Incrusion of Bubonic Plague in the Rural Commune Andina
Introduction: Plague is a current scourge, despite the therapeutic evolution. In Africa, the DRC and Madagascar are the two countries that declare cases of plague: in 2018, 133 cases and 5 deaths in the DRC; 104 cases and 34 deaths in Madagascar. It is an infectious bacterial disease of wild rodents accidentally transmitted to humans by the infected fleas. It is a notifiable disease subject to international health regulations. Andina is one of the most active plagues in Madagascar. All people bitten by infected fleas can be sick without distribution according to social class. In view of these considerations, our objective aims to estimate the frequency of the plague, to describe its epidemiological, clinical and therapeutic aspects, and to evaluate the exposure of patients in the commune to the disease. Materials and Methods: On the one hand, we carried out a retrospective study in Andina by consulting the registered cases of the years 2013-2014. The diagnosis of plague was retained in 18 cases among the 31 cases recorded in the center. On the other hand, a survey on the housing of the patients was carried out. Results: The disease affected children under 15 (66.67% of cases). The female gender was predominant (61.11%). More than 51% of patients are febrile, including 69% with inguinal and axillary lymphadenopathy. More than 81% of clinical suspects were confirmed by the rapid diagnostic test and more than 44% of cases were treated with streptomycin, with 12% of cases dying during treatment. An additional survey was carried out to know the knowledge of the population which showed that 80% of people had heard of the plague and 60% recognized that deratting constitutes a means of preventive control of this disease. Conclusion: Plague management and surveillance have been improved following the possibility of rapid diagnosis in all CSB II, but the persistence of poverty plays a role in the maintenance of endemic outbreaks of this disease.
Introduction
The plague is an infectious disease that is still relevant today. It is considered a global, economic and social scourge with 21,725 declared cases and 1,612 recorded deaths, for a lethality rate of 7.4% [1, 2]. Plague is a zoonosis infecting mainly rodents but can be transmitted to humans accidentally either by the bite of an infected flea or when handling an infected host. It is one of the three quarantine epidemic diseases subject to the International Health Regulations and human cases must be notified to the WHO [3]. It is included in the list of re-emerging diseases because it is reappearing in countries where it was thought to have disappeared [4, 5]. Of the cases reported to WHO, 97% of cases are reported by African countries [2]. Indeed, over the past decade, 82% of all cases worldwide have been in the Democratic Republic of Congo (10,581 cases between 2000 and 2009) and Madagascar (7,182) [2, 6]. The plague is endemo-epidemiological in Madagascar, the endemic space consists of two foci, in the center and in the north of the island [7, 8]. As Madagascar is one of the countries that reports the highest number of human cases, about a hundred each year [9, 10], controlling this disease is a major public health issue. With the efforts of the Ministry of Health, all public health centers are able to treat all suspected or confirmed cases of plague free of charge. Generally, the victims of the plague are among the most deprived populations and in areas where political unrest persists [11]. In Madagascar, outbreaks of plague correspond to the most vulnerable rural area [4, 12]. The plague takes advantage of the ignorance and carelessness of the population to settle and take root in certain Fokontany or hamlets.
In view of these considerations, our objective aims to estimate the frequency of the plague, to describe its epidemiological, clinical and therapeutic aspects, and to evaluate the knowledge of the plague by the population in the Andina rural commune. Thus the first part of our study relates to literature reviews, followed by the second part relating to methodology and results. The discussion and the conclusion complete our work.
Reminders
Plague is a spontaneously fatal infectious bacterial disease caused by the Gram-negative bacterium Yersinia pestis [13]. It is a disease of wild rodents including rats, incidentally transmitted to humans by their fleas [14]. The general cycle of the plague involves three main actors: the bacillus, the rodent and the flea, man being only an accidental host. The natural reservoir of Yersinia pestis is the rat and its vectors are the fleas. In Madagascar, the reservoirs are the black rat Rattus rattus, and Rattus norvegicus, sewer rat, its vectors are fleas called Xynopsylla cheopsis for dwellings and Synosyllus fonquermiei for fields [15, 16]. Plague is typically transmitted either by fleas or by direct contact with infected animals, or by indirect contact by live vectors or by inert vectors. Transmission is very efficient but requires a relatively long incubation period (several weeks). Plague can manifest in two forms depending on the routes of entry of the bacillus and the severity of the symptoms developed. Cutaneous transmission by bite of infected fleas generally causes a bubonic plague which is marked by the appearance of hard and painful ganglia called bubo. Pneumonic plague, which is deadly and more severe, occurs either when infectious droplets are inhaled by coughing people or animals or by contact with virulent materials (called primary pneumonic plague), or when a case of bubonic plague is not treated in time (called secondary pneumonic plague). These two forms can progress to septicaemic plague which is accompanied by bacteraemia. Plague being a serious disease, the diagnosis is essentially clinical.
Confirmation of plague requires laboratory testing. Biological confirmation of the plague is done either by bacteriological examinations or by immunodiagnostic tests from samples (bubo pus, sputum, blood). Symptomatic treatment and antibiotic therapies must be implemented early without waiting for the results of bacteriology. In order to be able to control the plague, the cycle of the plague must be destroyed by permanent measures. Plague prophylaxis is based on the training of health personnel, anti-reservoir control and vector control, education of the population, the establishment of public health structures that are capable of rapid and laboratory diagnosis. For biological confirmation. The objective of surveillance is to detect and even predict the occurrence of cases of plague, and to limit the sources of human-to-human contagion, the occurrence of secondary pulmonary forms and to increase the cure rate. The best surveillance of human plague is based on the system of detection, confirmation, treatment and notification of cases. This is why it is important that health personnel are trained and recognize the symptoms that may suggest plague, and where sampling and analysis of the sample for diagnostic confirmation should be carried out.
Methodology
We carried out our study in 2016, at the Community Medical Center of Ambohimandroso located in the Andean Rural Commune. We chose to carry out our study in this town because it is one of the most active plague centers in Madagascar. This is a descriptive and cross-sectional retrospective study on the case of the plague that occurred in the town between 2013 and 2014. The study population consisted of patients registered in the register of the Community Medical Center in Ambohimandroso.
Inclusion Criteria
All patients registered in the plague register and who were treated as plague is included in our study.
Exclusion Criteria
All patients registered in the register but whose records are incomplete because clinical signs and/or treatments are not recorded. Sampling Mode This is an exhaustive sampling mode.
Variables Studied
The epidemiological data are age, gender, profession, address, month of appearance of the plague, vector, source, geographical locations. The clinical data are the mode of onset of the disease, the clinical manifestation, the clinical form. The paraclinical data are obtained by the use of the rapid diagnostic test on strip in the form of immunochromatic strip. This test is carried out by the public health staff of the Ambositra District with the staff of the center from the blood sample, or the liquid from the bubon, or sputum, or organs taken post-mortem. The collection of the test result and the preservation of the sample for the diagnostic confirmation examination are carried out on the same date as the collection. This confirmation examination is done at the Pasteur Institute of Madagascar located in Antananarivo.
Treatment
Treatment against the plague is implemented immediately after taking the samples for examination. The District Health Service is able to treat suspected patients free of charge. In general, the treatment instituted is antibiotic therapy.
Evolution
The evolution of the patients after the treatments was evaluated by taking the temperature and assessing the condition and size of the bubo.
Mode of Data Collection
We collected data from the registers of plague patients in the Service of the Community Medical Center of Ambohimandroso during the study period. We were able to interview all the patients coming from the Andina Rural Commune to have an overview of the exposure of patients to the disease. We collected information on their homes, on the number of people living under the same roof. Promiscuity is defined as many people living together in a small space. Thus houses with one or two rooms for 6 to 8 people have been classified as living in promiscuity. We took advantage of this trip to question the healthy population taken at random about the plague. For each individual an individual questionnaire was completed.
Statistical Analyzes
The data entered is analyzed using Epi info software version 7.1.5.0 (CDC, USA). The significance threshold used was p<0.05. Then we used the Excel 2013 software to make the graphs.
Limit of the Study
Our study is limited by the problem of representativeness and the lack of control of the variables because of its retrospective character, its unicentric character, the size of the sample.
Ethical Considerations
The anonymity of the patients was respected during the consultation of medical records. Privacy, human rights, patient confidentiality and professional secrecy were respected with honesty and caution. The doctor working in the department where the register was consulted was made aware of our study. His agreement was obtained before starting our research.
Results
Distribution According to Epidemiological Data
Frequency: From January 2013 to December 2014, there were 31 patients registered in the Medical Center among which 18 patients are infected with plague. This represents 58% of the patients registered during the study period. Among these 18 patients, 12 patients met our inclusion criteria, 13 patients were excluded.
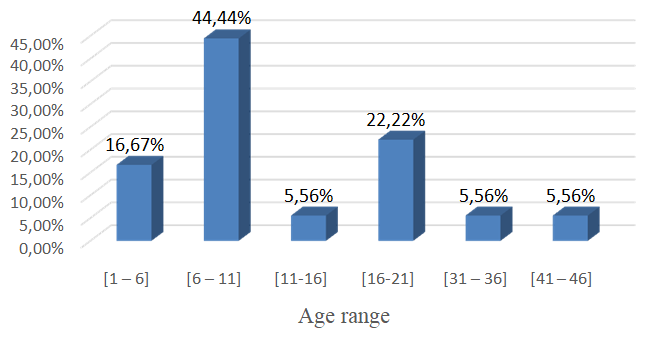
Distribution of Plague Cases by Age
The age of plague patients during the study period was within the age range of Figure 1 [6, 7, 8, 9, 10, 11].
Distribution of Plague Cases by Gender
Table 1 show that 61.11% of patients were female giving a sex ratio of 1.4.
| October | 15 | 83,33 | |
|---|---|---|---|
| Gender | Number (n=18) | Percentage (%) | |
| Female | 11 | 61,11 | |
| Male | 7 | 38,89 |
Table 2: Breakdown by gender of patients.
Distribution of Plaguecases by Profession
Figure 2 shows that more than 61% of patients are school-aged children.
16,67%
22,23%
61,11% Figure 2: Breakdown by occupation.
Distribution of Patients by Fokontany
Table 2 presents the case of suspected plague by fokontany. More than 80% of patients live in neighboring fokontany including Ampasina and Ambalamarina.
| Frequency (n=18) | Percentage (%) | |
|---|---|---|
| Ambalamarina | 8 | 44,44 |
| Ampasina | 7 | 38,89 |
| Anjamaivo | 1 | 5,56 |
| Ivato | 1 | 5,56 |
| Talaky | 1 | 5,56 |
Table 5: Table according to the frequency of patients by Fokontany.
Monthly Distribution of Plague Cases
Table 3 shows the resurgence of the plague in the hot and rainy season.
| Month | Number (n=18) | Percentage (%) |
|---|---|---|
| February | 1 | 5,56 |
| September | 2 | 11,11 |
| October | 15 | 83,33 |
Table 1: Monthly distribution of appearance of cases.
Distribution according to the Existence of Dead Rats
Table 4 reports that only 11.11% of patients reported the presence of dead rats spontaneously in their village a few days before the illness.
| Number of patients (n=18) | Percentage (%) | |
|---|---|---|
| Yes | 2 | 11,11 |
| No | 16 | 88,89 |
Table 3: Distribution according to dead rats.
Distribution of Patients according to Clinical Signs
The mode of onset and the clinical manifestations at the onset of the disease were not mentioned in the register.
Distribution of patients according to Clinical Manifestations
Table 5 shows that inflammatory lymphadenopathy (61.11%) is the most frequently observed clinical sign.
| Fokontany | Frequency (n=18) | Percentage (%) | |
|---|---|---|---|
| Ambalamarina | 8 | 44,44 | |
| Ampasina | 7 | 38,89 | |
| Anjamaivo | 1 | 5,56 | |
| Ivato | 1 | 5,56 | |
| Talaky | 1 | 5,56 |
Table 4: Distribution of patients according to clinical manifestations.
Distribution of Plague Cases according to the Treatment received by the Sick
Streptomycin was used to treat 83.33% of patients (Table 6).
| Number (n=18) | Percentage (%) | |
|---|---|---|
| Not mentioned | 3 | 16,67 |
| Streptomycin | 15 | 83,33 |
Table 6: Distribution of patients according to the treatments received.
Distribution of Patients according to Habitat
• Distribution according to the condition of the floor: All the floors of the houses of the sick are in beaten earth, 22% of which have holes rat (Table 7).
| Twice a month | 1 | 5,56 |
|---|---|---|
| Once every two month | 2 | 11,11 |
Table 8: Distribution according to the condition of the floor.
Distribution according to the Condition of the Roof
Table 8 shows that 61% of patients have thatch roofs with holes.
| Number of rooms | Number of houses | Number of people per house | Proportion (%) | |
|---|---|---|---|---|
| 1 | 1 | 6 | 5,56 | |
| 2 | 7 | 8 | 38,89 | |
| 3 | 2 | 3 | 11,11 | |
| More Than 4 | 8 | 7 | 44,44 |
Table 10: Distribution of patients according to the condition of the roof.
Breakdown by Environment Outside Homes Sick People
More than 38% of the houses of the sick are surrounded by bushes (Table 9).
| Effective (n=18) | Proportion (%) | |
|---|---|---|
| Well cleared | 11 | 61,11 |
| Surrounded by bushes | 7 | 38,89 |
Table 11: Distribution according to the environment near the habitat.
Breakdown by Frequency of Room Cleaning
More than 33% of patients clean their room twice a week (Table 10).
| Cleaning frequency bedrooms | Number (n=18) | Proportion (%) |
|---|---|---|
| Once a day | 3 | 16,67 |
| Once a week | 4 | 22,22 |
| Twice a week | 6 | 33,33 |
| Once a month | 2 | 11,11 |
| Twice a month | 1 | 5,56 |
| Once every two month | 2 | 11,11 |
Table 7: Distribution of patients according to the frequency of room cleaning.
Distribution according to the Number of People Living in the Same House
More than 44.45% of patients live in promiscuity (Table 11).
| Number of rooms | Number of houses | Number of people per house | Proportion (%) |
|---|---|---|---|
| 1 | 1 | 6 | 5,56 |
| 2 | 7 | 8 | 38,89 |
| 3 | 2 | 3 | 11,11 |
| More Than 4 | 8 | 7 | 44,44 |
Table 9: Distribution according to overcrowded lifestyle.
Comments and Discussion
Plague is real in Madagascar; the district of Ambositra is one of the most active centers of plague [17], with many cases occurring almost every year. It is a district located administratively in the region of Amoron’i Mania, it is included in the plague triangle of central Madagascar. The parameters used as the basis for analysis in our comments are:
- socio-demographic factors: age, gender, profession, address of patients.
- Epidemiological factors: the monthly evolution of plague cases, the existence of dead rats in the environment precedes the appearance of the disease.
- The clinical forms.
- Disease management.
- The environmental factors of the patients in the Rural Communes of Andina: type of habitat, salubrity, way of life.
- The most affected age group is from 6 to 11 years old, accounting for 44.44% of plague cases.
- This observation is compatible with other studies made in Madagascar which reported that plague is more frequent in children and adolescents [12, 18].
- A study in Zambia reported that 95% of plague patients were under 15 years old [19].
This frequency can be justified by the fact that this age group is confronted with contributing factors, such as promiscuity in schools, increased exposure to fleas (because they like to play in the mud), ignorance of what to do in the event of the spontaneous death of rodents in the village, and that their immune system is even weaker to defend itself against the plague bacteria.
One possible explanation for the younger age distribution of this disease was the practice of children sleeping on mats on the floor, which could have brought children closer to fleas. In fact, in rural areas, for lack of resources, only adults generally slept on beds raised above the ground.
We recommend expanding Information-Education- Communication (IEC), carried out by the health authorities to educate the population (especially children and adolescents) for the fight against the plague, with particular emphasis on modes of transmission and preventive measures.
Gender
In our study, there is a slight difference between the two genders with a male predominance (51.72% of cases), with a sex ratio of 1.4 (Table 1). In the district of Ikongo, a study on the resurgence of the plague shows a male predominance, i.e. 66% of cases [18]. Several other studies carried out in Madagascar have shown that males are more frequently affected than females [17, 20]. In Zambia, plague affects men more frequently than women (52% of cases were men) [19]. A study done in another country showed a higher frequency in men than in women in Manchuria, but a higher frequency in women than in men in India [12]. According to these reviews of the literature, our results of studies are consistent with other studies made in Madagascar and in other countries.
Occupation
In our study, the plague strikes all professional categories with a slight predominance among students According to the WHO, plague is a rural disease mainly linked to agricultural activities in Madagascar [2]. A study in Majunga showed that the hypothesis that the plague is linked to agricultural activity is unlikely because the majority of these patients were non-agricultural [12]. Our study supports this observation made in Majunga because among the 58 cases studied more than 27% of cases are farmers. We suggest intensifying communications for behavior change (CCC) so that the population is aware that the plague can be linked to their professional activities which are not necessarily linked to agriculture.
Address
In our study, than 80% of patients live in neighbouring fokontany including Ampasina and Ambalamarina. It is thought that the patients in the communes who were sick with the plague did not all come to the medical center for consultation. This may be due, on the one hand to the very far distance from the medical center and that patients can die on the road and their family takes them home without reporting them to the health authorities, and on the other hand to the use of traditional medicine before going to hospital.
We recommend setting up other medical centers in all municipalities so that diagnosis and treatment are closer to the residence of patients to avoid delays in treatment and to facilitate the monitoring of plague epidemics.
Epidemiological Factors
o The monthly evolution of plague cases It appears from our study that the plague occurs in the rural Andina commune with a seasonal incidence during the hot and rainy season. Indeed, 83,33% of Plague cases occur in October . Plague is an endemic disease in Madagascar, with seasonal epidemic peaks from October to April in the Central Highlands [12, 17]. In Tanzania, a study showed that the case of plague usually appears twice a year, going from May to June then in October and November [21]. A study carried out at Lushuto Hospital in Tanzania showed a tendency seasonal in which the highest number of plague cases occurs in the month of January [22]. Our results are in correlation with those of the literature with regard to the season plague.
The explanation for this epidemic seasonal peak may be linked to the fact that the maximum rainfall is between the months of November and April (the average start date of rains is mid- October, the average end date is mid-April). The humidity during this period favours the proliferation of rats and the pullulation of fleas. The ambient temperature at this time is also favourable for hatching epidemic.
In Madagascar, this seasonal peak can also be caused by the increase in burning practices of bushes which coincide with this period because the fires drive out the field rats that will move towards the villages and contaminate humans through their fleas. Farmers practice wild fires every year at the end of the dry period, so that the young grasses watered by the rain serve as food for the zebus.
The Notion of the Existence of Spontaneously Found Dead Rats
In our study, among the 18 cases, only 11,11 % of patients observed rodents died spontaneously 15 days before the epidemic (Table 4). During the epidemic in Mahajanga, 56.9% of the cases studied declared having seen dead rats around their homes. According to the literature, an epidemic of human plague can begin with an epizootic in peri-domestic rats from which infected rodent fleas can accidentally infect humans through their bites [23].
Indeed, murine mortality is a major indicator and provider of the disease. Plague but the meaning of the existence of dead rats without apparent causes is still unknown to most of the population. According to the Medical personnal of Andina there were no captured rats or fleas captured during the epidemic of 2013 and 2014. We recommend strengthening information-education- communication measures to raise awareness about the importance of disease outbreak notification.
Clinical Manifestations
It appears in our study that out of 18 patients more than 88,89% of the patients are febrile, 61,11% presented with inflammatory inguinal and axillary lymphadenopathy, and that 88,89% had presented with headaches (Table 5). In an African study that was done in Algeria reported that 88% of patients had inguinal lymphadenopathy [24]. In Madagascar, during the study carried out in Majunga, lymphadenopathy at the inguinal level is the most common [25]. Another study in Madagascar reported that 98% of cases had a bubo [12]. In Zambia, the most common sign was swollen cervical lymph nodes (90% of cases) [19]. Our study agrees with other studies made in Madagascar. Supported In our study, among the 18 cases studied, more than 83% of the cases are treated by the Streptomycin (Table 6) with a daily dose adapted according to the weight of the patients for 5 to 10 days.
Patient Environmental Factors
To be able to quantify the importance of the risk factors of the patients to the exposure to the disease we need to know their way of life and their dwelling. We were able to visit the home of the sick in the Rural Commune of Andina which declared cases of plague.
- Frequencies of cases of patients in Andina by Fokontany.
- By collecting information in this Commune, more than 80% of patients live in the neighbouring fokontany including Ampasina and Ambalamarina (Table 2).
- The state of the house and the way of life of the sick.
Housing and environmental sanitation can influence the occurrence of plague. Our study shows that 44% of patients in Andina live in promiscuity (Table 11). In our study, promiscuity is defined by the fact that many people live together in a small space. The eight houses for the sick, which have one or two rooms for 6 to 8 people living under the same roof, have been classified as living in promiscuity. All patients have mats on the floor; the frequency of cleaning the floor under the mat was asked. Our study showed that only 33% of patients cleaned their room twice a week (Table 10).
We believe that this frequency of cleaning is insufficient because this habit promotes the proliferation of fleas. Moreover, even if all the fields of their cultivation are further away from their home, there are also those who keep their livestock on the ground floor of their house. Patients claim that they rarely clean their floors even though they are aware that there are sometimes fleas in their house, especially during the hot and rainy season. All the houses of the patients in Andina are built of rammed earth, of which 88% of the patients have a thatched roof, of which 61% are in poor condition (Table 8). In our study, 22% of houses have dirt floors with rat holes (Table 7) and 38% of the houses have bushes nearby (Table 9).
Among the patients, there are those who burn their garbage but there are those who do not have well- defined methods to manage their waste. A study in Madagascar reported that poverty associated with overcrowded housing is a factor favoring the transmission of the plague [4]. A study done in Africa, specifically in Tanzania, reported that the flea is found in high densities in dwellings with dirt floors and thatched roofs [26]. In Africa, plague control emphasizes the control of rodents and their fleas [26].
The type of houses and the way of life are among the factors favouring the transmission of the plague. Indeed, the poor quality of houses can lead to many openings for rats wishing to enter the house and that the lack of hygienic sanitation constitutes a very favourable living environment for rodent reservoirs and vectors of the plague. Our study agrees with that of the literature which affirms that the way of life and the state of the house can favour the occurrence of plague. We suggest:
- Improve social conditions through the fight against poverty in order to promote descent housing and avoid promiscuous living.
- To raise awareness among the population so that it takes into account take into account the regulation of the materials to be used for the construction of houses.
- To raise the awareness of the inhabitants, especially in endemic regions, to conserve environmental hygiene by promoting sanitation measures.
- To sensitize the population for activities against rats and fleas.
- To fight against bush fires so that wild rats do not go to near houses.
- To educate the population through IEC (Information- Education-Communication) so that the inhabitants rigorously apply the measures hygiene and sanitation to reduce human-rat contact and contact Chipman. This measure is elementary to avoid any plague epidemic human.
- To increase the budget allocated to carrying out monitoring of the application knowledge acquired by the populations during the Information-Education- Communication.
Plague is a disease that still remains an important public health problem in the developing country while it is a scourge of the past for the developed countries. In Madagascar, the plague is still a disease to be fought and eradicated.
Conclusion
Our study reports 18 suspected and confirmed cases of plague recorded in 2013-2014 at the Ambohimandroso Andina medical center. Fever affected 88.89% of patients and lymphadenopathy 61% which constitute the major clinical manifestations. According to the WHO: “the importance of the number and species playing the role of reservoirs means that the disease can be controlled, but by no means eradicated” [22]. This is why in order to curb the plague, it is necessary to demand the intensification of community awareness and improved surveillance, especially in endemic areas.
References
-
Pierre A (2022) Doctor Bernard-Alex Gaüzère.
-
Wold Health Organisation (2009) Human plague: review of regional morbidity and mortality, 2004- 2009. Wkly Epidemiol Rec 85(6): 40-45.
-
Dennis DT, Gage KL, Gratz N, Poland J, Tikhomirov E, et al. (1999) Plague manuel : epidemiology, distribution, surveillance and control. WHO, Geneva, Switzerland, pp: 1-171.
-
Duplantier JM, Duchemin JB, Chanteau S, Carniel E (2005) From the recent lessons of Malagasy foci towards a gobal understanding of the factors involved in plague re-emergence. Vet Res 36(3): 437-453.
-
Snowden FM (2008) Emerging and re-emerging diseases: a historical perspective. Rev Immunological 225(1): 9-26.
-
Butler T (2013) Plague gives surprises in the first decade of the 21st century in the United states and wordwide. Am J Trop Med Hyg 89(4): 788-793.
-
Brygoo ER (1966) Epidémiologie de la peste à Madagascar. Arch Inst Pasteur Madagascar 35: 9-147.
-
Chanteau S, Ratsifasoamanana L, Rasoamanana B, Rahalison L, Randriambelosoa J, et al. (1998) Plague, a reemerging disease in Madagascar. Emerg Inf Dis 4(1): 101-104.
-
Stenseth NC, Atshabar BB, Begon M, Belmain SR, Bertherat E, et al. (2008) Plague: Past, present, and future. PLoS Medecine 5(1): e3.
-
Chanteau S, Boisier P, Carniel E, Duchemin JB, Duplantier JM, et al. (2004) Atlas of the plague in Madagascar. IRD/ Institut Pasteur of Madagascar, Marseilles, Madagascar, pp: 1-94.
-
Moulin AM (2006) The plague remains a serious threat. The story 310: 55.
-
Migliani R, Chanteau S, Rahalison L, Ratsitorahina M, Boutin JP, et al. (2006) Epidemiological trends for human plague in Madagascar during the second half of the 20th century: a survey of 20900 notified cases. Trop Med int Health 11(8): 1228-1237.
-
Carniel E (2002) La peste. C R Biologies 325(8): 851-853.
-
Prentice MB, Rahalison L (2007) Plague. Lancet 369(9568): 1196-1207.
-
Pasteur Institute of Madagascar (2006) Plague Study Group. Atlas of the plague in Madagascar. IRD.
-
Duchemin JB, Ratovonjato J, Duplantier JM (2003) Siphonaptera, Fleas, Parasy Gasy. In: Goodman SM, Benstead JP (Eds.), The natural history of Madagascar. University of Chicago Press, Chicago, USA, pp: 687-692.
-
Chanteau S, Ratsitorahina M, Rahalison L, Rasoamanana B, Chan F, et al. (2000) Current epidemiology of human plague in Madagascar. Microbes Infect 2(1): 25-31.
-
Migliani R, Ratsitorahina M, Rahalison L, Rakotoarivony I, Duchemin JB, et al. (2001) Resurgence of plague in the district of Ikongo in Madagascar in 1998. 1. Epidemiological aspects in the human population. Bull Soc Pathol Exot 94(2): 115-118.
-
Sinyange N, Kumar R, Inambao A, Moonde L, Chama J, et al. (2016) Outbreak of Plague in a High Malaria Endemic Region-Nyimba District, Zambia, March-May 2015. MMWR Morb Mortal Wkly Rep 65(31): 807-811.
-
Ratsitorahina M, Chanteau S, Rosso ML, Randriambelosoa J, Ratsifasoamanana L, et al. (2002) Epidemiological news of the plague in Madagascar. Arch Inst Pasteur de Madagascar 68(1-2): 51-54.
-
Njunwa KJ, Mwaiko GL, Kilonzo BS, Mhina JIK (1989) Seasonal patterns of rodents, fleas and plague status in the Western Usambara Moutains, Tanzania. Med Vet Entomol 3(1): 17- 22.
-
Davis S, Makundi R, Leirs H (2006) Demographic and spatio-temporal variation in human plague at a persistent focus in Tanzania. Acta Trop 100(1-2): 133- 141.
-
Perry RD, Fetherston JD (1997) Yersinia pestis etiologic agent of plague. Clin Microbiol Rev 10(1): 35-66.
-
Bertherat E, Bekhoucha S, Chougrani S, Razik F, Duchemin JB, et al. (2007) Plague réappearance in Algeria after 50 years, 2003. Emerg Inf Dis 13(10): 1459-1462.
-
Boisier P, Rahalison L, Rasolomaharo M, Ratsitorahina M, Mahafaly M, et al. (2002) Epidemiologic features of four successive annual outbreaks of bubonic plague in Mahajanga, Madagascar. Emerg Infect Dis 8(3): 311-316.
-
Laudisoit A, Leirs H, Makundi RH, Van DS, Davis S, et al. (2007) Plague and the human flea, Tanzania. Emerg Infect Dis 13(5): 687-693.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria