Description and Comparison of Methods for the Determination of Anti-Sars-Cov-2 Antibodies
Introduction: The SARS-COV-2 pandemic had an impact with more than 570 million cases and more than 6.8 million deaths as recorded by the United Nations by July 2022. Within the diagnostic context, a few immunological techniques for the detection of anti-SARS-CoV-2 IgG antibodies emerged, including Chemiluminescent Microparticle Immunoassay (CMIA) and Enzyme-Linked Immunosorbent Assay (ELISA). This study aimed to compare three detection techniques that have different methodological basis. The study was observational, cross-sectional and retrospective in design. Materials and Methods: Serum samples were processed by the following methodologies: CMIA and “in-house” ELISA. Results: The methodologies were quantitatively evaluated by the correlation method, and qualitatively by assessing individual and simultaneous sensitivity and specificity. Conclusion: These methodologies were designed in a health emergency context so they do not have a gold standard; thus, different algorithms are proposed to improve both the sensitivity and specificity of the detection of SARS-CoV-2 antibodies.
Introduction
Coronavirus disease-2019 (COVID-19) is an infectious disease, caused by the virus of the same name, which causes severe acute respiratory syndrome coronavirus 2 (SARS- CoV-2). It was first identified in December 2019 in Wuhan city, capital of Hubei province in China, when cases of a group of sick people with an unknown type of pneumonia were reported. The affected individuals were linked to workers at the Wuhan South China Wholesale Seafood Market. The
World Health Organization (WHO) recognized COVID-19 as a global pandemic on March 11, 2020 [1].
The United States Centers for Disease Control and Prevention, (U.S. CDC) and the WHO argues that the etiological diagnosis of COVID-19 requires identification of the responsible microorganism, SARS-CoV-2, in upper or lower respiratory tract samples using molecular biology techniques such as real-time reverse transcriptase polymerase chain reaction (RT-PCR) [2].
The SARS-CoV-2 genome is composed of approximately 30,000 nucleotides, which encodes four structural proteins, including spike (S), envelope (E), membrane (M) and nucleocapsid (NP) proteins, and also several accessory or non-structural proteins [3]. The protein S is a transmembrane protein with approximately 180 kDa molecular weight, which is found on the outside of the virus. The S-glycoprotein forms homotrimers on the virion surface and mediates receptor recognition and membrane fusion. During viral infection, a host cell’s furine-like protease cleaves protein S into the subunits S1 and S2. Whereas S1 contains the receptor- binding domain, which binds directly to the peptidase domain of angiotensin-converting enzyme 2 (ACE2), S2 is responsible for membrane fusion. When S1 binds to the host ACE2 receptor, another splitting site in S2 is exposed and cleaved by host proteases; such a process is critical for viral infection [4]. The NP protein is a structural component of SARS-CoV-2 whose primary function is to bind to the RNA virus, forming the nucleocapsid [5]. Interestingly, the location of NP in the endoplasmic reticulum (ER) and Golgi region suggests a role for it in the viral assembly and budding [6]. Since such protein is bound to RNA, it participates in processes related to the viral genome, viral replication cycle, and host cell response to viral infections [7]. Moreover, NP protein is strongly phosphorylated and is suggested to lead to structural changes that improve the affinity for viral RNA; it also serves as a strong immunogen that induces humoral and cellular immunity [8, 9, 10]. Another important part of the virus is the membrane or M-protein, which is a structural protein that plays an essential role in determining the shape of the virus envelope. The last component is the envelope or protein E, which is the smallest protein in the structure of SARS-CoV-2 that plays a role in the production and maturation of the virus.
Most patients with COVID-19 were observed to develop lymphopenia, thrombocytopenia, and pneumonia, presenting higher plasma levels of proinflammatory cytokines in severe cases [11]. This suggests that the host immune system is involved in pathogenesis [12]. Patients infected with SARS- CoV or MERS-CoV were previously reported to develop antibody responses, but they exhibited a defective expression of type I and type II interferons (IFN), which is indicative of an inappropriate protective immune response, with high production and expression of inflammatory cytokines (IL6, IL1), a more severe characteristic in some individuals [13]. Cytopathic viruses, including SARS-CoV-2, induce death and injury of virus-infected cells and tissues as part of the viral replication cycle. Viral infection and replication in airway epithelial cells could cause high levels of pyroptosis, a highly inflammatory form of programmed cell death that is commonly observed with cytopathic viruses. This may further trigger a subsequent inflammatory response. The levels of IL-1β, an important cytokine released during pyroptosis, increase during SARS-CoV-2 infection.
Through a variety of pattern recognition receptors (PRRs), the alveolar epithelial cells and macrophages can detect both pathogen-associated molecular patterns (PAMPs) released, such as viral RNA, and damage-associated molecular patterns (DAMPs), such as ATP, DNA, and oligomers. A wave of local inflammation occurs in the blood of affected patients, involving an increased secretion of the proinflammatory cytokines and chemokines IL-6, IFγ, and the monocyte chemoattractant protein MCP1. These cytokines are indicative of a polarized T helper 1 (TH1) cell response, which is parallel to the observations made for SARS-CoV and MERS-CoV. Secretion of such cytokines and chemokines attracts immune cells from the blood to the infected site, particularly monocytes and T cells, but not neutrophils. The pulmonary recruitment of immune cells from the blood and infiltration of lymphocytes into the respiratory tract may account for the lymphopenia and the increased neutrophil- lymphocyte ratio observed in about 80% of patients with SARS-CoV-2 infection [14].
Serologic tests arise as a need to know the immune response to infection and the disease in its different forms becoming a laboratory test of clinical and epidemiological value. Antibody tests require a thorough understanding of the proteins that form the viral envelope, specifically those proteins to which the immune system responds, triggering the production of antibodies that mark or neutralize the virus [9]. For instance, protein S is the only one present on the viral surface and is responsible for the virus’s entry into the host cell; thus, it constitutes the main antigen that induces the production of neutralizing antibodies [10]. The S1 subunit of protein S contains a receptor-binding domain (RBD), which is responsible for recognition and binding to the ACE2 receptor on the cell surface to which SARS-CoV-2 binds.
Regarding the specificity of serological tests, the more unique the protein used, the lower the likelihood of cross- reactivity with other coronaviruses. The most similar of such viruses is SARS-CoV, which caused the 2002 SARS outbreak, whereas four other coronaviruses cause the common cold and it is essential to ensure that there is no cross-reactivity among them. Since March 2020, several important research studies have been published describing the features of immune system responses to SARS-CoV-2 infection, of which the following concepts stand out:
- Patients with COVID-19 have an NP-specific antibody response [15].
- Sera from patients recovered from COVID-19 could inhibit SARS-CoV-2 entry into target cells, indicating the involvement of humoral immunity [16].
- Anti-S antibodies were detected in patients with COVID-19 as early as three days after symptoms onset [17].
- S-RBD-specific antibody production and virus neutralizing activity was observed in recovered patients [10].
The assessment of the immune response provides information on whether a person was infected with the virus, whether they have developed neutralizing antibodies and whether these could be effective in preventing reinfection [18]. Available data indicate that up to 94% of patients can respond by producing immunoglobulins by day 14 after the onset of symptoms.
Since the abrupt onset of COVID-19, the need for methodologies to evaluate the immune response against the new virus became evident worldwide. Thus, rapidly emerged different formats of serological tests for the detection of specific antibodies against SARS-CoV-2, different types of antibodies, various antigenic targets, and the use of different specimens. However, due to the emergency context, such tests were manufactured without following formal regulations established by international entities.
Serological tests detect specific antibodies to SARS- CoV-2 proteins, mainly S and NP proteins, which are the most immunogenic. Anti-S-RBD IgG could be useful to analyze the serum neutralizing capacity in patients with COVID-19, in line with the role of humoral immunity in blocking receptor binding during viral entry into host cells [19].
The Food and Drug Administration (FDA) has published a policy for monitoring these tests for rapid authorization based on in vitro studies performed by diagnostic companies [20]. Despite existing recommendations on how to perform serological studies, there is no global consensus. Whereas the Diseases Society of America identifies four possible scenarios where such tests might be useful [21], including:
- Patients with symptoms suggestive of SARS-CoV-2 with negative viral RNA detection.
- Selection of potential plasma donors.
- Evaluation of the immune response after vaccination.
- Epidemiological studies.
Objective
This study aims to compare three serological techniques for the detection of anti-SARS-CoV-2 IgG antibodies to determine whether there are differences among them and whether they are comparable.
Materials
One hundred processed samples were selected from volunteer plasma donors who attended the Public Health Laboratory of Tucumán, Argentina between June 2020 and March 2021. The study was analyzed and approved by the Committee of Research Ethics under the Research Directorate of the local health system known as SIPROSA (acronym of Sistema Provincial de Salud), through the Proceedings N° 2926-410-A-2022 and Dictum of the Committee of Research Ethics N° 12-2022.
Inclusion Criteria
Samples from patients with detectable PCR results, in this way we have the certainty of exposure to the virus.
Exclusion Criteria
Samples from patients from the following population groups:
- Patients under 18 years of age.
- Patients with previous transfusions.
- Patients with symptoms associated with COVID-19.
- Patients with tattoos or piercings performed within the last 6 months.
- Women who were pregnant.
- Insulin-dependent diabetic patients.
- COVID-19 hospitalized patients who received plasma as treatment (detectable PCR).
The chosen exclusion criteria are based on resolution for the selection of blood donors RM 797/13 -1507/15 of the Directorate of Blood and Blood Products. Ministry of Health Presidency of the Nation. In the case of women who have been pregnant at some point in their lives, they cannot be convalescent plasma donors, because if they have had children or have suffered an abortion, they can generate antibodies that could be harmful to the Covid19 patients who receive their plasma. The same situation can occur in the case of people who at some point in their lives have received blood.
These generated antibodies could cause a serious reaction to the recipient of the plasma. This is why research projects with convalescent plasma from Covid19 patients focus on men and non-pregnant women who have never received blood. This work does not include a control group because it aims to evaluate and correlate different methods for the determination of anti-SARS-CoV-2 antibodies.
Laboratory Methodology
The serum samples were processed through CMIA and “in-house” ELISA methodologies developed by the local Institute for Research in Applied Molecular and Cellular Medicine (IMMCA, Tucumán, Argentina) with the collaboration of the Immunology Laboratory of the Public Health Laboratory (Tucumán, Argentina). • The SARS-CoV-2 IgG assay is a two-step automated immunoassay for the detection of IgG against SARS- CoV-2 nucleocapsid protein (NP) in serum and plasma using CMIA technology on the ARCHITECT i System.
A directly proportional relationship exists between the amount of IgG SARS-CoV-2 NP antibodies in the sample and the relative units of light (URLs) detected by the optical system. Such a relationship is reflected in the Index (S/C) calculated, where S is the signal of the sample and C is the cut-off point. The interpretation of the results is as follows: Negative URL when the Index is less than 1.4, and Positive URL when the Index is greater than or equal to 1.4. The ABBOTT CoV-2 6R86 insert shows the evaluation of both analytical specificity and clinical performance. • The CovidTuc-ELISA is a heterogeneous, non-competitive, in-house enzyme assay based on the indirect detection of specific IgG against the S-RBD protein present in serum samples. This protein is obtained by cloning, expression in human HEK293T cells culture, and further purification from the supernatant of the cell cultures; then, the pure protein is immobilized in microplates suitable for the clinical assay.
The “in-house” ELISA assay was developed and validated with more than 758 samples at IMMCA Laboratory, following a modified protocol established by Stadlbauer D, et al. [22], and was subsequently transferred to the Immunology Laboratory of the local Public Health Laboratory (Tucumán, Argentina). The assay presents a high sensitivity (92.2%) and specificity (100%). Cutoff values were calculated using receiver operating characteristic curve (ROC). Titers were calculated as the dilution in which the optical density obtained was equal to the cutoff [22, 23, 24]. • The SARS-CoV-2 IgG II Quant assay is designed to detect IgG antibodies, including neutralizing antibodies against RBD of the S1 subunit of the SARS-CoV-2 S protein both in serum and plasma of individuals. This assay is a two-step automated immunoassay for the qualitative and quantitative detection of antibodies using CMIA technology. The resulting chemiluminescent reaction is measured in URLs and there is a directly proportional relationship between the number of IgG antibodies against the SARS-CoV-2 virus in the sample and the URLs detected by the optical system.
The results are expressed in arbitrary units (AU)/ mL and the cut-off is 50 AU/mL. The interpretation of the results is as follows: Negative for values less than 50.0 AU/ mL and Positive for values greater than or equal to 50.0 AU/ mL. The specific performance features of the equipment are available in the insert, including accuracy, accuracy in recovery, linearity, analytical specificity, interference, clinical performance, comparison with a neutralization test, and class specificity. REF 6S60-01 CoV-2 IgG II. A comparison of the three methods analyzed in the current study is presented in Table 1.
| Test | Trial | Antigen | Trademark | Analyzer | Result Interpretation | |
|---|---|---|---|---|---|---|
| A | CMIA | NP | SARS-CoV-2 IgG ABBOTT | ARCHITECT Plus i1000 SR | ≥ 1.4 URL = POSITIVE< 1.4 URL = NEGATIVE | |
| B | ELISA | RBD | IN HOUSE | ELISA IV DIAGNOSTIC M021 Reader | ≥ 200 = POSITIVE< 200 = NEGATIVE | |
| C | CMIA | Spike | SARS-CoV-2 IgG II Quant ABBOTT | ARCHITECT Plus i1000 SR | ≥ 50.0 AU/mL = POSITIVE< 50.0 AU/mL = NEGATIVE |
Table 1: Comparison of the methods analyzed.
Statistical Analyses
The comparisons were performed using analyzing correlation and concordance and the Chi Square test. The statistical analysis was complemented by applying the 2 x 2 contingency table.
Results
100 samples were analyzed through methods A and B and 96 through method C. The correlation between the methods analyzed is presented in Figure 1.
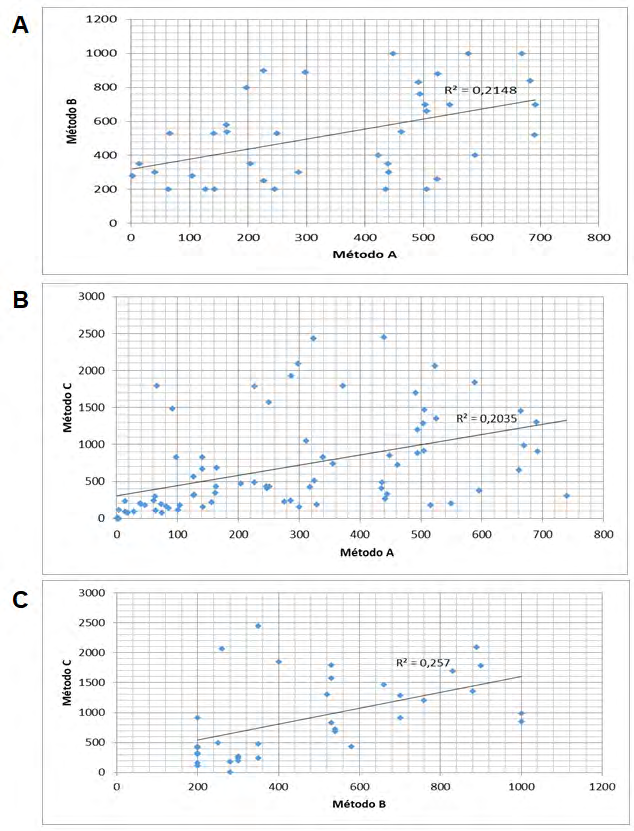
The correlation between pairs of methods was analyzed through a scatter chart. A) Correlation between method A and B. B) Correlation between method A and C. C) Correlation between method B and C. Positive and negative results for samples processed by each method are shown in Table 2.
| Method | Results | Total | |
|---|---|---|---|
| Positive | Negative | ||
| A | 70 (70%) | 30 (30%) | 100 |
| B | 58 (58%) | 42 (42%) | 100 |
| C | 92 (95.8%) | 4 (4.2%) | 96 |
Table 2: Distribution of results from analyzed samples.
To describe the performance of one method relative to another, the clinical epidemiology tool Table 2 x 2 was used. To date no gold standard-diagnostic method (laboratory, clinical and/or imaging) is available, we performed a comparison of the three available methods taking each one as a reference, alternately (Table 3).
| Method to Compare | Sensitivity | Specificity | PPV | NPV | |
|---|---|---|---|---|---|
| A | B | 70 | 70 | 8 | 50 |
| A | C | 100 | 14 | 74 | 100 |
| B | A | 84 | 50 | 70 | 70 |
| B | C | 98 | 8 | 62 | 75 |
| C | A | 74 | 100 | 100 | 14 |
| C | B | 62 | 75 | 98 | 8 |
Table 3: Sensitivity, Specificity and Positive and Negative Predictive Values of the three methods under study. References: PPV:
Table 3: Sensitivity, Specificity and Positive and Negative Predictive Values of the three methods under study. References: PPV: Positive Predictive Value; NPV: Negative Predictive Value; PV: Positive Value; NV: Negative Value; TPV: Total Positive Values; TNV: Total Negative Values. Sensitivity = PV/TPV of the method of reference. Specificity = NV / TNV of the method of reference. PPV = PV/(PV + PF). NPV = NV/(NV + NF).
Due to the differences in the dimension of the values of the cut-off points of the methods studied, the analysis of the qualitative results was performed using the interpretation as positive or negative. Both simultaneous sensitivity and simultaneous specificity are shown in Figure 2.
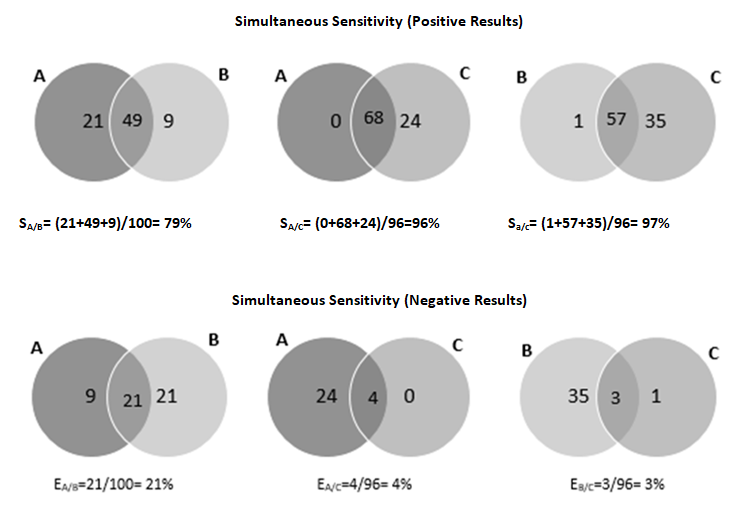
The simultaneous sensitivity shows the distribution of the positive results whereas the simultaneous specificity shows the distribution of negative results, both considering all the combinations of the methods in pairs.
Discussion
The dispersion of the methods analyzed was correlated with each other, with a value of R below 0.3, as observed in the scatter charts in Figure 1. In addition, significant differences were observed when comparing the quantitative results of the methods tested for anti-SARS-CoV-2 antibodies. As shown in Table 1, the methods analyzed show different development in terms of antigenic specificity, types of calibrators, expression of results and their different interpretations, which would explain the low correlation.
In this vein, it is important to highlight that the FDA established a control policy for these kinds of tests to obtain rapid authorization in the context of the epidemiological emergency. To date, there is no standardization or a global consensus for the measurement of these antibodies that would allow the interpretation of quantitative levels. After evaluating the qualitative results, we can highlight that method C has a higher percentage of positivity (95.8%), which was expected considering that all samples corresponded to patients with a diagnosis of COVID-19 by RT-PCR (Table 2).
From Table 3, we can observe that method C presents higher sensitivity when we take A and B as a reference, but not method B, which on the contrary shows the lowest value of sensitivity compared to A and C. The simultaneous sensitivity and specificity assessment (Figure 2) is useful in cases where the diagnostic test with the highest sensitivity and specificity (Gold Standard) is not available. It was observed that when samples are processed in parallel with methods A and C or B and C, the diagnostic sensitivity exceeds 95%, increasing the “efficiency” of antibody detection.
Conclusion
A serological diagnosis is an important tool in clinical and epidemiological evaluation. The methods studied were designed in a health emergency so they do not have a gold standard. To increase the diagnostic sensitivity, it is suggested that antibodies be detected simultaneously by two methods. Likewise, to improve the specificity of the result, we propose to process the samples sequentially with at least two of these methods. Considering that these are samples of patients diagnosed with COVID-19 by RT-PCR, with a high probability of presenting detectable titers of antibodies, we can argue that method C could be taken as a reference as it is the one with the best performance.
References
-
Lippi G, Gomar FS, Henry BM (2020) Coronavirus disease 2019 (COVID-19): the portrait of a perfect storm. Annals of Translational Medicine 8(7): 497.
-
Lippi G, Plebani M (2020) The critical role of laboratory medicine during coronavirus disease 2019 (COVID-19) and other viral outbreaks. Clinical Chemistry and Laboratory Medicine 58(7): 1063-1069.
-
Zhang YZ, Holmes EC (2020) A Genomic Perspective on the Origin and Emergence of SARS-CoV-2. Cell 181(2): 223-227.
-
Huang Y, Yang C, Xu XF, Xu W, Liu SW (2020) Structural and functional properties of SARS-CoV-2 spike protein: potential antivirus drug development for COVID-19. Acta Pharmacologica Sinica 41(9): 1141-1149.
-
de Haan CA, Rottier PJ (2005) Molecular interactions in the assembly of coronaviruses. Advances in Virus Research 64: 165-230.
-
Klumperman J, Locker JK, Meijer A, Horzinek MC, Geuze HJ, et al. (1994) Coronavirus M proteins accumulate in the Golgi complex beyond the site of virion budding. Journal of Virology 68(10): 6523-6534.
-
McBride R, van Zyl M, Fielding BC (2014) The coronavirus nucleocapsid is a multifunctional protein. Viruses 6(8): 2991-3018.
-
Burbelo PD, Riedo FX, Morishima C, Rawlings S, Smith D, et al. (2020) Sensitivity in Detection of Antibodies to Nucleocapsid and Spike Proteins of Severe Acute Respiratory Syndrome Coronavirus 2 in Patients With Coronavirus Disease 2019. The Journal of Infectious Diseases 222(2): 206-213.
-
Tan CW, Chia WN, Qin X, Liu P, Chen MI, et al. (2020) A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein- protein interaction. Nature Biotechnology 38(9): 1073- 1078.
-
Liu L, Wang P, Nair MS, Yu J, Rapp M, et al. (2020) Potent neutralizing antibodies against multiple epitopes on SARS-CoV-2 spike. Nature 584(7821): 450-456.
-
Chan JF, Yuan S, Kok KH, To KK, Chu H, et al. (2020) A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet 395(10223): 514-523.
-
Mahallawi WH, Khabour OF, Zhang Q, Makhdoum HM, Suliman BA (2018) MERS-CoV infection in humans is associated with a pro-inflammatory Th1 and Th17 cytokine profile. Cytokine 104: 8-13.
-
Cameron MJ, Bermejo Martin JF, Danesh A, Muller MP, Kelvin DJ (2008) Human immunopathogenesis of severe acute respiratory syndrome (SARS). Virus Research 133(1): 13-19.
-
Tay MZ, Poh CM, Rénia L, MacAry PA, Ng L (2020) The trinity of COVID-19: immunity, inflammation and intervention. Nature reviews. Immunology 20(6): 363- 374.
-
Burbelo PD, Riedo FX, Morishima C, Rawlings S, Smith D, et al. (2020) Detection of Nucleocapsid Antibody to SARS-CoV-2 is More Sensitive than Antibody to Spike Protein in COVID-19 Patients. MedRxiv.
-
Zhou P, Yang XL, Wang XG, Hu B, Zhang L, et al. (2020) A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579(7798): 270-273.
-
Ni L, Ye F, Cheng ML, Feng Y, Deng YQ, et al. (2020) Detection of SARS-CoV-2-Specific Humoral and Cellular Immunity in COVID-19 Convalescent Individuals. Immunity 52(6): 971-977.e3.
-
Petherick A (2020) Developing antibody tests for SARS- CoV-2. Lancet 395(10230): 1101-1102.
-
Zhou G, Zhao Q (2020) Perspectives on therapeutic neutralizing antibodies against the Novel Coronavirus SARS-CoV-2. Int J Biol Sci 16(10): 1718-1723.
-
FDA (2021) FAQs on Testing for SARS-CoV-2.
-
(2020) IDSA COVID-19 Antibody Testing Primer.
-
Stadlbauer D, Amanat F, Chromikova V, Jiang K, Strohmeier S, et al. (2020) SARS-CoV-2 Seroconversion in Humans: A Detailed Protocol for a Serological Assay, Antigen Production, and Test Setup. Current Protocols in Microbiology 57(1): e100.
-
Mostoslavsky G, Fabian AJ, Rooney S, Alt FW, Mulligan RC (2006) Complete correction of murine Artemis immunodeficiency by lentiviral vector-mediated gene transfer. Proceedings of the National Academy of Sciences of the United States of America 103(44): 16406-16411.
-
Tomas Grau RH, Ploper D, Ávila CL, Vera Pingitore E, Maldonado Galdeano C, et al. (2021) Elevated Humoral Immune Response to SARS-CoV-2 at High Altitudes Revealed by an Anti-RBD “In-House” ELISA. Frontiers in Medicine 8: 720988.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria