Prevention of Melasma in Pregnant Women: Aspects of Approach in Aesthetic Treatment
In the gestational period, several changes can occur in the woman's body, almost all the body's systems can undergo modifications, among them is the skin. One of the main changes that occur in the skin is melasma or pregnancy stain, which is the most common in the pigmentary changes of pregnancy. Hyperpigmentations are, in general, disorders distinguished by an increase in melanin and other pigments in the skin. The main triggers for the emergence of melasma are: sex hormones solar radiation and external agents, sources of free radicals. Melasma is characterized by irregularly shaped, brownish melanic pigmentation that appears mainly on the face, and may appear in the 1st or 2nd trimester of pregnancy, especially in women who are of childbearing age and also with phototypes IV and V. During pregnancy, the use of photoprotection correctly is essential for skin protection and to prevent the appearance of melasma, it is always recommended to use sunscreen daily, being applied 30 minutes before sun exposure and reapplying whenever necessary, avoiding the maximum sun exposure between the hours of 10 am to 4 pm. After pregnancy, there may be a large increase in hyperpigmentation, so some professionals indicate treatment after weaning, with some whitening substances such as glycolic acid, azelaic acid, and kojic acid, and can be associated with combined therapy, that is, in some cases, associate diamond pelling, which is a device with a sandpaper at the tip where it produces a sanding in the epidermis. , thus generating cell renewal. It is extremely important that pregnant women receive, at the beginning of pregnancy, all the information on prevention of melasma, and care with adequate photoprotection, thus avoiding psychological suffering and changes in their self-esteem.
Introduction
During the gestational period, major changes occur in the woman’s body, such as endocrine, immunological and vascular changes, making them more sensitive from a physiological point of view, and especially emotionally. These bodily and psychological changes must be accompanied through health education, promoting self-knowledge and self-care, making the pregnant woman aware of the changes that may occur during this period [1, 2, 3]. One of the dermatological changes is the appearance of melasma, which is usually called chloasma or pregnancy mask, is termed as epidermal or dermal pigment disorder, which manifests as hyperpigmented macules, melanocytes and melanosomes, solar elastosis and enlarged dermal blood vessels. The spots appear on the face, and can affect the neck and arms, they are usually small and dark brown, affecting the forehead, nose, cheekbones (lower cheeks), upper lip and chin. They are unsightly, resulting in emotional imbalance that impacts women’s quality of life [2, 4, 5].
It is a dermatological disorder that is difficult to treat, with a multifactorial etiology, mainly associated with family history and genetics linked to Afro ethnicity, which can worsen with exposure to sunlight and heat, the use of hormonal oral contraceptives and pregnancy. Melasma occurs due to an increase in melanin synthesis and activity of melanocytes and melanosomes, and an increase in the activity of tyrosinase, an enzyme involved in the process of melanogenesis, also occurs [5, 6, 7].
By presenting itself in an unsightly way, it causes emotional suffering accompanied by embarrassment, altering the future mother’s routine. Hyperpigmentations tend to disappear soon after the gestational period, however, they need preventive care so that the clinical picture does not worsen, since conventional procedures and products for the treatment of stains should be avoided, due to the risk associated with the mother-to-be binomial. baby [8, 9, 10].
So far, there are few studies in the literature that investigate the use of aesthetic techniques and application of specific products for the treatment of spots in pregnant women. The growing concern of women with the prevention of melasma and the growth in the use of aesthetic procedures, makes it necessary to debate the risk and a deeper knowledge about the safety of aesthetic procedures applied during pregnancy [11, 12, 13]. In view of the need to update the literature that discusses cosmetic ingredients that do not present risks for the treatment of melasma in the gestational period, this study aims to establish which of the possible cosmetic ingredients that can be used for the prevention of melasma (chloasma, mask or pregnancy), addressing treatment options that do not pose risks to the mother and fetus.
Methodological Aspects
This review was carried out in a bibliographic and exploratory character, was conducted by searching scientific articles indexed in the main electronic databases: Web of Science (Thomson Reuters), PubMed Central (NCBI); Science Direct (Scopus, Elsevier), Springer Link (Nature), Wiley Online Library (John Wiley & Sons), Taylor & Francis (Taylor & Francis Group), EBSCO (EBSCO Industries), Scielo (Scientific Electronic Library Online) and Lilacs ( Latin American and Caribbean Literature in Health Sciences), published in English, Portuguese or Spanish. In a complementary way, searches were carried out based on bibliographic references of studies that addressed the topic in a relevant way on the Google Scholar search platform (Google, USA).
The present study sought to investigate the literature on aesthetic approaches used to prevent melasma during pregnancy, exploring information about safe active principles. For that, the descriptors “cosmetic procedures in pregnancy” were used, initially in English, and in a complementary way in Spanish and Portuguese. For better updating, the word “melasma” was added to the search, which has the same spelling in the three languages.
References of selected works to other documents of potential interest were also searched. Once qualified for full- text review, articles were included in the qualitative review if they met the following inclusion criteria:
- They contained data on treatment of melasma during pregnancy;
- Published after 2019;
- With observational reports or experimental study. Articles were excluded if: a) they were reports, banners or congress abstracts; b) did not present relevant or conflicting data on the use of active ingredients in the treatment of melasma during pregnancy. There was no review of confidential health information and the study was not interventional. Therefore, ethics committee approval was not required.
Results and Discussion
The term “cosmetic procedures in pregnancy” has 1520 results in English on the GoogleScholar search platform, 145 results in Spanish and 219 results in Portuguese (excluding patents and citations). Most indexed articles use English
words to register the descriptors, and this reason is verified in the main researched databases, where there are few articles in Portuguese or Spanish, or even no scientific literature on this topic in these languages. For this reason, the research conducted within the indexed databases continued using the word “cosmetic procedures in pregnancy” as a descriptor, together with the word “melasma”, using the Boolean operator “AND”. Within the researched databases, it is possible to find a total of 969 scientific articles, however, most of the articles have a different year of publication, and it is not possible to restrict the period to less than 5 years, as many databases did not present publications. during this period (Figure 1). After reading the titles, abstracts and exclusion of repeated articles, it was possible to observe that 44 references met the requirements and use the terms reported above as a tool for studies regarding aesthetic approaches used to prevent melasma during pregnancy.
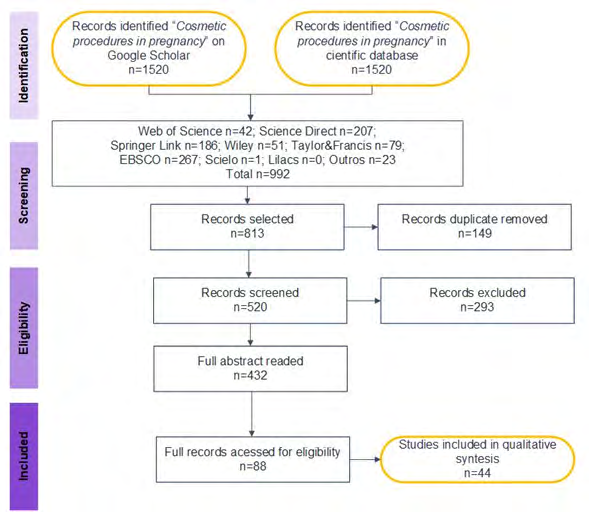
Source: The authors, 2022. Figure 1: Number of articles available in the literature that present the term “cosmetic procedures in pregnancy” associated with the descriptor “melasma”.
In this bibliographic review, several researches of some treatments for melasma during pregnancy were evaluated, which can be used certain depigmenting agents that do not cause risk to the mother and the fetus. It is generally more appropriate to adopt possible preventive care and avoid procedures and products with maximum effectiveness, but they can promote risks such as hypersensitivity, contact allergies, loss of pregnancy, malformations or functional changes, or even neuro-behavioral disorders, such as mental retardation, hydrocephalus, microphthalmia. between others. According to Jang YH, et al. [14], melasma is characterized as a symmetrical cutaneous hypermelanosis, due to an alteration in the pigmentary system of the skin. Excess melanin in the skin, can occur due to melanocytosis (which is the increase in melanocytes) or melogenesis (which is the excess production of melanin), they are called hyper-pigmented molecules, that is, melasma is evaluated. as a dermatosis that causes an increase in pigmentation in the skin [15]. It mainly affects women, especially with dark skin types V and VI. It is caused by genetic influences, exposure to sunlight, pregnancy, oral hormonal contraceptives, estrogen- progesterone hormone therapies, thyroid dysfunction, cosmetics and the use of some drugs, such as anticonvulsants (hydantoin) and antipsychotics (chlorpromazine), among others, which can influence the increase in the expression of the enzyme tyrosinase, involved in the synthesis of eumelanin [12, 16, 17].
In the human skin pigmentation process, tyrosinase is involved in the early stages of melanogenesis, and is an essential pigment for protecting the skin from damage caused by ultraviolet (UV) radiation. The increased expression of tyrosinase is implicated in the appearance of dermal and epidermal hyperpigmentation, such as melasma, freckles, ephelides and solar lentigines [6, 18]. Tyrosinase catalyzes the rate-limiting step for the melanin pigment biosynthetic pathway, being also responsible for the defense of the organism, and mutations that eliminate the activity of the tyrosinase gene result in albinism [19].
Tyrosinase is a binuclear copper-containing enzyme that catalyzes three steps in melanin biosynthesis:
- the hydroxylation of tyrosine to 3,4-dihydroxyphenylalanine (DOPA),
- the oxidation of DOPA to DOPAquinone, and
- the oxidation of 5,6- dihydroxyindole to indolequinone (Figure 1).
Due to its key role in melanogenesis, tyrosinase is an attractive target in the search for various types of depigmenting agents [6, 20, 21].
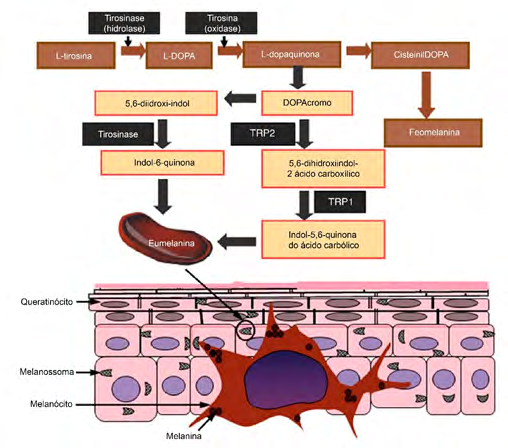
Source: adapted from Qian W, et al. [22]. Figure 2: Schematic representation of the action of tyrosinase on melanogenesis.
Melanin is mainly produced by melanocytes that are located in the epidermis, the outermost layer of the skin, and it is also this layer that determines skin color in humans. It is synthesized in melanosomes, which are intracellular corpuscles or melanin granules, acting as specialized organelles in melanocytes. Melanogenesis and chemical reactions within melanosomes, resulting in the production of two types of melanin: eumelanin and pheomelanin. Eumelanin is a dark-brown insoluble polymer, while pheomelanin is a light red-yellow soluble polymer that also contains sulfur. Both eumelanin and pheomelanin are formed by the conjugation of cysteine or glutathione [17, 23].
The pigment processhereeat itwthe with the oxidizesherethat of L-tyrosine to L-dopaquinone in the presence of the rate-limiting enzyme TYR. After the formation of L-dopaquinone, the resulting quinone undergoes intramolecular cyclization and oxidation, where it serves as a substrate for the synthesis of eumelanin and pheomelanin. During the process of melanogenesis, the hydroxylation of L-tyrosine to form L-3.4-dihydroxyphenylalanine (L-DOPA) It isthe rate limiting step of the entire process, whichIt iscatalyzed by tyrosinase [22].
The main cause of the appearance is still unknown, but there are some factors that contribute to the appearance of melasma, which are: solar radiation, sex hormones and external agents, sources of free radicals. In addition to these hormonal changes, genetics, racial characteristics, medications, cosmetics and endocrinopathies can also influence the onset of melasma [5, 10]. Placental formation can contribute by altering melanin synthesis, as it interferes with estrogen and progestin levels, which can act as a trigger for melatogenesis [14, 17]. Melasma affects mainly women of childbearing age and phototypes IV and V according to the Fitzpatrick classification (Table 1).
| Phototype | Skin Color | Feature |
|---|---|---|
| I | white, very light | Burns easily, never tans |
| II | white, clear | Burns easily but tans minimally |
| III | white, less light | Moderate burns, moderately tans |
| IV | light brunette to moderate | Burns little tans easily |
| V | dark brunette | Rarely burns and tans easily |
| SAW | black | never burns |
The classification of melasma depends on the melanin pattern according to histological characteristics and types of reaction to Wood’s lamp. This exam is used to define the four clinical types of melasma according to pigmentation [25]:
- Epidermal which has shades of light brown,pigmentation is intensified under Wood’s light examination. It is the most common type of melasma,histologically, it is characterized by an increase in melanin in the basal, suprabasal and stratum corneum layers;
- Dermal has more grayish or bluish-gray tones. There is no enhancement of pigmentation under Wood’s light. Histologically, there is a preponderance of melanophages in the superficial and deep dermis;
- Mixed type, pigmentation becomes more apparent in some areas, while in others there is no change;
- Indeterminate: invisible under Wood’s light.
Regarding the classification of lesions, there may be three clinical patterns of melasma. Central facial patterns that involve the cheeks, forehead, upper lip, nose, and chin. The malar pattern that involves the cheeks and nose, and the mandibular pattern that involves the ramus of the mandible [26]. On body the pigmentary changesare located on the inner sides of the thighs and armpits, areolas, nipples, linea alba of the abdomen and on the external genitalia [5, 27].
The pigmentary changes affects 70% of pregnant women, and may be physiological in this period, affecting women of Latin American ethnicity, where the prevalence can reach up to 90%. Melasma can disappear around a year after childbirth, however 30% of women remain with some sequel, which can contribute to the loss of self-esteem, or even develop postpartum depression [4, 10, 28, 29]. The causal agent of melasma is a decisive factor for it to be classified as transient or persistent, where the transient type disappears in less than one year, whereas the persistent type remains present for more than one year after the withdrawal of the hormonal stimulus, that is, in these cases after childbirth [15, 30].
As for the existing dermocosmetic ingredient options, so far, there are very few treatments that can be used during pregnancy, which are not harmful to the health of both the pregnant woman and the fetus. The FDA (Food and Drug Administration) classifies ingredients into six major groups, according to the risk assigned (Table 2) [12, 24, 31, 32].
| Action | Fda Class | Restriction Of Use | |
|---|---|---|---|
| hydroquinone | Used with corticosteroids and retinoic acids. It can prevent the formation of melanocytes or the increase in their degradation. | C | When up to 300 mg/kg is applied, it does not present toxicity in the formation of the fetus. |
| arbutin | It has depigmenting action and prevents tyrosinase (Tyr) from occurring. It shows excellent results in inhibiting hyperpigmentation and reducing melasma. | $\cdot$ | No toxicity is reported, causing no irritation or any hypersensitivity reaction. |
| Ascorbic acid | It is a depigmenting agent, which acts by preventing melanogenesis and preserving melanin in its discreet and achromatic form. | $\cdot$ | Restricted use due to difficulty in skin penetration and rapid oxidation. |
| kojic acid | It has whitening and anti-aging action and acts by preventing tyrosinase, through the chelation of ions and copper. | $\cdot$ | It can cause contact allergies and has a high potential for sensitivity, but teratogenic effects have not been proven. |
| azelaic acid | It is a dicarboxylic acid, isolated from Malassezia furfur yeasts, is vigorous in the treatment of melasma and post-inflammatory hyperpigmentation. It has an action to decrease tyrosinase inhibition. | B | Toxicological investigations regarding fertility, teratogenicity and embryotoxicity in animals did not show any risk of use in the gestational period. |
| retinoids | Prevents keratinocyte pigmentation granules and cell turnover growth, and aiding in the elimination of pigment. A peeling (peeling) occurs, through the reduction of keratinization. | C | They are not indicated because they have teratogenic results (Central Nervous System, heart, palate, ears, eyes) as studies do not show damage when used topically. |
| alpha hydroxy acids | It decreases the thickness of the stratum corneum, causes cell proliferation and collagen synthesis, resulting in an improvement in skin texture and hyperpigmentation. | B | AHAs with a pH less than or equal to 3.5 and a concentration less than or equal to 10% are safe for use during pregnancy. |
| Skin Whitening Complex | It has a whitening action and increases several levels of the chain in the formation of melanin, with benefits certified in studies. | A | It was clinically approved by dermatological professionals from Escola Paulista de Medicina. Because it does not cause skin irritation and can be applied to pregnant women and infants. |
Table 2: Risk factors attributed to the most used dermocosmetic ingredients in the treatment of melasma, according to the FDA.
FDA Risk Classification: A-Controlled studies observed no risk; B-Does not pose a risk to human fetuses, although there is a possible risk to animals;C- Risk cannot be eliminated, there are no studies performed in humans. But the benefit can outweigh the risks; D-Possess a possible risk to a human fetus, but the benefits may outweigh the risks; X- Contraindicated use in pregnancy.
Hydroquinone (HQ) is a hydroxyphenolic chemical, and inhibiting the conversion of dopa to melanin by inhibiting the enzyme tyrosinase.It also has as its mechanism of action the inhibition of DNA and RNA synthesis and reducing the degradation and distribution of melanocytes. HQ has been widely used in the treatment of hyperpigmentation and has shown great results, but it should be used with caution in patients who are in the gestational period [6, 28].
Arbutin, (grape extract) the beta-D-glucopyranoside derivative of hydroquinone, is a naturally occurring plant product that has a depigmenting action through tyrosinase inhibition, and has been very effective in decreasing existing melasma. The action of arbutin is dose-dependent and less toxic than hydroquinone. It is generally used at concentrations of 2 to 3%. Special care needs to be taken with higher doses as it can induce hyperpigmentation [26].
Ascorbic acid, also known as vitamin C, has antioxidant properties, which inhibit melanogenesis, reducing dopaquinone to DOPA and preventing the production of free radicals and the absorption of ultraviolet radiation. Ascorbic acid can promote great results in melasma therapy, as it has no side effects and can be used alone or in combination therapy [6, 27, 29].
Kojic acid is one of the depigmenting agents used to treat melasma in pregnant women,is a naturally occurring hydrophilic fungal product derived from certain species of Acetobacter, Aspergillus and Penicillium. It works by inhibiting the production of free tyrosinase; It is also a potent antioxidant.It is usually used at a concentration of 2%-4%, alone or in combination with tretinoin, hydroquinone or a corticosteroid [6, 17, 33, 34].
Azelaic acid is an acidsaturated, non-phenolic, naturally occurring nine-carbon dicarboxylic acid that inhibits tyrosinase, which promotes great results in the treatment of post-inflammatory hyperpigmentation and melasma.Its mechanisms of action are to prevent the synthesis of DNA and mitochondrial enzymes, thus inducing direct cytotoxic effects on the melanocyte.It has no toxic effects and can be used during pregnancy and lactation [17, 33].
Retinoic acid (RA)synthetic derivatives of vitamin A, the mechanism of action of topical retinoids is still unclear, but theRetinoids affect several steps in the melanization pathway. Tretinoin promotes rapid loss of pigment through epidermopoiesis and increases epidermal turnover and decreases the period of contact between keratinocytes and melanocytes. Retinoic acid suppresses UVB-induced pigmentation by reducing tyrosinase activity. The acid acts at a post-transcriptional level on tyrosinase and tyrosinase- related protein.Generating a desquamation (peeling), through the reduction of keratinization. Both systemically, isotretinoin and topically are contraindicated during pregnancy [7, 17, 34].
Alpha-hydroxy acids are a group of organic acids widely represented in fruits and vegetables (glycolic acid, lactic acid, tartaric acid, malic acid and citric acid) which when used on the skin promotes a reduction in the thickness of the stratum corneum, stimulating cell proliferation and collagen synthesis, thus providing an improvement in skin texture, and also in hyperpigmentation. AHAs with a pH lower than or equal to 3.5 and a concentration lower than or equal to 10% do not present risks during pregnancy [6, 17, 18, 20].
SkinWhiteningComplex® (SWC) has as components: grape extract, biofermented grapefruit extract from Aspergillus spp, and rice extract, promoting the whitening action, expanding at various levels of melanin formation, promoting great effectiveness, it does not promote side effects and and can be used in pregnant women [22, 35]. Soon after pregnancy, hyperpigmentation is common, and treatment with bleaching substances such as glycolic acid, azelaic acid and kojic acid is necessary. These ingredients can be associated with the diamond peeling thatIt is a type of mechanical exfoliation that acts by removing all the dead cells from the surface layer of the skin, promoting tissue regeneration and uniforming the pigmentation of the skin and also contributes to the reduction of acne and skin oiliness [16, 17, 28, 33].
The most indicated treatment for melasma during pregnancy includes the use of sunscreens, topical corticosteroids and topical depigmenting factors, which act by decreasing local inflammation and preventing the action of the tyrosinase enzyme, decreasing melanin deposition and decreasing the deposition of blood cells. of melanin. During pregnancy, the use of photoprotection correctly is essential for skin protection and to prevent the appearance of melasma, it is always recommended to use sunscreen daily, being applied 30 minutes before sun exposure and reapplying whenever necessary, avoiding as much as possible. of sun exposure between 10 am and 4 pm [2, 12, 13, 17, 36].
Currently, chemical sunscreens are classified by groups into anthranilates, salicylates, benzophenones and cinnamates, among others, which are molecules capable of absorbing UVA and UVB radiation. There are also physical photoprotectors, characterized as sunscreens. This is not absorbed by the skin, a protective layer is built that acts by reflecting and spreading ultraviolet (UV) radiation, and thus preventing its absorption, such as titanium dioxide and zinc oxide. In general, the safety and protection measure for skins, but sensitive in the gestation period [27, 37, 38].
Many of these women do not receive the proper information about the harmful effects that the sun can cause on the skin, certain daily care to protect the skin. In addition to melasma, sun rays can promote sunburn and phototoxicity, actinic changes or dermatoheliosis, which are characterized by the appearance of wrinkles and premature aging of the skin, irregular thinning of the epidermis, telangiectasia, hyperpigmented macules; It can also cause the appearance of efelides (freckles); solar urticaria; and polyform eruption, or even skin cancer [39, 40]. After treatment, melasma may return due to the hormonal trigger that is persistent for the development of the disease. For this reason, treatment of melasma during pregnancy is usually delayed until postpartum, and treatment may be unnecessary because melasma may disappear after pregnancy. In view of this, the pregnant woman should look for a trained professional who must provide the necessary information about the changes that occur in the gestational cycle, the preventions that she must take and specific, totally safe treatment that can be applied during pregnancy.
Final Considerations
For most pregnant women, melasma ends up becoming a very big concern, even though it is basically of a non-harmful nature that is not harmful to the health of the pregnant woman, but causes harmful effects on the quality of life, such as postpartum depression that affects the vast majority. This study considered several therapeutic resources for the treatment of melasma, verifying that aesthetic treatments can occur during pregnancy as a means of prevention. Some results show that there are not enough guidelines offered by health professionals to make pregnant women aware of the pigmentary changes in the skin and the care they should take during this period.
It is extremely important to raise awareness of pregnant women about the dangers of sun exposure without proper protection, it is essential to carry out actions aimed at health education in this gestational period, since these pigmentary changes in the skin occur, causing discomfort and socio- emotional conflicts. that can be prevented or minimized. Data collected in the researched articles show that 90% of pregnant women do not use sunscreen due to forgetfulness or lack of time. Women who did not receive information about all the pigmentary changes ended up developing melasma and showed psychological distress, changes in their self-esteem, even influencing future pregnancies.
It is concluded that the best way to avoid the emergence of melasma in this gestational period is prevention, it is the adequate information of daily care, thus avoiding the performance of procedures, as well as the discomfort and socio-emotional impacts. It is up to dermatologists, obstetricians and other health professionals to warn about the risks and preventions that must be taken. There is a great lack of data that can prove the safety of the procedures used during pregnancy, and with that comes a great difficulty for professionals to provide adequate treatments that are not harmful to the health of the mother and the fetus.
References
-
Bieber AK, Martires KJ, Stein JA, Grant KJM, Driscoll MS, et al. (2017) Pigmentation and Pregnancy. Obstetrics and Gynecology 129(1): 168-173.
-
Ogbechie GOA, Elbuluk N (2017) Melasma: an up-to-date comprehensive review. Dermatology and Therapy 7(3): 305-318.
-
Winton GB, Lewis CW (1982) Dermatoses of pregnancy. Journal of the American Academy of Dermatology 6(6): 977-998.
-
Fernandez FA, Barja JM, Vilas SA, Alija A (2018) Histopathological findings in pregnancy associated with cutaneous hyperpigmentation. Journal of Cutaneous Pathology 45(4): 286-289.
-
Hande AC, Miot LDB, Miot HA (2014) Melasma: A clinical and epidemiological review. Brazilian Annals of Dermatology 89(5): 771-782.
-
Perez BA, Munoz PMA, Camacho F (2000) Management of facial hyperpigmentation. American Journal of Clinical Dermatology 1(5): 261-268.
-
Shankar K, Godse K, Aurangabadkar S, Lahiri K, Mysore V, et al. (2014) Evidence-based treatment for melasma: expert opinion and a review. Dermatology and Therapy 4(2): 165-186.
-
Goldberg D, Maloney M (2013) Dermatologic surgery and cosmetic procedures during pregnancy and the postpartum period. Dermatologic Therapy 26(4): 321- 330.
-
Lee KC, Korgavkar K, Dufresne RG, Higgins HW (2013) Safety of cosmetic dermatologic procedures during pregnancy. Dermatologic Surgery 39(11): 1573-1586.
-
Purim KS, Avelar MF (2012) Photoprotection, melasma and quality of life in pregnant women. Brazilian Journal of Gynecology and Obstetrics 34(5): 228-234.
-
Brown AS, Hussain M, Goldberg DJ (2011) Treatment of Melasma with low fluence, large spot size, 1064- nm Q-switched neodymium-doped yttrium aluminum garnet (Nd:YAG) laser for the treatment of melasma in Fitzpatrick skin types IIIV. Journal of Cosmetic and Laser Therapy 13(6): 280-282.
-
Katsambas A, Antoniou C (1995) Melasma. Classification and treatment. Journal of the Eur. academy of Dermato. Venereol 4(3): 217-223.
-
Prignano F, Ortonne JP, Buggiani, G, Lotti T (2007) Therapeutical approaches in melasma. Dermatologic Clinics 25(3): 337-342.
-
Jang YH, Yes JH, Kang HY, Kim YC, Lee ES (2012) The histopathological characteristics of male melasma: Comparison with female melasma and lentigo. Journal of the American Academy of Dermatology 66(4): 642-649.
-
Seite S, Park SB (2013) Effectiveness of a broad-spectrum sunscreen in the prevention of melasma in Asian pregnant women. Journal of Cosmetics, Dermatological Sciences and Applications 3(3): 4-7.
-
Guerrero D (2012) Dermocosmetic management of hyperpigmentations. Annals of Dermatology and Venereology 139(S4): S166-S169.
-
Sehgal VN, Verma P, Srivastava G, Aggarwal AK, Verma S (2011) Melasma: Treatment strategy. Journal of Cosmetic and Laser Therapy 13(6): 265-279.
-
Ortiz RCV, Berna J, Tudela J, Varon R, Garcia CF (2016) Action of ellagic acid on the melanin biosynthesis pathway. Journal of Dermatological Science 82(2): 115- 122.
-
Nesterov A, Zhao J, Minter D, Hertel C, Ma W, et al. (2008) 1-(2,4-Dihydroxyphenyl)-3-(2,4-dimethoxy-3- methylphenyl)propane, a novel tyrosinase inhibitor with strong depigmenting effects. Chemical & Pharmaceutical Bulletin 56(9): 1292-1296.
-
Kim YM, Yun J, Lee CK, Lee H, Min KR, et al. (2002) Oxyresveratrol and hydroxystilbene compounds. Inhibitory effect on tyrosinase and mechanism of action. Journal of Biological Chemistry 277(18): 16340-16344.
-
Victor FC, Gelber J, Rao B (2004) Melasma: A Review. Journal of Cutaneous Medicine and Surgery: Incorporating Medical and Surgical Dermatology 8(2): 97-102.
-
Qian W, Liu W, Zhu D, Cao Y, Tang A (2020) Natural skin-whitening compounds for the treatment of melanogenesis (Review). Experimental and Therapeutic Medicine 20(1): 173-185.
-
Cardinali G, Kovacs D, Picardo M (2012) Mechanisms underlying post-inflammatory hyperpigmentation: lessons from solar lentigo. Annales de dermatologie et de venereology 139 (S4): S148-S152.
-
Pires CA, Pancote CG (2017) Prevention and treatment of melasma during pregnancy. Corpus Hippocraticum Magazine 1(1): 1-11.
-
Tamler C, Fonseca RMR, Pereira FBC, Barcaui CB (2009) Classification of melasma by dermoscopy: Comparative study with Wood’s lamp. Surgical and Cosmetic Dermatology 1(3): 115-119.
-
Bandyopadhyay D (2009) Topical treatment of melasma. Indian Journal of Dermatology 54(4): 303-309.
-
Ni Z, Mu Y, Gulati O (2002) Treatment of melasma with Pycnogenol®. Phytother Res 16(6): 567-571.
-
Bolanca I, Bolanca Z, Kuna K, Vukovic A, Tuckar N, et al. (2008) Chloasma- The mask of pregnancy. Collegium Anthropologicum 32(S2): 139-141.
-
Jutley GS, Rajaratnam R, Halpern J, Salim A, Emmett C (2014) Systematic review of randomized controlled trials on interventions for melasma: An abridged Cochrane review. Journal of the American Academy of Dermatology 70(2): 369-373.
-
Sanchez NP, Pathak MA, Sato S, Fitzpatrick TB, Sanchez JL, et al. (1981) Melasma: A clinical, light microscopic, ultrastructural, and immunofluorescence study. Journal of the American Academy of Dermatology 4(6): 698-710.
-
Ghafarzadeh M, Eatemadi A (2017) Clinical efficacy of liposome-encapsulated Aloe vera on melasma treatment during pregnancy. Journal of Cosmetic and Laser Therapy 19(3): 181-187.
-
Katsambas AD, Lotti TM, Desinioti C, Derme AM (2015) European Handbook of Dermatological Treatments. In: 3rd (Edn.), Springer Berlin Heidelberg, Germany.
-
Chilicka K, Rogowska AM, Szygula R, Dziendziora UI, Taradaj J (2020) A comparison of the effectiveness of azelaic and pyruvic acid peels in the treatment of female adult acne: a randomized controlled trial. Scientific Reports 10(1): 1-8.
-
Gupta AK, Gover MD, Nouri K, Taylor S (2006) The treatment of melasma: A review of clinical trials. Journal of the American Academy of Dermatology 55(6): 1048- 1065.
-
Haddad AL, Matos LF, Brunstein F, Ferreira LM, Silva A. et al. (2003) A clinical, prospective, randomized, double- blind trial comparing skin whitening complex with hydroquinone vs. placebo in the treatment of melasma. International Journal of Dermatology 42(2): 153-156.
-
Lee DH, Oh IY, Koo KT, Suk JM, Jung SW, et al. (2014) Reduction in facial hyperpigmentation after treatment with a combination of topical niacinamide and tranexamic acid: A randomized, double-blind, vehicle- controlled trial. Skin Research and Technology 20(2): 208-212.
-
Cestari TF, Oliveira FBD, Boza JC (2012) Considerations on photoprotection and skin disorders. Annals of Dermatology and Venereology 139(S4): S135-S143.
-
Jadotte YT, Schwartz RA (2010) Melasma: Insights and perspectives. Acta Dermatovenerologica Croatica 18(2): 124-129.
-
Krieger L, Berneburg M (2012) Pigmentary lesions in patients with increased DNA damage due to defective DNA repair. Annals of Dermatology and Venereology 139(S4): S130-S134.
-
Torok HM, Jones T, Rich P, Smith S, Tschen E (2005) A safe and effective 12-month treatment for melasma. Cutis 75: 57-62.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria