Successful Treatment of Inverse Psoriasis and Psoriatic Arthritis with Deucravacitinib
The treatment of inverse psoriasis with systemic therapy has not been widely reported, this report revealed the use of deucravacitinib in this condition.
Abbreviations
BSA: Body Surface Area; DIP: Distal Interphalangeal; FDA: Food and Drug Administration.
Introduction
We present the case of a 58-year-old man with inverse psoriasis and psoriatic arthritis successfully treated with deucravacitinib. Our patient suffered from inverse psoriasis and psoriatic arthritis for years. The patient was previously managed with topical steroids. The introduction of deucravacitinib therapy led to significant clinical improvement in both cutaneous and arthritic symptoms within four weeks. His skin remains cleared with no side effects noticed at week 12.
Deucravacitinib may be an effective treatment option for patients with inverse psoriasis who do not respond adequately to topical medications.
Case Report
Our patient is a 58-year-old Chinese male with a five- year history of itchy plaques on the scalp, underarms, groin, and genitals. He also experienced pain in his fingers and knees for four years, which occasionally affected his ability to walk. He was treated with topical steroids, but the plaques persisted, and he experienced significant painful swelling over his knees and a few finger joints. He had a long history of anxiety but did not require medication for it.
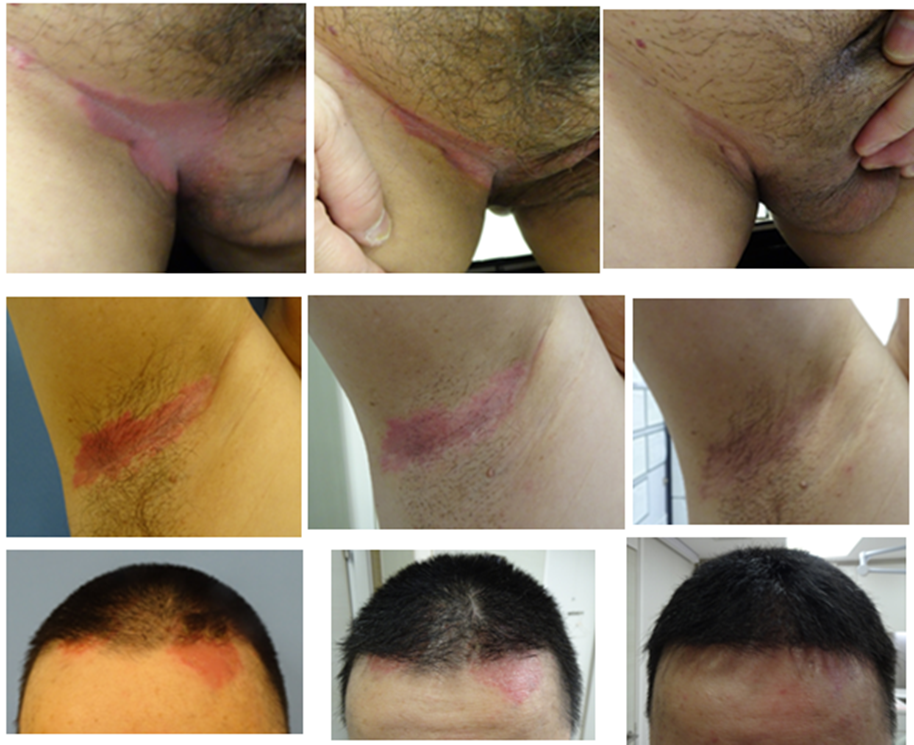
On examination, the patient had psoriasis plaques extending from his scalp to his forehead, as well as plaques on his underarms, groin, and penile shaft (Figure 1). His Body Surface Area (BSA) was 5%. He also had swelling in his knees and the distal interphalangeal (DIP) joint of his left middle finger and right little finger, with reduced range of motion in these joints. Given the severity of his symptoms and the failure of topical treatments, he was started on deucravacitinib 6mg daily after excluding tuberculosis and viral hepatitis infections. At a two-week follow-up, the plaques had become thinner with less erythema and scaliness, and his joint pain had significantly reduced, allowing him to walk without pain. By week four, his skin had cleared, with no plaques in the previously affected areas, and his joint pain had mostly subsided. He remained stable at subsequent follow-ups, with the last follow-up at week 12 showing clear skin and no significant joint pain. Blood tests, including a complete blood count and liver and renal function tests, remained normal.
Discussion
Inverse psoriasis is a subtype of psoriasis typically involving the genital and flexural areas rather than the extensor surfaces seen in the more common vulgaris subtype. Although patients with inverse psoriasis usually do not have extensive skin involvement, genital involvement can significantly impact their quality of life [1]. The absence or minimal presence of thick white scales on the plaques can make clinical diagnosis challenging [1], potentially delaying diagnosis and prolonging patient suffering. Treatment for inverse psoriasis can differ from other psoriasis subtypes, especially in the choice of topical agents, as the involvement of sensitive flexural and genital areas may limit the use of potent topical steroids. There is limited evidence of systemic therapies for treating inverse psoriasis [2]. Compared to those with psoriasis vulgaris, patients with inverse psoriasis may achieve PASI 90 or PASI 100 more slowly with biologics [3].
The patient in this case report had suffered from inverse psoriasis and psoriatic arthritis for years, causing significant psychological distress and affecting his self-esteem. Due to the severity of his arthropathy and joint pain, treatment with biologics approved by the US Food and Drug Administration (FDA) for psoriatic arthritis was initially suggested, but he was reluctant to take regular needle injections. Therefore, the standard dose of deucravacitinib was prescribed for better disease control.
Deucravacitinib is the first-in-class oral selective Tyrosine-protein kinase 2 (TYK2) inhibitor that inhibits the JAK/STAT pathway. TYK2 mediates cytokines involved in psoriasis pathogenesis, such as interleukin-23 and type
1 interferons [4]. Deucravacitinib was approved by the US FDA in 2022 for treating adults with moderate-to-severe psoriasis. Identical phase 3 randomized double-blind studies have shown deucravacitinib to be effective in treating plaque psoriasis, with a good safety profile. Patients treated with deucravacitinib demonstrated higher clinical effectiveness than those treated with placebo and apremilast at week 24 (PASI 75: 69.3% in POETYK PSO-1, 58.7% in POETYK PSO- 2) [4, 5]. The pooled data from two phase 3 trials revealed deucravacitinib is a safe and well tolerated treatment. No new safety signals were observed at week 52 [6]. Although deucravacitinib has not received its FDA approval on psoriatic arthritis yet, a phase 2 studies on the use of deucravacitinib for treating psoriatic arthritis showed significantly higher PASI 75 and ACR20 in patients treated with deucravacitinib [7]. The rapid response observed suggests that deucravacitinib is a potent therapeutic option for patients who have not responded adequately to topical treatments. However, its use in patients with inverse psoriasis had not been widely studied yet.
Conclusion
We report a case of a middle-aged man with inverse psoriasis and psoriatic arthritis, who demonstrated a rapid clinical therapeutic response to deucravacitinib. The treatment was well-tolerated, with no significant side effects observed at week 12. Deucravacitinib can be an effective treatment for inverse psoriasis and psoriatic arthritis, offering significant clinical improvements within a short duration. Further studies are needed to establish its long-term efficacy, particularly in the treatment of inverse psoriasis.
Funding
No funding received
Conflict of Interest
No conflict of interest to declare.
References
-
Micali G, Verzi AE, Giuffrida G, Panebianco E, Musumeci ML, et al. (2019) Inverse Psoriasis: From Diagnosis to Current Treatment Options. Clin CosmetInvestig Dermatol 12: 953-959.
-
Khosravi H, Siegel MP, Voorhees ASV, Merola JF (2017) Treatment of Inverse/Intertriginous Psoriasis: Updated Guidelines from the Medical Board of the National Psoriasis Foundation. J Drugs Dermatol 16(8): 760-766.
-
Mastorino L, Dapavo P, Macagno N, Ortoncelli M, Verrone A, et al. (2024) Clinical characteristics and response to biological therapies for inverse psoriasis: a real-life comparison between the therapeutic effects of anti- IL-23 and anti-IL-17 agents. Int J Dermatol.
-
Armstrong AW, Gooderham M, Warren RB, Papp KA, Strober B, et al. (2023) Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, placebo-controlled phase 3 POETYK PSO-1 trial. J Am Acad Dermatol 88(1): 29-39.
-
Strober B, Thaci D, Sofen H, Kircik L, Gordon KB, et al. (2023) Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, phase 3 program for evaluation of TYK2 inhibitor psoriasis second trial. J Am Acad Dermatol 88(1): 40-51.
-
Strober B, Blauvelt A, Warren RB, Papp KA, Armstrong AW, et al. (2024) Deucravacitinib in moderate-to-severe plaque psoriasis: Pooled safety and tolerability over 52 weeks from two phase 3 trials (POETYK PSO-1 and PSO- 2). J Eur Acad Dermatol Venereol 38(8): 1543-1554.
-
FitzGerald O, Gladman DD, Mease PJ, Ritchlin C, Smolen JS, et al. (2024) Phase 2 Trial of Deucravacitinib in Psoriatic Arthritis: Biomarkers Associated With Disease Activity, Pharmacodynamics, and Clinical Responses. Arthritis Rheumatol 76(9): 1397-1407.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling