Persistence of Different Epidemic Pattern of Covid-19 in Western Pacific and In Europe
Covid-19 epidemic started towards the end of 2019. In the initial phase of the epidemic, the number of SARS-COV-2 patients per population was 100-fold higher in Europe than in Western Pacific. In Europe, the number of SARS-COV-2 patients per population remained continuously high, while, in Western Pacific, it increased from the lower level to higher level wave by wave. As of July 2022, the epidemic level of Western Pacific was still 10-fold lower than that of Europe. Probably the epidemic pattern different in Western Pacific and in Europe was still influenced by prevalence of α-1 anti-trypsin deficiency which is high in Europe but low in Western Pacific.
Introduction
Covid-19 epidemic emerged in China towards the end of 2019 and spread worldwide. The morbidity was high in Europe while it was low in Western Pacific. Epidemiological studies indicated positive correlation between the prevalence of Covid-19 and prevalence of α-1 anti-trypsin deficiency (AAT deficiency) [1, 2, 3, 4].
The present analysis was undertaken to examine whether the Covid-19 epidemic was still under the influence of AAT deficiency as of July 2022, because the number of the SARS-COV-2 infection became high even in Republic of Korea, Japan and other countries in Western Pacific, where AAT deficiency is rare.
As virus experiences mutation and selection during the transmission, variants more adapted to the receiving environment will prevail. In other words, when SARS-COV-2 virus spreads among population with low prevalence of AAT deficiency, such as, in Western Pacific [5, 6], it is expected that variants less sensitive to α-1 anti-trypsin may arise, while in Europe where AAT deficiency is frequent, epidemic will progress uninterruptedly.
Data Source
- WHO Coronavirus (Covid-19) Dashboard (https:// covid19.who.int/WHO-COVID-19-global-data.csv) for number of the SARS-COV-2 patients by country.
- Countries in the world by population (2022) https:// www.worldometers.info/world-population/population- by-country/ for the population size of the countries.
Relation between Number of the Patients and the Population Size
For the analysis, the epidemic period was split into two, before and after 25 April 2021, which is the midpoint of the epidemic from 3 January 2020 to 6 July 2022. The number of the patients per country was plotted in the vertical axis against the population size in the horizontal axis in Figure 1. The number of the patients was proportional to the population size both in Europe and in Western Pacific.
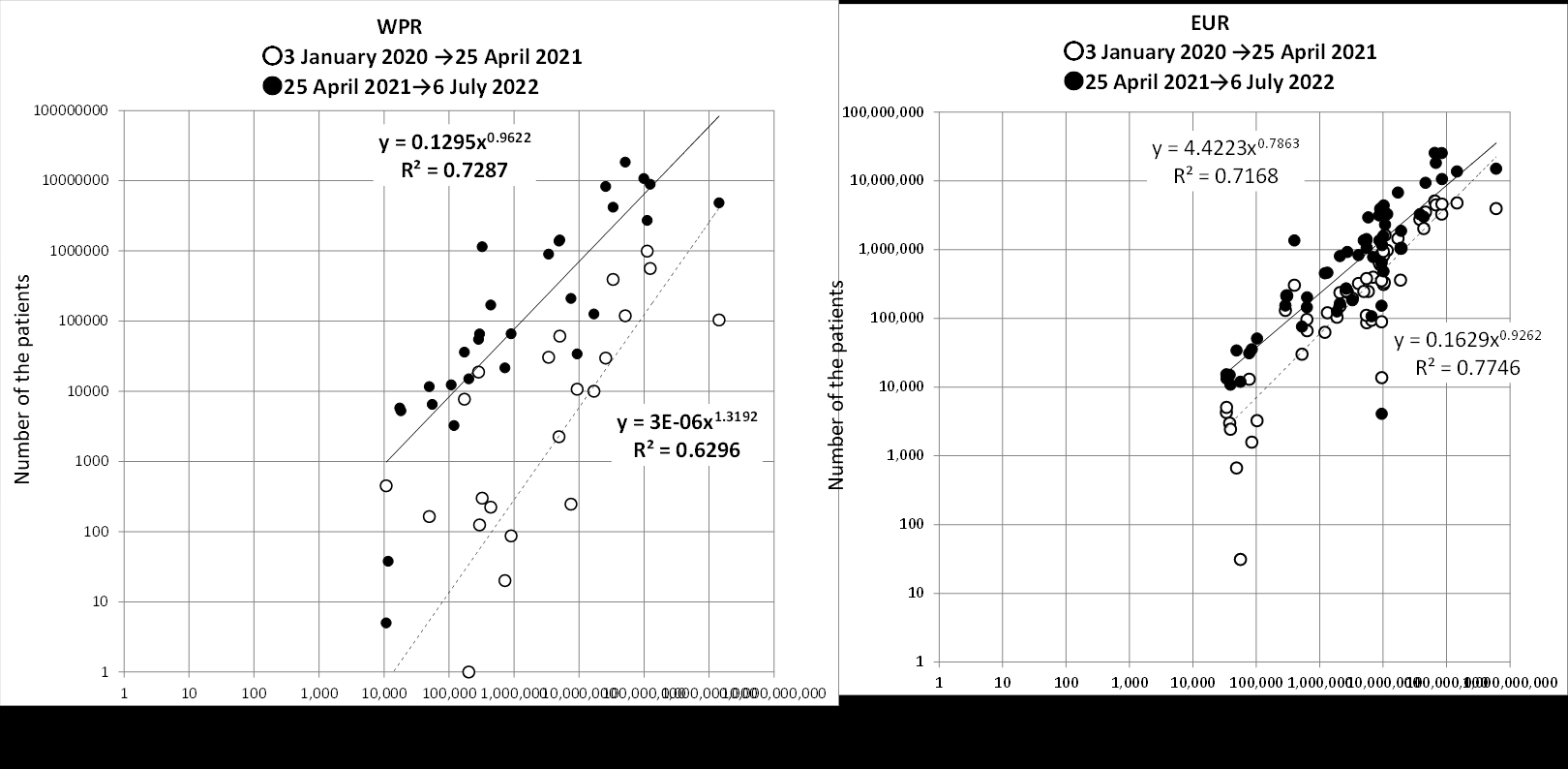
Figure 1: Relation between number of the patients and the population size. The number of the patients is plotted in vertical axis against population size in the horizontal axis both in the logarithmic scale. ○: from 3 January 2020 to 25 April 2021; ●: from 25 April to 2021 to 6 July 2022. Panel A: countries in Western Pacific; panel B: countries in Europe.
Before 25 April 2021 (Open Circles ○), the plot level was about 100-fold lower for Western Pacific (Panel A) than for Europe (Panel B). After 25 April 2021 (Closed Circles ●), however, the plot level became only 2-fold lower for Western Pacific (Panel A) than for Europe (Panel B). The observation suggested that, in Western Pacific where AAT deficiency was rare, SARS-COV-2 variants less sensitive to AAT was selected for during the epidemic, but, not in Europe because there was no such selective pressure.
Epidemic Curves with Respect to AAT Deficiency
As the number of the patients was proportional to the population size (Figure 1), daily number of the patients and that of the deaths per 1,000,000 population was plotted in the vertical axis along days starting from 3 January 2020 till 6 June 2022 (Figure 2).
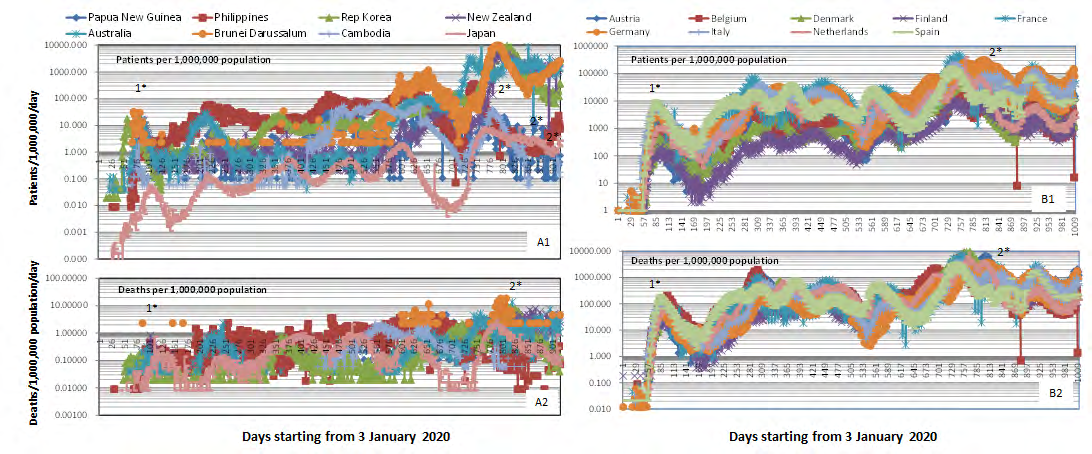
Figure 2: Daily number of the patients (panels A1 and B1) and that of the deaths (panels A2 and B2) per 1,000,000 population in logarithmic scale in the vertical axis along days after 3 January 2020. Panel A1 and A2: countries in Western Pacific; panel B1 and B2: countries in Europe. Peaks marked “*1” or “*2” were nearly synchronous between Western Pacific and Europe.
As for the patients (Upper Panels), it was found:
- For Western Pacific (Figure 2A1), in the first peak, 1*, the number of the patients per population was 30/1,000,000, while, for Europe (Figure 2B1), it was 10,000/1,000,000. The difference was about 300-fold.
- In Western Pacific, the number of the patients per population became larger wave by wave, from 30/1,000.000 population at peak 1* to 10,000/10,000 population at peak 2*. The increase was about 300-fold (Figure 2A1).
- In Europe (Figure 2B1), the number of the patients per population was much higher than in Western Pacific from the start of the epidemic; it was 10,000/1,000.000 at peak 1* and 60,000/1,000.000 at peak 2*: the increase was at most by 6-fold (Figure 2A2). It was as if SARS- COV-2 virus was “pre-adapted” to European population.
As for the deaths:
- In Western Pacific (Figure 2A2), the number of the deaths per 1,000,000 population was 0.01-10 throughout the period. As the number of the patients increased wave by wave, the case fatality decreased wave by wave, from 0.05 (1/20) at peak 1* To 0.002 (20/10,000) at peak 2*.
- In Europe (Figure 2B), the number of the deaths was 100-fold lower than that of the patients, and the plot of the deaths ran parallel with that of the patients. The case-fatality rate was 0.03 (300/10,000) at peak 1* and 0.02 (10,000/600,000) at peak 2*.
The above trend suggested that, in Western Pacific where AAT deficiency is rare, SARS-COV-2 virus became less sensitive to AAT through mutation and selection (Figure 2A1). In Europe where AAT deficiency is frequent, SARS- COV-2 spread uninterruptedly without requiring such adaptation (Figure 2B1).
Epidemic Curves with Respect to Synchronization
The Epidemic curves were synchronized almost perfectly among countries in Europe both for the patients (Figure 2B1) and for the deaths (Figure 2B2) and, to a lesser extent, among countries in Western Pacific (Figures. 2A1 and 2A2). Interestingly, peak 1*, peak 2* and some other peaks were synchronized in Western pacific and in Europe. It may have been brought about by evolution as quasi-species [7].
References
-
Vianello A, Braccioni F (2020) Geographical Overlap Between Alpha-1 Antitrypsin Deficiency and Covid-19 Infection in Italy: Casual or Causal? Arch Bronconeumol 56(9): 596-610.
-
Yoshikura H (2021) Epidemiological Correlation between Covid-19 Epidemic and Prevalence of α-1 Antitrypsin Deficiency in the World. Glob Health Med 3(2): 73-81.
-
Luisetti M, Seersholm N (2004) Alpha-Antitrypsin Deficiency. 1: Epidemiology of Alpha1-Antitrypsin Deficiency. Thorax 59(2): 164-169.
-
Yoshikura H (2021) Regionality of SARS-COV-2 Epidemic Under the Influence of Prevalence of α -1 Antitrypsin Deficiency: Similar Case-Fatality Rate in all The Regions but about 10-Fold Higher Number of Patients or Deaths per Population in American and European Regions. London Journal of Medical and Health Research 21(3): 1-6.
-
De Serres FJ (2002) Worldwide Racial and Ethnic Distribution of Alpha1-Antitrypsin Deficiency: Summary of an Analysis of Published Genetic Epidemiologic Surveys. Chest 122(5): 1818-1829.
-
Blanco I (2017) Blanco’s Overview of Alpha-1 Antitrypsin Deficiency-History, Biology, Pathophysiology, Related Diseases, Diagnosis And Treatment. Academic Press, United Kingdom, pp: 1-236.
-
Yoshikura H (2022) Synchronization of Covid-19 Epidemic among Different Prefectures and Different Age Groups in Japan. Epidemol Int J 6(S1): 000S1-019.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria