Persistence of Measles Transmission despite of Measles Elimination Program Progressing
The number of measles cases per million was plotted in linear scale or in logarithmic scale in the vertical axis along years from 1974 to 2021 in the horizontal axis. In the linear scale plot, measles cases persisted with consecutive peaks till early 1990s and then became invisible. In logarithmic scale plot, the plots were horizontally distributed at high level till early 1990s and declined to lower level with ups and downs. Though proportion of measles cases in older population gradually increased over time, as of 2021, the number of measles cases was still correlated with population size of age group
Introduction
In 2010, the World Health Assembly established 3 milestones towards the future eradication of measles to be achieved by 2015. Reducing and maintaining annual measles incidence to less than 5 cases per million by 2015 was one of the milestones (https://www.who.int/news-room/fact- sheets/detail/measles). Progress of measles elimination in Western Pacific region was reviewed for years 2013-2017 by Hagan JE, et al. [1] and for years 2017-2022 by Durrheim N, et al. [2]. This paper examines progress of measles elimination in longer time span, from 1974 to 2021, for countries in Western Pacific, Southeast Asia, Europe and America.
Data source
- Measles data were derived from Global Health Observatory data repository (https://apps.who.int/ gho/data/view.main.1540_62?lang=en)
- Vaccine coverage was derived from measles immunization rate-country rankings (https://data. worldbank.org/indicator/SH.IMM.MEAS)
Epidemic Curves
The number of measles cases per 1,000,000 populations was plotted in linear or in logarithmic scale in the vertical axis along years starting from 1974 to 2021 in the horizontal axis (Figure 1). In the linear scale plot (Figures A1-C1), the epidemic curves consisted of successive spikes of different sizes till early 1990s followed by sporadic spikes [3]. In the logarithmic scale plot (Figures A2-C2), the epidemic curves were near horizontal till 2000, when they started declining with ups and downs to the level of 5/1,000,000. Countries whose wave peaks exceeded 100/1,000,000 later than 2000 were highly populous countries, e.g., Philippines, Viet Nam and Lao PDR in Western Pacific and India, Indonesia and Bangladesh in Southeast Asia (Figure B2), and Bulgaria, Romania and Ukraine in Europe (Figure C2).
Canada (90%) USA (91%) Colombia (90%) Ecuador (81%) Brazil (79%) Peru (77%) Paraguay (80%) Argentina (77%) Chile (91%) Australia (95%) New Zealand (91%) Papua New Guinea (47%) Mongolia (87%) Rep Korea (95%) Japan (98%) China (99%)
2000.0 A1
Malaysia (95%) Lao PDR (79%) Philippines (72%) Cambodia (84%) Vanuatu (50%) Fiji (96%) Viet Nam (89%) Singapore (95%) India (89%) Bangladesh (97%) Indonesia (72%) Sri Lanka (96%)
Belgium (96%) France Germany (97%) Netherlands (94%) Switzerland (97%) Croatia (91%) Italy (92%) Latvia (99%) Hungary (99%) Estonia (91%) Finland (96%) Denmark (94%) Norway (97%) Sweden (97%) Russian (97 %) Bulgaria (88%) Ukraine Romania C1
Figure 1: Epidemic curves of measles in America (panels A1-A2), in Western Pacific (panels A1-A2 and B1-B2), in Southeast Asia (panels B1-B2) and in Europe (panels C1-C2). Vertical axis: number of measles cases/1,000,000 population/year in linear scale (panels A1, B1 and C1) or in logarithmic scale (panels A2, B2 and C2). Horizontal axis: year starting from 1974 till year 2021. The level of 5 cases per million, targeted level of measles incidence, is indicated by a dotted line in Figs. 1A2, 1B2 and 1C2. Year 2015, target year of the measles elimination is shown in the top of panel A2 with a downward arrow in Figure 1A2.
Vaccine Coverage
Vaccine coverage among children in 12-23 months of age in 2020 was obtained from World Bank’s data base (https://data.worldbank.org/indicator/SH.IMM.MEAS) and from Measles immunization rate - country rankings (https://www.theglobaleconomy.com/rankings/measles_ Canada (90%) USA (91%) Colombia (90%) Ecuador (81%) Brazil (79%) Peru (77%) Paraguay (80%) Argentina (77%) Chile (91%) Australia (95%) New Zealand (91%) Papua New Guinea (47%) Mongolia (87%) Rep Korea (95%) Japan (98%) China (99%)
10000.0 A2 Target year 2015
0.0 Malaysia (95%) Lao PDR (79%) Philippines (72%) Cambodia (84%) Vanuatu (50%) Fiji (96%) Viet Nam (89%) Singapore (95%) India (89%) Bangladesh (97%) Indonesia (72%) Sri Lanka (96%) B2
0.01 Belgium (96%) France Germany (97%) Netherlands (94%) Switzerland (97%) Croatia (91%) Italy (92%) Latvia (99%) Hungary (99%) Estonia (91%) Finland (96%) Denmark (94%) Norway (97%) Sweden (97%) Russian (97 %) Bulgaria (88%) Ukraine Romania
100000.0 C2
In Figure 1, the vaccine coverage is shown in parenthesis after the country name. Among 47 countries, vaccine coverage was >90% in 30 countries, 80-90% in 9 countries and 80% or less in 8 countries. In Europe, the number of the patients per population remained high in Romania, Ukraine and Bulgaria
in comparison with other countries. Vaccine coverage was 75% (2 doses of MMT vaccine in 2017) for Romania [4], 85% (for first dose) for Ukraine (https://www.who.int/ europe/news/item/27-04-2022-ukraine--immediate- steps-needed-to-prevent-a-measles-outbreak-due-to-the- ongoing-war-and-low-vaccination-rates--warns-who) and 88% for Bulgaria. In Western Pacific, measles epidemic persisted in Viet Nam, Philippines and Cambodia, where the vaccine coverage was 89%, 72% and 84%, respectively. The data appeared to suggest that vaccine coverage >90% was required for eliminating measles.
Discussion
The above data suggested that measles epidemic was on decline in countries in America and Europe and several countries in Western Pacific and Southeast Asia. It owes much to the measles vaccination program that was implemented first in Pan American Health Organization (PAHO) (https://www3.paho.org/hq/index. php?option=com_content&view=article&id=12526:measles- elimination-in-the-americas&Itemid=0&lang=en#gsc.tab=0). The present analysis confirmed that the measles vaccine was a powerful tool for eliminating measles. Nevertheless, measles persisted in India and Bangladesh in Southeast Asia where vaccine coverage was 89% and 97%, respectively. In depth investigation, including geographical distribution of the patients, age distribution, vaccine cold chain, etc. is needed.
An emerging issue related to elimination of measles is increase of measles among older age groups. For example in Japan, while 40 % of the measles cases were younger than 9 years in 2008-2010, in 2019, only 15% of the measles cases were younger than 9 years and about 70% were older than 20 years (https://www.niid.go.jp/niid/ja/measles-m/measles- iasrtpc/8732-470t.html). In Europe, 41% of the patients were older than 9 years in 2019 [4]. Increasing proportion of measles cases among older age groups was reported from India in 2017 [5]. In front of such situations, there is concern that intensifying routine vaccination to younger age group may not be able to eliminate measles.
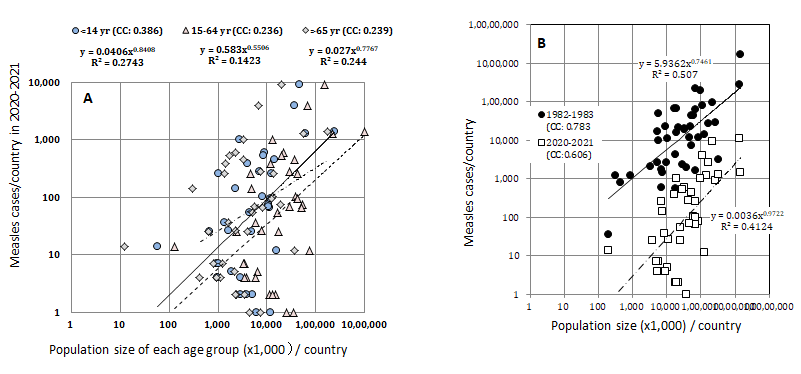
Figure 2: Relation between the population size and measles cases. Panel A: Plots for examining which age group was best correlated with measles epidemic. For each country, the number of the measles cases in 2020-2021 was plotted in the vertical axis against population size of age groups <14 years, 15-64 years and > 65 years of the countries both in the logarithmic scale. Correlation was significant only for age group <14 years with correlation coefficient (cc) 0.3862. [Note: if measles cases for different age groups were available for all the countries, this graphic was not necessary.] Panel B: The number of measles cases is plotted in the vertical axis against the population size for countries appearing in Fig. 1 in the horizontal axis both in the logarithmic scale. ●: year 1982-1983; □: 2020-2021. [Note: countries with zero reporting are excluded from plots in the logarithmic scale.
So as to deal with this issue, I tried to identify which age group(s) was the major determinant of current measles epidemic. For this purpose, I plotted the total number of measles cases per country in the vertical axis against the population size of age groups, <14 years, 15-64 years and >64 years in the horizontal axis (population data were derived from https:// en.wikipedia.org/wiki/List_of_countries_by_age_structure) (Figure 2A). In this plot, if the epidemic was represented mainly by population of 15-64 years of age, for example, the correlation between the total number of measles cases and the population size of 15-64 years of age would be the highest. As a matter of fact, the correlation was the highest for age group <14 years, current vaccination target population, with correlation coefficient 0.3826 against correlation coefficient 0.2363-0.2394 for the other age groups. Thus, despite of increasing measles cases among older age groups, the current vaccination schedule targeting at younger population was found still appropriate. Actually, measles incidence has been steadily decreasing in the present schedule (Figure 2B). Finally, monitoring the epidemic both in logarithmic and linear scales is useful for following measles epidemics whose epidemic size varies by an order of magnitude in time and in space.
References
-
Hagan JE, Kriss J, Takashima Y, Mariano KML, Pastore R, et al. (2018) Progress Toward Measles Elimination- Western Pacific Region, 2013-2017. MMWR Morb Mortal Wkly Rep 67(17): 491-495.
-
Durrheim N, Baker MG, Capeding MR, Goh KT, Lee D, et al. (2022) Accelerating measles elimination in the Western Pacific Region during the calm between the storms. Lancet Reg Health West Pac 23: 100495.
-
Yoshikura H (2018) Population size dependency of measles epidemic that was scalable from Japanese prefectures to European countries. Jpn J Infect Dis 71(5): 325-332.
-
Habersaat KB, Pistol A, Stanescu A, Hewitt C, Grbic M, et al. (2020) Measles outbreak in Romania: understanding factors related to suboptimal vaccination uptake. Eur J Public Health 30(5): 986-992
-
Rathi P, Narendra V, Sathiya V, Kini S, Kumar A, et al. (2017) Measles outbreak in the adolescent population- matter of concern? J Clin Diag Res 11(8): LC20-LC23.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria