Anxiety, Depression and Dermatology Life Quality Index Scores in Dermatology Outpatients
Background: The physical or perceived disfigurement can become a source of significant distress, with a considerable impact on an individual’s psychological, social, and physical well-being. Dermatological conditions are responsible for a significant source of social stigmatization in many human societies and cultures, contributing to the development of co-morbid diseases such as depression and anxiety. Objectives: To determine the levels of anxiety and depression in dermatology outpatients and to evaluate their association with quality of life and sociodemographic and clinical characteristics. Methods: A total of 150 patients attending our dermatology outpatient clinic in dermatology department, Benghazi Medical Center, and 100 healthy control subjects matched for age and sex were included in this study. All patients were asked to fill Dermatology Life Quality Index (DLQI) and Hospital Anxiety and Depression Scale (HAD), and healthy controls to fill only HAD. Results: The differences between the mean HAD anxiety (HAD-A) and HAD depression (HAD-D) scores of the patients and the controls were not significant statistically. 44% of all patients were at risk for anxiety while 35% of control subjects were at risk for anxiety, 38.7% of all patients were at risk for depression whereas only 29% of the controls were at risk for depression. Forty of the male patients and eighty-four of the female patients were at risk for anxiety and depression. Conclusion: Both marital status and severity of the disease have an influence on HAD-A and HAD-D scores. DLQI scores were not correlated with HAD-A and HAD-D scores.
Najat H Belkhair1, Ghada A Albarghathi2* and Gamal A Duweb3
¹Dermatology Department, Aljomhoryia Hospital, Libya ²Dermatology Department, Benghazi University, Libya ³Professor of Dermatology, Dermatology Department, Benghazi University, Libya *Corresponding author: Dr Ghada A Albarghathi, MD, Assistant professor of Dermatology, Dermatology Department, Faculty of Medicine, Benghazi University, Benghazi-Libya, Email: ghadataeib@yahoo.com
Abbreviations
Introduction
Psychodermatologic disorder is a condition that involves an interaction between the mind and the skin. Psychophysiologic disorders (e.g., psoriasis and eczema) are associated with skin problems that are not directly connected to the mind but that react to emotional states, such as stress. Most psychodermatologic disorders can be treated with anxiety-decreasing techniques or, in extreme cases, psychotropic medications [1].
Regardless of psychiatric morbidity, skin diseases can greatly affect patient’s quality of life (QOL). Thus, patient oriented QOL measures are particularly beneficial in chronic diseases as they assess how the diseases affect a person socially, psychologically and physically [2].
Only by understanding actual morbidity is it possible to achieve the free flow of relevant information for diagnosis and prescription, as well as subsequent adherence to therapy [3].
Several studies document an association between skin disease and anxiety. The anxiety level is reduced with improvement in skin condition and psychological treatment, and skin condition has been shown to improve with psychological treatment [4].
Objectives of the Study
To determine the levels of anxiety and depression in dermatology outpatients and to evaluate their association with quality of life and sociodemographic and clinical characteristics.
Patients and Methods
A total of 150 patients aged 18 years or older attending our dermatology outpatient clinic in dermatology department, Benghazi Medical Center, and 100 healthy control subjects matched for age and sex were included in this study, from March to September 2022. Information about age, sex, marital status, education was obtained in all subjects. Diagnosis and duration of the disease as well as the severity of the disease were noted in all patients according to proforma. The severity of the disease as minimal to severe was recorded by the scale of Dermatology Index of Disease Severity.
All patients were asked to fill Dermatology Life Quality Index (DLQI) [5] and Hospital Anxiety and Depression Scale (HAD) [6], and healthy controls to fill only HAD.
Results
A total of 150 dermatological outpatients (104 females and 46 males) and 100 healthy controls (61 females and 39 males) were enrolled in this study.
The mean ages of the patients and the controls were 35±12 and 36±10 years, respectively, the difference being not significant statistically.
Sex distribution was also not significant between the groups.
Sociodemographic and clinical characteristic of the patients are shown in Table 1.
| No. | % | |
|---|---|---|
| Sex | ||
| Female | 104 | 69.3% |
| Male | 46 | 30.7% |
| Education | ||
| 12 | 8% | |
| Primary School | 9 | 6% |
| Secondary School | 25 | 16.6% |
| Institute | 28 | 18.7% |
| University | 76 | 50.7% |
| Marital Status | ||
| Single | 73 | 48.7% |
| Married | 64 | 42.7% |
| Divorced | 6 | 4% |
| Widow | 7 | 4.7% |
| Stage of Disease | ||
| Mild | 58 | 39% |
| Moderate | 64 | 43% |
| Severe | 28 | 18% |
Table 1: Sociodemographic of the patients.
In 67 patients (44.7%) the duration of the disease was less than 1 year whereas in 29 patients (19.3%) the duration was more than 5 years. In most of the patients the disease was moderate in severity (42.7%). The mean HAD anxiety (HAD-A) and HAD depression (HAD-D) scores of the patients and the controls are given in (Table 2), the differences were not significant statistically.
| Patients | Control | T-Test | |
|---|---|---|---|
| Anxiety Subscale | 6.9±3.5 | 6.7±3.8 | P=0.816 |
| Depression Subscale | 6.5±3.8 | 6.3±3.2 | P=0.813 |
Table 2: The mean hospital anxiety and depression scale scores of the patients and the control.
| HAD-A Subscale | No. of patients (%) | No. of Controls (%) |
|---|---|---|
| Normal (0-7) | 84 (56%) | 65 (65%) |
| Mild (8-10) | 38 (25%) | 14 (14%) |
| Moderate (11-14) | 25 (17%) | 18 (18%) |
| Severe (15-21) | 3 (2%) | 3 (3%) |
Table 3: Distribution of patients and controls according to the HAD-A score.
Sixty-six of all patients (44%) were at risk for anxiety while 35 of control subjects (35%) were at risk for anxiety according to cut-off score of HAD-A subscale (Table 3), 58 of patients (38.7%) were at risk for depression whereas only 29 of the controls (29%) were at risk for depression according to cut-off score of HAD-D subscale (Table 4).
| HAD-A Subscale | No. of patients (%) | No. of Controls (%) |
|---|---|---|
| Normal (0-7) | 92 (61%) | 70 (70%) |
| Mild (8-10) | 37 (25%) | 18 (18%) |
| Moderate (11-14) | 17 (11%) | 11 (11%) |
| Severe (15-21) | 4 (3%) | 1 (1%) |
Table 4: Distribution of patients and controls according to the HAD-D score.
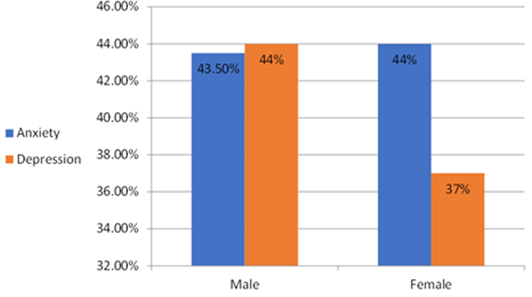
Forty of the male patients (87.5 %) and eighty-four of the female patients (81%) were at risk for psychiatric disorders (anxiety and depression) (Figure 1).
Most of the patients who are at risk for anxiety and depression belong to the age group 18-28 years, (39% and 33% respectively). More than half of the patients who are at risk for anxiety and depression are single (60% and 55% respectively). The duration of the disease was less than one year in most of the patients who are at risk for anxiety and depression (45% and 53% respectively). The mean HAD-A and HAD- D and DLQI scores of the patients according to diagnostic groups and the controls were shown in Tables 5 & 6.
| Diagnosis | No. | Anxiety Subscale | Depression Subscale |
|---|---|---|---|
| Acne Vulgaris | 15 | 7.1±4.1 | 6.4±4.5 |
| Tinea | 9 | 7.4 ±3.3 | 5.6±3.8 |
| Contact Dermatitis | 10 | 6.7±2.9 | 4.9±3.0 |
| Other Type Dermatitis | 9 | 6.5±4.4 | 6.1±4.1 |
| Psoriasis | 16 | 6.0±3.1 | 6.5±3.5 |
| Urticaria | 8 | 6.2±1.7 | 6.0±4.0 |
| Androgenetic Alopecia | 6 | 7.8±3.5 | 7.6±4.6 |
| Alopecia Areata | 9 | 6.1±3.8 | 5.6±3.5 |
| Vitiligo and Other Pigmentary Disorder | 20 | 6.8±3.1 | 7.8±4 |
| Warts | 6 | 6.0±2.0 | 6.1±2.7 |
| Hirsutism | 8 | 6.3±4.2 | 7.7±5.4 |
| Bacterial Skin Diseases | 9 | 10±3.7 | 6.6±3.3 |
| Other Diagnosis | 25 | 7±3.8 | 5.7±3.4 |
| Controls | 100 | 6.7±3.8 | 6.3±3.2 |
Table 5: The mean Hospital Anxiety and Depression Scale of the patients according to diagnostic groups and the controls.
| Diagnosis | No. | DLQI |
|---|---|---|
| Acne Vulgaris | 15 | 6.0±6.3 |
| Tinea | 9 | 4.4±5.3 |
| Contact Dermatitis | 10 | 1.3±5.9 |
| Other type Dermatitis | 9 | 8.7±5.2 |
| Psoriasis | 16 | 8.3±7.7 |
| Urticaria | 8 | 9.2±5.6 |
| Androgenetic Alopecia | 6 | 5.0±5.4 |
| Alopecia Areata | 9 | 8.7±6.8 |
| Vitiligo and Other Pigmentary Disorder | 20 | 6.3±5.2 |
| Warts | 6 | 3.1±2.4 |
| Hirsutism | 8 | 8.2±7.7 |
| Bacterial Skin Diseases | 9 | 7.3±5 |
| Other Diagnosis | 25 | 9.7±7.1 |
Table 6: The mean Dermatology Life Quality Index (DLQI) scores of the patients according to diagnostic groups.
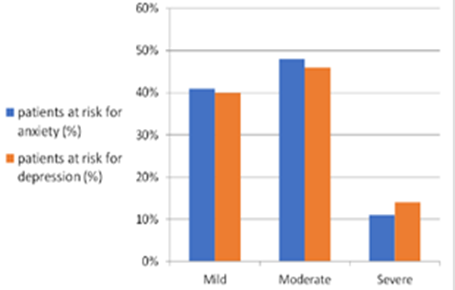
Multivariate analysis of variance showed that sex, age, educational level and duration of the disease did not have an influence on HAD-A and HAD-D scores, while both marital status and severity of the disease have an influence on HAD-A and HAD-D scores (p= 0.007 and p= 0.035 respectively) (Figure 2).
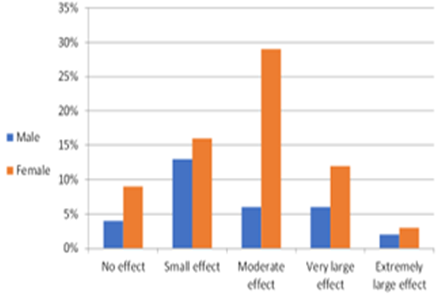
There were no statistically significant differences between the female and the male patients with respect to HAD-A and HAD-D scores (p= 0.642). The DLQI scores of the 150 patients ranged from 0 to 29, with a mean score of 7.67±6.33. Nine patients (6%) did not score on the DLQI (total score was zero), 53% of our patients have moderate to very large effect of the disease on their life, 5% have extremely large effect, while 29% have small effect and in 13% of patients no effect of the disease on their life. Majority of the male patients (13%) have small effect, but in female patients the majority (29%) have moderate effect of the disease on their life (Figure 3).
The disease has small effect on the life of 12% of patients in age group 18-28 years. The disease has moderate effect on the life of most of patients in age groups less than 50 years. In age group 29-39 years, no extremely large effect of the disease on the patient’s life. Most of the patients who have extremely large effect of the disease on their life were married (3%) while the disease has small effect on the life of 15% of single patients.
The disease has no effect on the life of 7% of patients with disease duration less than one year, whereas the effect of the disease was moderate in 10.6% of patients with disease duration more than 5 year.
In our study DLQI scores were not correlated with HAD-A (P= 0.509) and HAD-D (p=0.523) scores (Table 7).
| DLQI Score | HAD-A score (cut off point ≥ 8) | HAD-D score (cut off point ≥ 8) |
|---|---|---|
| No. of Patients (%) | No. of Patients (%) | |
| No Effect | 10(15%) | 7(13%) |
| Small Effect | 18(27%) | 18(31%) |
| Moderate Effect | 19(29%) | 17(29%) |
| Very Large Effect | 14(21%) | 10(17%) |
| Extremely Large Effect | 5(8%) | 6(10%) |
| Total | 66(100%) | 58(100%) |
Table 7: The relationship between the DLQI score and the HAD scores.
Discussion
Dermatological diseases have a negative effect on the daily life, self-confidence, and self-respect. In fact, they may lead to questions on self-image, thus creating a problem of identity. Dermatologists have observed their patients to be relatively more concerned and worried about the diseases that are related to their physical appearance, as a result of which dermatology patients may be affected by disorders such as anxiety, depression, and other psychosocial problems. In the present study there were no statistically significant differences between the mean HAD-A and HAD-D scores of the patients and the controls. Kiyment BAZ, et al. [7] found that the mean HAD-A and HAD-D scores of the patients were significantly higher than the controls, they also found that the age and sex distributions were not significant between the groups. In this study 44% of all patients were at risk for anxiety while 35% of control subjects were at risk for anxiety according to cut-off score of HAD-A subscale and 38.7% of patients were at risk for depression whereas only 29% of the controls were at risk for depression according to cut-off score of HAD-D subscale, these findings were much higher than what were reported by Kiyment BAZ, et al. [7].
Most of the patients who are at risk for anxiety and depression in the present study belong to the age group 18- 28 years, while Kumar A, et al. [8] found that the prevalence of depression was more in age group 26–45 years. The current study found that 87.5 % of the male patients and 81% of the female patients were at risk for psychiatric disorders (anxiety and depression), this was much higher than a previous study by Attah Johnson and Mostaghimi [9]. The results of the present study showed that sex, age, educational level and duration of the disease did not have an influence on HAD-A and HAD-D scores, while both marital status and severity of the disease have an influence on HAD-A and HAD-D scores. There were no statistically significant differences between the female and the male patients with respect to HAD-A and HAD-D scores.
Kiyment BAZ, et al. [7] found that sex, age, marital status, severity of the disease, educational level and duration of the disease did not have an influence on HAD-D scores, while HAD-A scores were influenced by the sex of the subject, with women having higher anxiety scores. Kumar A, et al. [8] found no significant difference in psychiatric morbidity between the gender groups. However, higher percentage was found among men. Earlier study, conducted by Johnson A, et al. [9] also found no significant difference among genders in total psychiatric morbidity. However, they found comorbid depressive disorder more in female as compared to male patients and comorbid anxiety disorder more in male as compared to female patients.
Jobanputra R, et al. [10] reported that women suffered significantly more in terms of self-esteem, clothing choice, as well as anxiety. Zachariae R, et al. [11] reported that a greater severity of disease, being female, having longer duration of disease, and younger age were associated with greater impairment of quality of life on DLQI. More than half of the patients in the present study who are at risk for anxiety and depression are single, while Picardi A, et al. [12] found a higher prevalence of psychiatric morbidity in women and in widows/ widowers. About half of the patients (53%) have moderate to very large effect of the diseases on their life. Majority of the male patients (13%) have small effect, but in female patients the majority (29%) have moderate effect of the disease on their life.
In the present study DLQI scores were not correlated with HAD-A and HAD-D scores, this was in contrast with a study of Kiyment BAZ, et al. [7] and Yanyu W, et al. [13] who found that DLQI scores were positively correlated with HAD-A and HAD-D scores. Sampogna F, et al. [14] also reported that in most skin conditions, psychiatric morbidity was strongly associated with poorer quality of life.
The DLQI measures a greater index of psychological disability than are measured by clinical severity of the skin disease. It has been reported that treatment adherence was strongly associated with complete satisfaction and strong negative association was observed between psychiatric morbidity and compliance, in a study examining factors associated with compliance with dermatological treatment [15].
Conclusion
Most of the patients who are at risk for anxiety and depression belong to the age group 18-28 years. The sex of the subject, age, educational level and duration of the disease did not have an influence on HAD-A and HAD-D scores, while both marital status and severity of the disease have an influence on HAD-A and HAD-D scores. There were no statistically significant differences between the female and the male patients with respect to HAD-A and HAD-D scores. The mean score of the DLQI was 7.67±6.33. DLQI scores were not correlated with HAD-A and HAD-D scores.
References
-
Koo J, Lebwohl A (2001) Psycho dermatology: the mind and skin connection. Am Fam Physician 64(11): 1873- 1878.
-
Finlay AY, Ryan TJ (1996) Disability and handicap in dermatology. Int J Dermatol 35(5): 305-311.
-
Holm EA, Wulf HC, Stegmann H, Jemec GBE (2006) Life Quality Assessment among Patients with Atopic Eczema. Br J Dermatol 154(4): 719-725.
-
Pasaoglu G, Bavbek S, Tugcu H, Abadoglu O, Misirligil Z (2006) Psychological status of patients with chronic urticaria. J Dermatol 33(11): 765-771.
-
Finlay AY, Khan GK (1994) Dermatology Life Quality Index (DLQI): A simple practical measure for routine clinical use. Clin Exp Dermatol 19(3): 210-216.
-
Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta Psychiatr Scand 67(6): 361-370.
-
Kiyment BAZ (2004) Increased levels of anxiety and depression correlated with dermatology life quality index scores in dermatology outpatients. T Klin J Dermatol 14: 31-37.
-
Kumar A, Kumar K, Swarup P, Tomar AS, Goel S (2016) A study to find depression in patients attending dermatological OPD in a teaching hospital. J Family Med Prim Care 5(2): 449-452.
-
Johnson FY, Mostaghimi H (1995) Co-morbidity between dermatologic diseases and psychiatric disorders in Papua New Guinea. Int J Dermatol 34(4): 244-248.
-
Jobanputra R, Bachmann M (2000) The effect of skin diseases on quality of life in patients from different social and ethnic groups in Cape Town, South Africa. Int J Dermatol 11: 826-831.
-
Zachariae R, Zachariae C, Ibsen H, Wulf HC (2000) Dermatology life quality index: data from Danish inpatients and outpatients. Acta Derm Venereol 80(4): 272-276.
-
Picardi A, Abeni D, Melchi CF, Puddu P, Pasquini P (2000) Psychiatric morbidity in dermatological outpatients: an issue to be recognized. Br J of Dermatology 143(5): 983- 991.
-
Yanyu W, Chaowei F, Wei Z, Caixia L, Jie Z (2018) The dermatology life quality index (DLQI) and the hospital anxiety and depression (HADS) in Chinese rosacea patients. Psychol Health Med 23(4): 369-374.
-
Sampogna F, Chren MM, Melchi CF, Pasquini P, Picardi A (2004) Association between poorer quality of life and psychiatric morbidity in patients with different dermatological conditions. Psychosom med 4: 620-624.
-
Renzi C, Picardi A, Abeni D, Agostini E, Baliva G, et al. (2002) Association of dissatisfaction with care and psychiatric morbidity with poor treatment compliance. Arch Dermatol 138(3): 337-342.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling