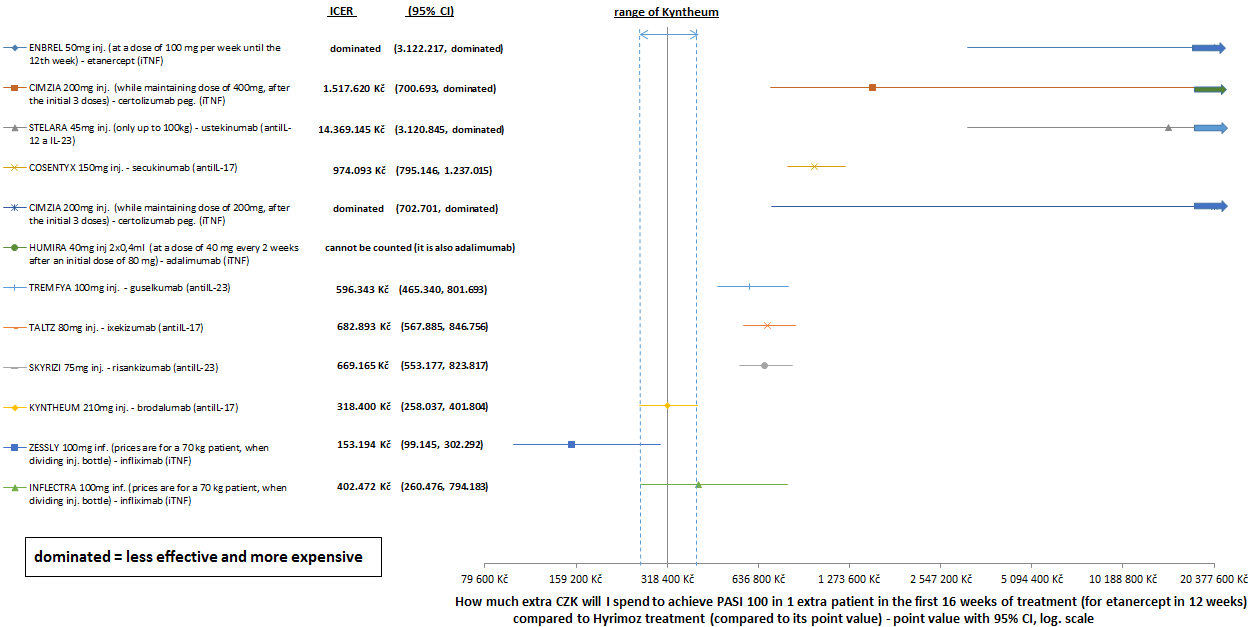
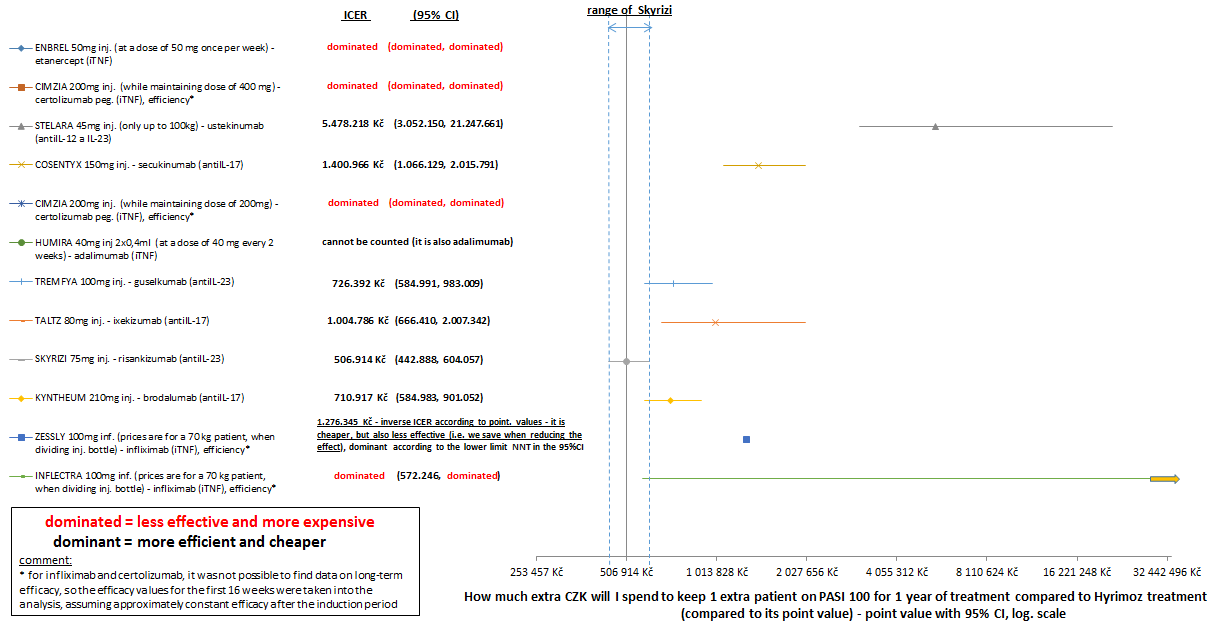
After long-term use, again excluding preparations with infiximab, Skyrizi is statistically almost significantly more cost-effective (risankizumab - the ICER point value compared to treatment with Hyrimoz is CZK 506,914 / PASI 100 (Figure 9) and compared to others in the order of Kyntheum (brodalumab) and Tremfya (guselkumab) has an ICER of more than CZK 200,000 / PASI 100 lower. The price of a one-year maintenance treatment with Skyrizi is even about CZK 8,000 cheaper than treatment with Kyntheum or Tremfya (Table 2 and Figure 10). The ICER parameter in our model can be interpreted as follows: “how many extra CZK will I spend to achieve PASI 100 in 1 extra patient in the first 16 weeks of treatment (for etanercept in 12 weeks), or how many CZK will I spend extra to keep 1 extra patient on PASI 100 for 1 year of treatment compared to treatment with Hyrimoz”.
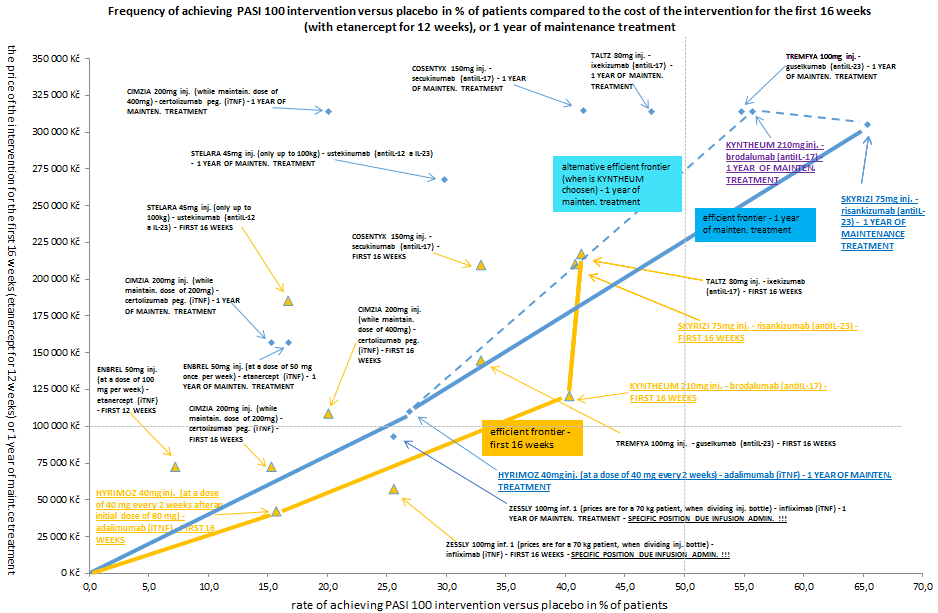
Figure 10: cost-effectiveness of biologics in a two-dimensional graph (cost vs. effectiveness) with efficient frontiers (yellow color and triangle marks indicate the induction phase of treatment, blue color and diamond marks indicate maintenance treatment, blue dashed line indicates the inclusion of KYNTHEUM as a 2nd-line drug after HYRIMOZ due to the result of the line of effectiveness after the induction phase of treatment, the underlined preparations indicate the preparations belonging to the most cost-effective - with the exception of preparations containing infliximab due to its specific position among biologics (for the reasons, see the text in the Results section).
Based on the above mentioned results of our model, it is possible to propose the most cost-effective sequence of administration lines of individual biologics (i.e. escalation of treatment) both for patients with plaque psoriasis only (hereinafter referred to as “without PsA”) and for patients with simultaneously active psoriatic arthropathy (hereinafter referred to as “with PsA”) (Table 3). The preparation Hyrimoz (adalimumab) can be proposed as a first-choice preparation both in patients without PsA and in patients with PsA - adalimumab is also listed among the first-line biological treatment preparations according to the EuroGuiDerm recommendation from 2020 [10] (Figure 2) Zessly, although according to the CER point values it is approximately 1. –1.25x more cost-effective than Hyrimoz (Table 3), but only statistically insignificant Chart 3 and Chart 4 and with maintenance treatment in 1 year is even cheaper than Hyrimoz, it should only be used in patients with the impossibility of administration or the ineffectiveness of Hyrimoz (e.g. due to the high frequency of administration of maintenance doses, or due to the need to achieve a rapid onset of effect (Table 4), and this when accepting IV administration by the patient. With Zessly, this recommendation is proposed due to its specific position (i.e., it is the only biologic that is administered by IV infusion and has the highest frequency of discontinuation of treatment due to adverse effects of all compared biologics [23], infliximab is also listed among second-line biological treatment preparations according to EuroGuiDerm recommendations from 2020 [10] (Figure 2). In case of ineffectiveness or intolerance of Hyrimoz, or Zessly, Kyntheum (brodalumab) is offered as the 2nd choice of biologic for patients without PsA, and Skyrizi (risankizumab) as the 3rd choice (Table). In case of ineffectiveness or intolerance of Hyrimoz, or Zessly, Tremfya (guselkumab) is offered as the 2nd choice biologic for patients with PsA and Taltz (ixekizumab) as the 3rd choice (Table 3).
| The Name of the Drug | Active Substance | Multiple of the Cost/Effectiveness Ratio Compared to HYRIMOZ (According to Point Values) During Maintainance Treatment for 1 Year (CER = Price for Maintainance of 1 Patient for PASI 100 for 1 Year of Treatment | Multiple of the Cost/Effectiveness Ratio to HYRIMOZ (According to Point Values) in the First 16 Weeks of Treatment For Etanercept in 12 Weeks (CER = Price for Achieving PASI 100 In 1 Patient in 16 Weeks of Treatment | Treatment Options According to Modelling Results (Patient with Plaque Psoriasis only (Here in after Referred to as “Without Psa”) and for Patients with Simultaneously Active Psoriatic Arthropathy (Here in After Referred to as “with PsA”) |
|---|---|---|---|---|
| HYRIMOZ 40mg inj. (at a dose of 40 mg every 2 weeks after an initial dose of 80 mg) | adalimumab | 1 (409.299 CZK) | 1 (269.566 CZK) | 1st with PsA and also without PsA |
| INFLECTRA 100mg inf. 1x100mg (prices are for a 70 kg patient, when dividing inj. Bottle) | infliximab | 1.3 | 1.2 | switch to the cheaper biosimilar Zesslyl |
| KYNTHEUM 210mg inj. 2x1.5ml | brodalumab | 1.4 | 1.1 | 2nd without PsA |
| TALTZ 80mg inj. 2x1ml | ixekizumab | 1.6 | 2 | 3rd with PsA 5th without PsA |
| ZESSLY 100mg inf. 1x100mg (prices are for a 70kg patient, when dividing inj. bottle) | infliximab | 0.9 | 0.8 | 1st exceptionally only in a certain from of psoriasis, otherwise 1st with PsA and also without PsA if Hyrimoz cannot be used |
| TREMFYA 100mg inj. 1x1ml | guselkumab | 1.4 | 1.6 | 2nd with PsA (PsA itself is not reimbursed in the Czech Republic) 4th without PsA |
| COSENTYX 150mg inj. 2x1ml | secukinumab | 1.9 | 2.4 | 6th without PsA 8th without PsA |
| HUMIRA 40mg inj.2x0.4ml (at a dose of 40mg every 2weeks after an initial dose of 80mg) | adalimumab | 1.4 | 1.4 | switch to the cheaper biosimilar Hyrimoz ! |
| ENBREL 50mg inj. 4x1ml (at a dose of 100mg per week until the 12th week, then 50mg once per week) | etanercept | 2.3 | 3.7 | 1st exceptionally only in a certain from of psoriasis, otherwise 7th with PsA, 9th withut PsA |
| STELARA 45mg inj. 1x0.5ml (only a dose of 45mg was chosen for patients upto 100kg due to reimbursement a dose of only 45mg in the Czech Rep) | ustekinumab | 2.2 | 4.1 | 8th with PsA (PsA itself is not reimbursed in the Czech Republic) 10th without PsA |
| CIMZIA 200mg inj. 2x1ml (while maintaining dose of 200mg) | certolizumab pegol | 2.5 | 1.8 | 4th with PsA 6th without PsA |
| CIMZIA 200mg inj. 2x1ml (while maintaining dose of 400mg) | certolizumab pegol | 3.8 | 2 | 5th with PsA 7th without PsA |
| SKYRIZI 75mg inj. 2x0.83ml | risankizumab | 1.1 | 1.9 | 3rd without PsA |
Table 3: A proposal for the most cost-effective escalation of biological treatment according to our model (Hyrimoz is listed in f
Table 3: A proposal for the most cost-effective escalation of biological treatment according to our model (Hyrimoz is listed in first place (see the Results section for the reasons for its priority), the ordering of the other preparations in the table is random and does not reflect the order of preference, the order of escalation of the preparations is given in the last column!).
| Benefits | Disadvantages | |
|---|---|---|
| Ustekinumab | * Maintenance dose every 12 weeks (along with risankizumabthe longest interval of all biologics)*Less servere Aes than IL-17i (expect for malignancies) and TNFi | * The effectiveness is lower than that of IL-23 Inhibitors -about the level of adalimumab and certolizumab (both are TNFi) |
| Ixekizumab | * Very high efficacyin the induction phase (together with brodal. and risank. the highest), maintenance dose every 4 weeks*Probably the 2nd fastest onset of effect (approx. 24% of patients achieved PA SI 90 after brodalumab * From IL-17Ai and IL-23I (i.e the most effective biological drug ) can be used in psoriasis with PsA | * The initial dosage has a total of 7 doses (one dose every 2weeks)* Of the most effective biological drugs (i.e risankizumab, guselkumab,ixekizumab,brodalumab and secukinumab) together with risankizumab has the worst coste/effective ratio in the model for the first 16 weeks of treatment after secukinumab |
| Secukinumab | * High efficiency (probably the 2nd highest after other IL-17i and IL-23i), maintenance dose every 1 month* From IL-17Ai and IL-23i(i.e the most effective biological drugs ) it can be used in psoriasis with PsA * Biological drugs with the 2nd longest biological half time * Probably 4th fastest onset of effect (approx 13% of patients achieved PASI 90after brodalumab , ixekizumab and in fliximab | * The initial dosage a total of 5doses (1 dose every week)* Of the most effective biological drugs (i.e risankizumab, guselkumab,ixekizumab,brodalumab and secukinumab) probably has the worst price /performanceratio in the model for the first 16 weeks of treatment , as well as in the maintenance phase |
| Brodalumab | * Very high efficacy both in the introduction and in the maintenance phase (together with risankizumab )*Probably the fastest onset of effect (approx 29% of patients achieved PA SI 90 after 4 weeks) of all biologics * In the introduction phase it is significantly cheaper than similarly effective risankizumab and ixekizumab | * 2nd highest frequency of administration of a maintenance dose from biologic drugs (every 2 weeks) after etanercept * From IL-17Ai and IL-23i(i.e the most effective biological drugs) it cannot be used in psoriasis with PsA* Probably a higher incidence of AEs than IL-23i ( guselkumab and risankizumab)* Possible increased risk of suicides? |
| Guselkumab | * Very high efficiency in maintenance phase (probably the 2nd highest with brodal. after risank.), maintenance dose every 8 weeks * Probably the lowest occurrence of SAE from biological drugs ( together with risankizumab- both are IL-23i) * From IL-17Ai and IL-23i ( i.e the most effective biological drugs ) it can be used in psoriasis with PsA | * In clinical practice it is sa shorter than IL-17Ai and ustekinumab ( has less clinical data on efficacy and safety) * Has a slower onset of action than brodalumab and ixekizumab (about 8x smaller PA SI 90 rate in 4 weeks), therefore has lower effectiveness after introduction than brodalumab, risankizumab and ixekizumab) |
| Risankizumab | * Very high efficiency both in the introduction and in the maintenance phase ( together with brodalumab) * maintenance dose every 12 weeks ( together with ustekinumab the longest interval among biologic drugs) * Probably the lowest occurrences of significance AEs among biologic drugs (together with guselkumab), biological drug with longest half-life | * From the most effective biologic drugs (i.e risank.,guselk., ixek., brodal. and secuk.) has together , with ixekizumab in the model, the worst cost/effectiveness ratio for the first 16 weeks of treatment after secukinumab *From IL-17Ai and IL-23i(i.e the most effective biological drugs) it cannot be usedin psoriasis with PsA * Slower onset of action than brodalumab and ixekizumab ( about 4x smaller PA SI 90 rate in 4 weeks) |
| Infliximab | * Maintenance dose every 8 weeks , good efficacy (probably the most effective of TNFi, efficacy is probably higher than ustekinumab) * After etanercept is together with adalimumab longest in clinical practice* Probably the 3rd fastest onset of effect (approx. 16% of patients achieved PA SI 90 after 4 weeks) after brodalumab and ixekizumab | * Lv infusion ( other biological drugs have a s.c method of administration)* The highest frequency of SAEs and serious infection from biological drugs* IL-17Ai and IL-23i are probably more effective * Unavailable data ( together with certolizumab-attime of authorship of the article)on long-term effectiveness |
Table 4: Comparison of benefit/ risk of individual biologic drugs (highlighted preparations in color indicate preparations belong
Discussion
The mutual comparison of the treatment effect of individual biological preparations in psoriasis was carried out on the basis of published results of indirect comparisons through selected NMAs [17, 18], due to the lack of randomized controlled studies of direct comparison (hereinafter referred to as “RCT”) of all biological treatment preparations with each other. NMA allows comparisons of interventions that were not directly compared in RCTs, but it should be remembered that the level of evidence between outcomes and individual interventions is not the same [10]. NMA has the position of an observational study in the EBM system, so it is on a lower level of the ladder according to EBM evidence than RCT [25], but in the absence of RCT it is the highest strength of evidence. NMA produces estimates of the relative effects between any pair of interventions in a network and usually provides more precise estimates than a single direct or indirect estimate [26], but several conditions must be respected: homogeneity, transitivity, and consistency [25]. The NMA published in 2021 [17] was selected for the following reasons: the inclusion of all biological treatment preparations used in the Czech Republic in the dosage according to the SPCs [13], the publication of results separately after the induction period and separately after long-term use and the inclusion of the largest number of RCTs, which thereby they increase the statistical power of the resulting NMA. For etanercept only after an induction period of 100 mg weekly for 12 weeks, the value from another NMA [18] published in 2019 was used, as this intervention at 100 mg weekly was not evaluated in a previous NMA [17]- inclusion of this one result from the NMA [18] among other results of the previous NMA [17] was made based on the results of a comparison of the values related to etanercept after the induction period at a dose of 50 mg weekly for 12 weeks between both NMAs in the parameter PASI 75, 90 and 100, which were very similar (differences were only approx.: 3 %, 7 % and 11 % respectively. The main limitation of both of these NMAs is, of course, the assumption of transitivity [17].
The order of preparations according to the patient’s duration of treatment from the data of the Dermatology Clinic of University Hospital Olomouc from 2016 to 27 August 2021 listed in Table No. 1 can, with certain limitations, serve as complementary “real world evidence” [27] to the results of the above-mentioned NMA. The most robust data from University Hospital Olomouc are, of course, for anti-TNFα preparations (except certolizumab) - in total, more than 60% of patients from evaluated biologics at University Hospital Olomouc were prescribed an anti-TNFα preparation in the 1st to 2nd line. For substances with already used biosimilar preparations (i.e. adalimumab and infliximab), only original preparations were taken into account for the evaluation of the order of preparations, because (in contrast to biosimilars) for the greater part of the time of their use (or deployment) more effective non-preparations were not yet available on the market anti-TNFα preparations – that is why I assume their use for a wider range of patients (even with severe forms of psoriasis) compared to biosimilar preparations that were introduced later, which no longer had to be used for such a wide range of patients. Even assuming a very likely distortion of the results for some preparations with a small number of patients (especially risankizumab and then also brodalumab), these data from University Hospital Olomouc roughly correlate with the results of the NMA processed in Figure 4 and Figure 5.
Cost-effectiveness analysis (hereinafter referred to as “CEA”) [16] was chosen as a type of pharmacoeconomic analysis in psoriasis for the following reasons:
- this is a comparison of different but comparable interventions (biological treatment) within one disease.
- The benefit (effect) of these interventions is clearly defined in the form of percentage PASI for this disease with sufficiently robust data from the point of view of evidence.
- assessment of the achievement of a certain percentage of PASI after the end of the induction period is a condition for reimbursement by health insurance companies in the Czech Republic.
- according to published studies and the NMA [6, 23], the frequency of discontinuation of treatment with a biologic due to adverse effects was overall very low (always up to 3 %, except for infliximab, which had 5-7 %) and was not statistically significantly different from placebo (except for infliximab and ixekizumab, which was only marginally worse than placebo), which made it possible not to include this parameter in the pharmacoeconomic analysis due to low significance, but instead to use only the efficacy parameter for CEA.
- Possible side effects resulting from the long-term use of biologicals (e.g. total mortality, serious CV events, malignancies, serious infections) were not included in the CEA due to their low incidence according to the results of the PSOLAR report from 2016 [6] specifically: all of them had an incidence below 1 per 100 patient-years, except for serious infections, which had an incidence of approx. 1-3 per 100 patient-years depending on the type of preparation.
From the possible percentage PASI values, PASI 100 was chosen for the following reasons:
- among the vast majority of biological treatment preparations for psoriasis (except for ustekinumab and partly also certolizumab), the differences between them in effectiveness increase in proportion to the increasing value of the PASI percentage both after the induction period and after long-term use [17, 18], so that at PASI 100 they are the difference in efficacy between the preparations is the highest (e.g. when comparing the preparations to adalimumab, the differences in efficacy between PASI 75 and PASI 50 after the induction period are approx. 1.1 times greater, between PASI 100 and PASI 75 both after the induction period and after long-term use, then approx. 1.2 – 1.9 times greater).
- although the reimbursement conditions for biological treatment products in the Czech Republic [13] are determined by reaching a PASI value of 50 or 75 (depending on the type of product) after the induction phase, and the current treatment goals in Europe [10] are also either PASI 75 and above or PASI between 50- 75 and at the same time DLQI below 5; a PASI 90 to 100 may represent the best meaningful clinical response instead of a PASI 75, especially in patients with very severe psoriasis, i.e., an absolute PASI of 20 or more [28].
CEA costs included only the prices for unit packages of preparations according to the maximum payments as of 18/09/2021 [13] (for two selected preparations also including the modeled fictitious amount of the financial bonus applicable only to these preparations, it must be emphasized that the modeled situation does not reflect the real state of the business policy at the University Hospital Olomouc!) because of the same method of administration of all biological preparations (except preparations with infliximab) by s.c. method. This means that we can assume roughly the same amount (and relatively low) of other direct medical costs associated with the application of these preparations, except for preparations with infliximab – with them, due to their IV method of administration, other costs associated with their administration were also not included, but when evaluating the results of the CEA analysis, these preparations were divided separately as specific preparations (see above in the Methodology section). In addition, the amount of these other direct medical costs associated with s.c. application of biologics are considered insignificant in relation to the price of the preparation itself. For the only one of the biologics administered in IV form (infliximab, specifically for the cheapest modeled Zessly), the ratio of the price associated with one application of the product to the price of the product itself (one dose) would be only about 11 % - the cost of IV administration of the biologic (including premedication) are assumed to be approximately CZK 1,600 for 1 infusion according to modeling from 2014 [29]. Whereas the initial variability of the effectiveness parameter PASI 100 compared to its point value for the analyzed biologics (except etanercept) during the induction period amounts to approximately ± 12 to 33 % depending on the type of biologic Figure 4.
Treatment costs for side effects were also not included in the total costs due to the low incidence of serious side effects or serious infections according to RCT results [6, 30]. These results [6, 30] were not significantly different from placebo, except for certolizumab at a higher dosage and infliximab in the case of serious side effects (the frequency compared to placebo was only slightly increased in both cases), then in the case of serious infections with infliximab (the frequency compared to placebo here was significantly increased) and partially also with adalimumab (however, the frequency compared to infliximab was approx. 6 times lower). The amount of costs associated with the treatment of side effects was also considered to be insignificant in relation to the price of the product itself. As an example, it is again mentioned the preparation Zessly (infliximab), because it is the preparation with the highest frequency of serious infections (specifically in 6 % of patients during induction [30]) and at the same time one of the lowest costs (when calculating the price of the preparation itself) spent on induction period – 57,449 CZK Table 2: at a price of approx. 29,000 CZK for the treatment of a respiratory infection [29], the share of the price associated with the treatment of a serious infection (at the above-mentioned frequency of 6 %) compared to the price of treatment with the Zessly preparation itself for the induction period will be only 3%.
Due to the use of only one benefit (effect), namely PASI 100 in our CEA, including 95% CI, no sensitivity analysis, nor validation of the results, was already performed [16]. Due to the calculation of prices for maintenance treatment only for a period of 1 year, no discount rate had to be applied [16].
The advantage of this presented study of cost- effectiveness in psoriasis is the presentation of a method that allows use in general by any provider of health services in the Czech Republic (hereafter referred to as the “provider”), in the context of its real prices of the relevant preparations.
According to the modeling used in our study according to Figure 10 with the marking of the cost-effectiveness lines [22], it follows that if in patients with psoriasis without PsA (with the same amount of budget) we want:
- 1st to provide the most effective treatment of biologic drugs to as many patients as possible, then in the 2nd line after failure or intolerance of anti-TNFα preparations (i.e. Hyrimoz, or Zessly) we will use Kyntheum instead of Skyrizi according to our model - this way we can very likely (assuming tolerance of Kynthea by the patient) when achieving approximately the same effect, save approximately CZK 90,000 for one patient in the first 16 weeks of treatment. Even though annual treatment with Skyrizi in the maintenance dosage is almost 9,000 CZK cheaper than treatment with Kyntheum, hypothetically (assuming long-term constant prices) the costs of using Skyrizi in the induction period would only be “returned” after 10 years of its use in the maintenance dose. But for the effectively “saved” amount of CZK 90,000, we can start treatment with the less effective Hyrimoz in two additional patients in the first 16 weeks.
- 2nd to calculate the distribution of costs for individual preparations in the most efficient way with an unchanged number of patients treated in a given center, then, for example, with an explicit budget of CZK 200,000 per 1 patient per year, it is most cost-effective to have approximately 9 patients on Kyntheum for every 11 patients with Hyrimoz, in in this case, for the given budget amount per 1 patient, we will achieve the highest effect in the form of a PASI 100 percentage rate.
Figure 10 advantageously contains graphically incorporated CER, ICER parameters as well as the amount of costs for individual preparations or sequencing. Specifically: the tangent of the angle between the cost-effectiveness line drawn from point 0 to the point of a specific product and the x-axis (i.e. the efficiency axis) is equal to the CER value of the given product, the tangent of the angle between the cost-effectiveness line drawn from the point of one product to the point of the other product and the x-axis (i.e. the axis of efficacy) is in turn equal to the ICER value of the second preparation against the first [31].
This cost-effectiveness evaluation model created in Excel software enables immediate interactivity and graphical visualization in case of any change in input variables (ie unit prices, bonuses, effectiveness data, or the addition of a new product). This can then very well serve the sales department of the relevant provider as an important basis for further negotiations with the relevant suppliers of biological treatment preparations within the framework of negotiated prices and bonuses covered by trade secrets [15]. As already mentioned above, as of 31 December 2020, a total of 2,474 patients [14] were treated with biological or targeted treatment for psoriasis in the Czech Republic. According to the NZIS report [3], a total of 97,450 patients were treated for psoriasis in the Czech Republic in 2017. With an assumed frequency of 60 % of the occurrence of chronic plaque psoriasis [2] and an assumption of 20 % of the occurrence of a moderate to severe form requiring systemic treatment in patients with plaque psoriasis [5, 6], we arrive at a number of approximately 11,000 patients requiring systemic treatment of psoriasis. According to data from the BIOREP registry [32], in 2019 the average time from diagnosis to the initiation of biological treatment was 21.5 years, in 2020 [33] it was similarly 21.6 years. Mean baseline absolute PASI in 2016 [34] was 19.5 and DLQI 17.0, in 2020 [33] similarly PASI 18.9 and DLQI 16.6 – after 3-4 months of biological treatment the mean absolute PASI was already only 3.9 (this corresponds approximately to an average percentage PASI of 79 after 3-4 months of treatment) and DLQI 3.5. These results clearly point to the long period of insufficient treatment of patients with psoriasis in the Czech Republic, the low quality of life of these patients before the use of biological treatment, and at the same time confirm the excellent effectiveness of biological treatment in psoriasis in real practice [34].
A study from Spain [35] was recently published, which also modeled the optimal sequencing algorithm for the treatment of biologics in psoriasis through CEA in the PASI 100 parameter, but from the payer’s perspective. In contrast to the approach in our analysis, a simulation of treatment over 5 years using 840 different treatment combination sequences was used here, but including fewer biologics than in our analysis (namely without etanercept and infliximab).
From a medical point of view, it must be remembered that the principles of cost-effectiveness cannot be applied strictly in absolute terms. In most cases, it is just another criterion (with a different weight of importance) helping to choose the most optimal preparation for a specific patient, also taking into account other clinical factors – (Table 4) or, for example, (Figure 3) from the Belgian recommendation [36].
A limitation of this analysis is: • Firstly, that in the individual RCTs included in the NMA
[17, 18], the data after long-term use were evaluated after the induction phase (12 to 16 weeks depending on the product) and then after the subsequent maintenance phase, i.e. the total follow-up period was 48–52 weeks according to preparation. In our analysis, I assume the same effectiveness for all preparations only with maintenance dosing for the entire 52 weeks for all preparations - but this assumption was not externally validated in our analysis.
- Second, the PASI 100 parameter used does not cover all aspects of the patient’s quality of life like the DLQI scoring system. However, Torres and Puig [28] report that a decrease in absolute PASI correlates well with a decrease in DLQI, that is, a better quality of life can be very well assumed as percentage PASI increases.
- Thirdly, for the original product and its eventually biosimilar alternatives (i.e. for substances: etanercept, infliximab and adalimumab [13]), was assumed that the transfer (switch) of a stable patient from the original product to a biosimilar or the administration of a biosimilar product to a patient not yet treated with biologicals is safe and effective [37]. It was also assumed that multiple conversions between different biosimilars and the original brand is not preferred but acceptable [37]. These assumptions are partially confirmed by the results from the overview of the limited number of patients switched from the original biological treatment product to its biosimilar product at University Hospital Olomouc, or the number of patients placed on the first biologic in the form of a biosimilar product Table 1 and the subsequent rates of treatment termination or switch to another biologic. Specifically: the overview Table 1 includes the original product with adalimumab (Humira) and its biosimilar Hyrimoz, as well as the original product with infliximab (Remicade) and its biosimilars Remsima and Inflectra.
- Fourthly, when comparing the preparations, it was not take into account possible differences in the effectiveness of a given biologic drug in a patient not yet treated with a biological for psoriasis, but already pre-treated, because it was assumed similar effectiveness - see, for example, in a recent comprehensive pharmacoeconomic analysis in the USA [6] it was also assumed only a relatively small 10 % reduction in efficacy in already pretreated patients.
- Fifth, data on the efficacy of certolizumab and infliximab after long-term use (48–52 weeks) were taken for the purposes of our CEA as equal to PASI 100 values achieved only after the induction period (including 95% CI), due to the unavailability of these data in wanted NMAs. Therefore, a greater degree of uncertainty of the cost- effectiveness result after long-term use can be assumed for preparations with these substances than for other preparations. However, this uncertainty of the result is partially compensated by the use of a 95% CI for the efficiency parameter (Figure 5), which is subsequently transferred to the CEA results Figure 7 and Figure 9.
- Sixth, the analysis of the cost-effectiveness calculation scenario was not performed for PASI 50 (for anti-TNFα and ustekinumab) or PASI 75 (for anti-IL 17 and anti-IL 23) values after 16 weeks of treatment (for etanercept after 12 weeks), as stated in the reimbursement conditions [13] in the Czech Republic as of September 18, 2021 [38].
Conclusion
The applied method of cost-effectiveness analysis (CEA) of biologic drugs in psoriasis in the context of modeled prices and bonuses at the health care provider confirmed our hypothesis that it can be used to fairly accurately quantify the effectiveness of the spent limited funds when using individual products, including the potential to determine the most cost-effective way of escalation treatment. I.e. with the intention to mediate the treatment of biological drugs to the greatest possible number of patients under the conditions of the same volume of funds, or with the intention to calculate the distribution of overall fixed costs for individual preparations as efficiently as possible while the number of patients treated in a given center does not change. These requirements become even more urgent in the context of the published long period of insufficient treatment of patients with psoriasis in the Czech Republic and the low quality of life of these patients before the introduction of biological treatment. A two-dimensional graph (costs vs. efficiency) with efficient frontiers has proven to be a very practical tool for visualization and quick evaluation of analysis results. In the current environment of the healthcare system in the Czech Republic, the practical application of the principles of how to spend the costs of using drugs in specialized care centers as effectively as possible is de-facto on the shoulders of this particular provider. We think that the presented CEA method used for a specific example of biological treatment of psoriasis can (with adequate adaptation) be applied in general for any chronic diseases with a clearly defined benefit (effect) parameter, with the current sufficient robustness of the data in terms of evidence. Furthermore, it is also a condition of the application of this CEA method when used in a given disease that the compared interventions of costly medicinal products have a not too different safety profile. When calculating treatment costs, it is also necessary to evaluate the impact of other costs associated with administration of the preparation, monitoring or treatment of side effects to the total price for the treatment. An important condition for the practical use of the CEA method in the provider’s environment is also the creation of a simple interactive evaluation model enabling immediate graphic visualization when changing any input variables, especially the prices per unit package of preparations or the amount of bonuses.
References
-
Tichý M (2011) Psoriasis-basic characteristic of a frequent disease. Dermatol Practice 5(4): 227-229.
-
Feldman SR (2023) Psoriasis: Epidemiology, clinical manifestations, and diagnosis.
-
National Health Information System (2018) Outpatient Care: Nzis Report No A brief overview of the activities of the field of dermatovenerology for the period 2007– 2017.
-
IDNES.cz (2021) Untreated psoriasis can put a person in a wheelchair, warns the primary minister.
-
(2019) SUKL’s decision on the Skyrizi product.
-
Institute for Clinical and Economic Review (2018) Targeted Immunomodulators for the Treatment of Moderate-to-Severe Plaque Psoriasis: Effectiveness and Value. Condition Update, Final Evidence Report, CEPAC.
-
Canadian Psoriasis Guidelines Addendum Committee (2016) 2016 Addendum to the Canadian Guidelines for the Management of Plaque Psoriasis 2009. Journal of Cutaneous Medicine and Surgery 20(5): 375-431.
-
Abdallah HB, Johansen C, Iversen L (2021) Key Signaling Pathways in Psoriasis: Recent Insights from Antipsoriatic Therapeutics. Psoriasis: Targets and Therapy 11: 83-97.
-
Fialová J, Kojanová M (2020) Complex treatment of psoriasis. Dermatol practice 14(2): 63-70.
-
Nast A, Smith C, Spuls PI, Bata-Csörgö Z, Boonen H, et al. (2020) EuroGuiDerm on the systemic treatment of Psoriasis vulgaris – Part 1: treatment and monitoring recommendations. JEADV 34(11): 2461-2498.
-
Wikipedia (2021) Psoriasis Area and Severity Index.
-
Amatore F, Villani AP, Tauber M, Viguier M, Guillot B, et al. (2019) French guidelines on the use of systemic treatments for moderate-to-severe psoriasis in adults. JEADV 33(3): 464-483.
-
Kojanová M, Fialová J, Gkalpakiotis S, Cetkovská P, Stork J, et al. (2021) BIOREP Biologic/Targeted Therapy Registry-2020 Summary Report. Czech-Slovak dermatology 96(1): 1-56.
-
(2021) Constitutional complaint: Reimbursement of modern drugs and drug centers.
-
Klimeš J, Mlčoch T, Pásztor B, Baloghová K, Veselá S, et al. (2020) Doporučené postupy pro zdravotně- ekonomická hodnocení v ČR: Česká společnost pro farmakoekonomiku a hodnocení zdravotnických technologií (ČFES). Květen, CFES, pp: 57.
-
Armstrong AW, Soliman AM, Betts KA, Wang Y, Gao Y, et al. (2021) Comparative Efficacy and Relative Ranking of Biologics and Oral Therapies for Moderate-to-Severe Plaque Psoriasis: A Network Meta-analysis. Dermatol Ther Heidelb 11(3): 885-905.
-
Sawyer LM, Malottki K, Sabry-Grant C, Yasmeen N, Wright E, et al. (2019) Assessing the relative efficacy of interleukin-17 and interleukin-23 targeted treatments for moderate-to-severe plaque psoriasis: A systematic review and network meta-analysis of PASI response. PLoS One 14(8): e0220868.
-
Lalkhen AG, McCluskey A (2008) Statistics V: Introduction to clinical trials and systematic reviews. Continuing Education in Anaesthesia Critical Care & Pain 8(4): 143-146.
-
University of Oxford (2021) pages left and right just this one cannot be found trust us, we did try.
-
Philips C, Thompson G (2009) What is cost – effectiveness? Hayward Medical Communications. 2nd(Edn.).
-
Bala MV, Zarkin GA (2002) Application of Cost- Effectiveness Analysis to Multiple Products: A Practical Guide. Am J Manag Care 8(3): 211-218.
-
Smith CH, Yiu ZZN, Bale T, Burden AD, Coates LC, et al. (2020) British Association of Dermatologists guidelines for biologic therapy for psoriasis 2020: a rapid update. British Journal of Dermatology 183(4): 628-637.
-
Warren RB, See K, Burge R, Zhang Y, Brnabic A, et al. (2020) Rapid Response of Biologic Treatments of Moderate-to-Severe Plaque Psoriasis: A Comprehensive Investigation Using Bayesian and Frequentist Network Meta-analyses. Dermatol Ther Heidelb 10(1): 73-86.
-
Tužil J, Práce S (2020) literary evidence. Iheta seminar in Prague on.
-
Chaimani A, Caldwell DM, Tianjing L, Higgins JPT, Salanti G, et al. (2021) Undertaking network meta-analyses. In: Higgins JPT, et al. (Eds.), Cochrane Handbook for Systematic Reviews of Interventions version. The Cochrane Collaboration.
-
Doležal T (2020) Data from real clinical practice of RWE. Iheta seminar in Prague on.
-
Torres T, Puig L (2015) Treatment goals for psoriasis: Should PASI 90 become the standard of care? Actas Dermo-Sifiliográficas 106(3): 155-157.
-
(2014) Lemtrada 12 mg (alemtuzumab). Analysis of cost effectiveness and impact on the budget in the conditions of the Czech Republic.
-
Institute for Clinical and Economic Review (2016) Targeted Immunomodulators for the Treatment of Moderate-to-Severe Plaque Psoriasis: Effectiveness and Value. Final Evidence Report, pp: 278.
-
Wikipedia (2021) Trigonometric function.
-
Kojanová M, Cetkovská P, Fialová J, Stork J, Gkalpakiotis S, et al. (2019) BIOREP Biologic/Targeted Therapy Registry - 2019 Summary Report. Czech word Derm 95(1): 1-40.
-
Kojanová M, Fialova J, Cetkovska P, Dolezal T, Lomicova I, et al. (2021) Demographic data, comorbidities, quality of life, and survival probability of biologic therapy associated with sex-specific differences in psoriasis in the Czech Republic. Dermatologic Therapy 34(2): e14849.
-
Kojanová M, Fialová J, Cetkovská P, Gkalpakiotis S, Jirčíková J, et al. (2016) Analysis of patients with moderate to severe psoriasis before starting biological treatment in the Czech Republic - data from the BIOREP registry 2005–2016. Czech word Derm 91(5): 205-252.
-
Egeberg A, Danø A, Pedersen MH, Sohrt A, Borg E, et al. (2021) Modelling the optimal sequence of biologic therapies in plaque psoriasis in Spain. Journal of Medical Economics 24(1): 1134-1142.
-
Lambert JLW, Segaert S, Ghislain PD, Hillary T, Nikkels A, et al. (2020) Practical recommendations for systemic treatment in psoriasis according to age, pregnancy, metabolic syndrome, mental health, psoriasis subtype and treatment history (BETA-PSO: Belgian Evidence- based Treatment Advice in Psoriasis; part 1). JEADV 34(8): 1654-1665.
-
Cohen AD, Vender R, Naldi L, Kalb RE, Torres T, et al. (2022) Biosimilars for the treatment of patients with psoriasis: A consensus statement from the Biosimilar Working Group of the International Psoriasis Council. JAAD Int 1(2): 224-230.
-
(2019) Czech Dermatovenerological Society ČLS JEP. Consensus of doctors of biological treatment centers in the field of dermatovenerology on the issue of biosimilars.
- Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review