Systematic Review of Institutional Scabies Outbreaks in Sub Saharan Africa
Background: Scabies is an important global health problem largely affecting low and middle-income countries in poor and overcrowded areas. Until recently, there has been paucity of data on the epidemiology of scabies in Sub-Saharan Africa and in particular community and facility based level estimates of disease burden. The aim of this systematic review is to identify and describe the literature on institutional scabies outbreaks across Sub Saharan African countries. Methodology: International databases (MEDLINE, EMBASE, Global Health), African Wide Portal and grey literature were systematically searched from July 1, 2020 to July 31, 2020. The data were analysed using STATA Version 16.1 and described through narrative synthesis. Results: Eight studies were included in this systematic review and analysed for prevalence estimation of scabies outbreaks in institutions. The outbreaks were most frequently reported in schools (n = 4) and religious institutions (n = 3). On average, scabies outbreaks persisted for 3 months (90 days) and the median attack/prevalence rate was 22.5%. Conclusion: The burden of institutional scabies outbreaks is under reported in Sub Saharan Africa . More research and practice emphasis must be paid to prevent scabies outbreaks in both community and institutional settings
Introduction
Background
Scabies is a global health problem largely affecting low and middle-income countries with a disproportionate burden on children and the elderly living in poor and overcrowded areas [1]. Globally, it has been estimated to affect over 200 million people with the prevalence rate of scabies infections variying between 0.2% to 71.4 % [2].
Up until recently, there has been paucity of data on the epidemiology of scabies in Sub-Saharan Africa and in particular community and facility based level estimates of disease burden [3]. There is more recent data from Ethiopia, Liberia, Nigeria, Cameroon, Malawi and Ghana which all suggest that scabies is a major public health problem in sub-Saharan Africa [4, 5, 6, 7, 8, 9]. The predisposing factors are overcrowding, poor personal hygiene, low socio-economic standards and impaired host immunity [5, 10]. The clinical features of scabies follow the invasion of the adult female S scabiei var hominis mites into the top layer of epidermis causing serpentine burrows using proteolytic enzymes to dissolve the stratum corneum .This results in the infected individual developing an allergic hypersensitive reaction to the presence of mite proteins and faeces in the scabies burrow, causing intense itch and rash [1, 11]. The persistent itch may lead to excoriations from scratches, exposing the skin to secondary bacterial infections that result in cellulitis, impetigo, and pyoderma [12, 13, 14].
Apart from the clinical manifestations, this disease is associated with reduced quality of life causing psychosocial, and emotional consequences to the affected populations [8, 9]. Scabies is a significant cause of morbidity and a potential source of economic burden in most low and middle- income countries. It imposes a considerable financial burden on individuals, families, communities, and the country`s health systems [1]. Early diagnosis of scabies is crucial in avoiding outbreaks, preventing exposure to unnecessary treatment, significant morbidity, and increased economic burden [1, 15]. The diagnosis has been quite challenging in most low income countries, as clinical diagnosis is still the most common method of disease confirmation [6]. In the past decade, evidence from literature has shown that there was no standardized technique for diagnosing scabies to facilitate communication and comparison of epidemiological and clinical findings and the development of scabies control strategies [16].
To address this issue, The International Alliance for the Control of Scabies (IACS) Criteria [17] was developed through a Delphi study with international experts panel where detailed expert opinions and recommendations were obtained and combined with a comprehensive review of the available literature to develop uniform, evidence‐based definitions and consistent diagnostic methods [17, 18].
The main public health interventions for scabies control are intensified disease management (IDM) and preventive chemotherapy [19]. The magnitude of community and institutional scabies outbreaks is still being underestimated. Evidence from literature has reported scabies outbreaks to have occurred in the hospitals, prisons, orphanages, schools, army barracks and nursery homes across the world [20]. The aim of this systematic review is to identify and describe the literature on scabies outbreaks within facility based settings, explore epidemiological risk factors, its progression and response across Sub Saharan African countries.
Materials and Methods
A systematic review was performed on reported institutional outbreaks of scabies following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [21].
Literature Search
The databases searched between July 1st 2020 to 31st 2020 with reasons were Ovid Medline (clinical) , Embase (clinical), Africa Wide Information (African studies), Global Health ( International public health), London School of Hygiene and Tropical Medicine library catalogues and grey literature using the keywords.
Grey literature search was performed by seeking reports not published in peer-reviewed journals through a request via newsletter to the members of the International Alliance for the Control of Scabies, a search of conference abstracts of meetings of the International Society of Dermatology , Training Programs In Epidemiology and Public Health Intervention Network and Field Epidemiology and Laboratory Training programmes. Reference harvesting and individual searches for author names were further carried out to identify further relevant articles. No language restrictions or time limits were applied.
Study eligibility
Eligibility Criteria
Inclusion criteria were defined according to the populations, interventions, comparisons, outcomes and study type (PICOS) framework, a model adopted by the Cochrane Library to structure rigorous reviews on health- related questions. The inclusion and exclusion criteria were as follows (Table 1).
| Population | All ages, gender, and socioeconomic populations were included |
|---|---|
| Any studies conducted in an institution or a community outbreak extending to an institution or vice versa in a Sub Saharan African country were included | |
| Intervention | Scabies outbreak investigation and response |
| Comparator | Any counterfactual or none |
| Outcome of interest | Prevalence of scabies outbreaks within institutions in SSA |
| Risk factors associated with institutional scabies in SSA | |
| Treatment options for institutional scabies in SSA | |
| Study design | Case reports and Case-control studies |
| Cross-sectional studies and/or Cohort studies | |
| Conference proceedings e.g. abstracts | |
| Ecological studies | |
| Randomised control trials and Non- randomised control trials | |
| Exclusion Criteria | This was used to peruse the titles and abstracts for suitability and an outbreak focus |
| Not institution-based or extending to an institution | |
| Not related to humans and Not conducted in SSA | |
| Not related to scabies | |
| Articles including newspapers, blogs, or opinion pieces | |
| General epidemiological studies | |
| Qualitative studies | |
| Single case studies without methodology |
Table 1: PICOS.
Quality assessment and Study Selection
The Critical Appraisals Skills Programme (CASP) checklists were used for case control and cohort studies [22]. The AXIS tool was employed for cross sectional study. Mixed method was used for Newcastle Ottawa Scale (NOS) was used to grade all the studies into low (0-3), moderate (4- 7), or high risk of bias (8-10). Two reviewers independently provided quality assessment of the articles at all stages. At the initial step, the two reviewers independently scanned through the titles and abstracts of the articles retrieved from the databases. The relevance of the studies was assessed, and the articles selected were further screened. After screening for eligibility, the remaining full texts were assessed for quality. For studies with unclear methods, the authors were contacted to seek clarification.
These checklists assessed the aim, risk of bias, statistical methods, measurement of exposures/outcomes, and relevance, among other criteria. The overall sections ask: “Are the results valid?”, “what are the results?” and “will the results help locally?” If the study failed to respond to these initial questions or a large flaw regarding a criterion was found, the study was rejected.
Data extraction analysis and Synthesis
An extraction form was prepared and was pilot-tested using three-outbreak investigation reports. Extracted data that was relevant to the objectives and guided by a recent systematic review on scabies outbreaks by Mounsey, et al. [23] included : author, year, country, type of institution, sample population, case definition, duration of an outbreak, numbers infected, attack or prevalence rates, diagnostic method, treatments utilized, details of the index case, risk factors and other notes.
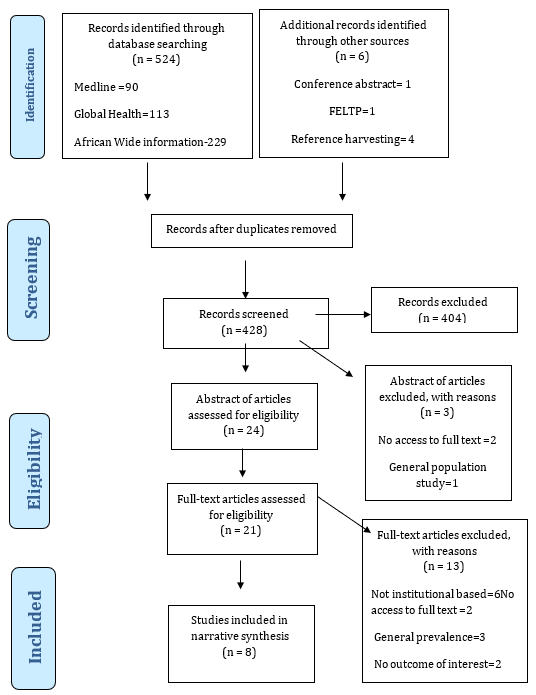
Due to the variability of the study designs, outcome measures and high degree of heterogeneity, the intention to conduct a meta-analysis could not be realised. The tabular presentation was well thought of and worked into such that it would make an appreciation of the intended aims and objectives very clear and succinct. This was followed by the descriptive analysis, narrative synthesis, and overall summary of public health importance of the study (Figure 1).
Results
Overview and characteristics of included studies in the narrative synthesis in this review, a total of 8 outbreaks in 3,348 respondents were reported between years 2000 to 2019 in Ethiopia, Ghana and Tanzania [9, 24, 25, 26, 27, 28]. The studies varied in research methods, country of origin, target population and study site. Case control studies were the most common study design method used (6 studies), followed by cross-sectional study and the remaining was a prospective cohort study.
The preliminary outbreak investigation was conducted in institutional settings in rural areas with the nearest health facilities being health posts, health centre, private clinics, and a district hospital. Majority of the eligible studies reported one outbreak involving one facility (n = 5). However, the study conducted by Sara, et al. [28] described a scabies outbreak that extended to the community from 2 primary schools. While studies conducted by Badeso, et al. [24] described scabies outbreaks reported from 5 madrasahs (Islamic religious schools) and 25 primary schools respectively [24, 26].
The most affected facilities were religious institutions and schools. The duration of outbreaks ranged from less than one month to over 6 months with four papers illustrating this information the form of epidemic curve. With few exceptions, poor surveillance, delayed detection and response was identified as a cause of prolonged transmission [24, 25, 27, 29]. While the average number of people infested per outbreak was 164, numbers varied markedly, from as low as 32 [27], to as high as 883 [25] in a prison setting.
Risk Factors Affecting Scabies Outbreaks
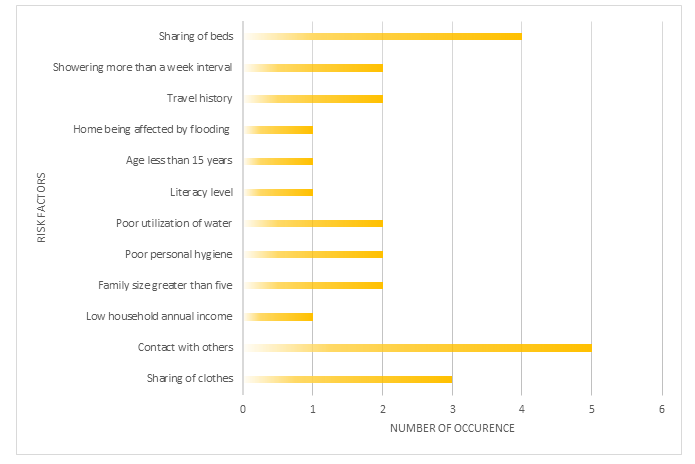
Most of the reviewed studies pointed out several risk factors that might have facilitated the occurrence and spread of outbreaks. The most frequently observed cause was person to person transmission through contact with infected person or via sharing of clothing or sleeping in the same quarters. Three studies identified index cases who had travel history from scabies epidemic areas within last two months prior to the onset of symptoms [24, 27, 29].
Kaburi, et al. [9] reported seating in pairs due to overcrowded classes and sharing of sleeping mats during siesta as contributing factors towards propagation of the outbreak among pre-school children [9]. Sara, et al. [28] described home being affected by flood as a significant risk factor citing displacement, overcrowding and poor personal hygiene which in turn leads to increased susceptibility to scabies infestation. Additionally, suboptimal hand hygiene became a more critical factor that facilitated the transmission of secondary bacterial infections including pyoderma in 60% of the cases. Two of the studies listed family size greater than 5 as a significant risk factor (Figure 2).
Diagnosis and Clinical Presentation of Scabies
‘Suspected case’ definitions were described in 5 papers. Three papers were identified in which no case definitions were evaluated; one was a conference abstract. There were no consistent criteria used for diagnosis in the included studies for scabies. Three studies reported clinical diagnosis made by trained healthcare professionals [9, 25, 26]. To avoid inter- and intra-operative error of reliability, at least two public health personnel had to agree on the case definition and clinical diagnosis for scabies to be added to the line list.
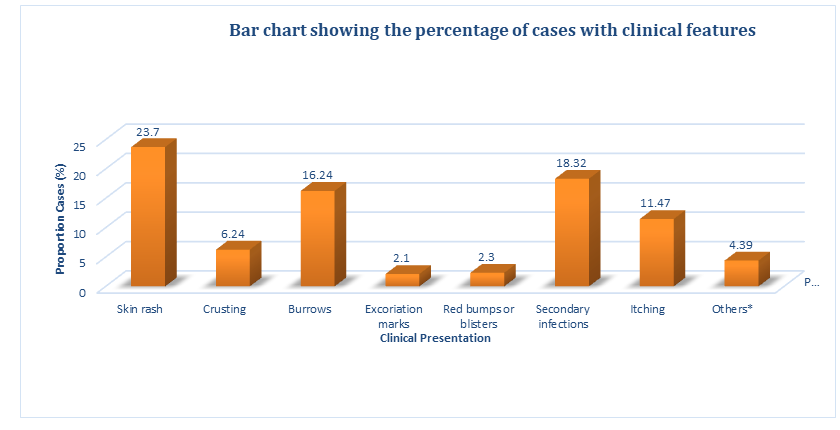
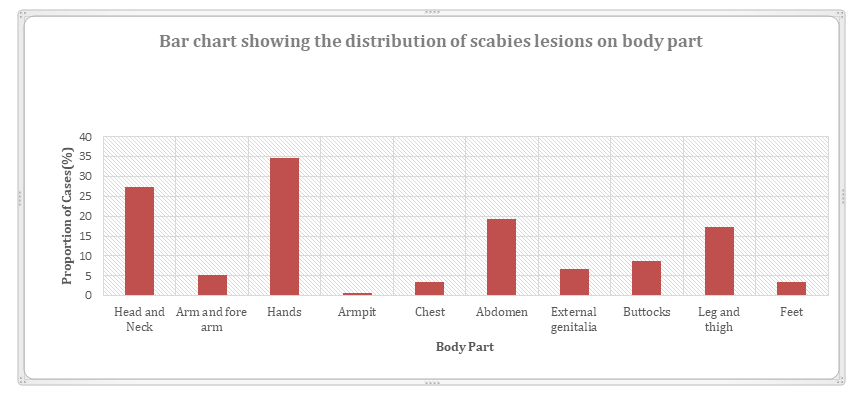
The diagnosis was based on the presence of the typical clinical signs and symptoms using a structured checklist developed by trained healthcare professionals. However, only two studies Kaburi, et al. [9] had a confirmed case definition of scabies demonstrating the presence of mite and its products on skin scraping. Regarding the distribution of scabies rash on the body parts, interdigital space (n=4) was the most affected area followed by the flexor aspect of the wrists, elbows, buttocks, and abdomen (n=2) as shown in Figure 3. Figure 4 illustrates the most reported clinical presentation among the cases.
Treatment and Management of Scabies Outbreaks
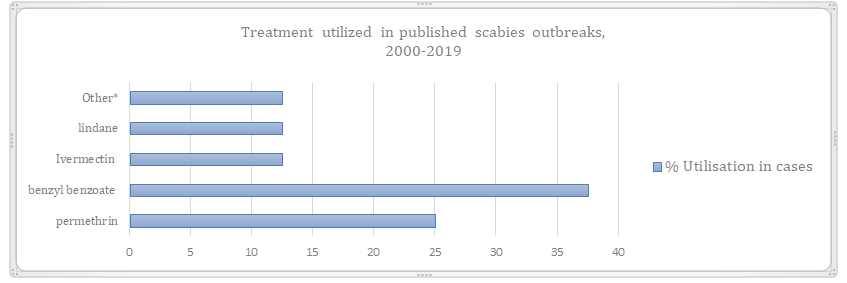
Most facilities notified public health authorities about the outbreaks and received advice and assistance to manage the outbreaks. Following the detection of the index cases, four reports on scabies outbreaks conducted active case finding among residents and staff by contact tracing. Responding to the outbreaks, treatment measures for the cases and its contacts included mass drug treatment with benzoyl benzoate (n=4), 5% permethrin dermal cream (n=3), single oral dose of ivermectin 150 mgkg (n=1) and 1% lindane as seen in Figure X below. Only one study reported that 64% of cases refused treatment at the nearest health facility [28]. Control measures included referral and transfer to a municipal hospital in two studies [9, 28]. Other measures included were health education and dissemination with emphasis on personal hygiene, sharing of beds and clothes.
The personal hygiene week was declared and performed in two studies [27, 29]. Alebachew, et al. [29] highlighted church community mobilisation and communal cleaning of the shared clothing, bedding, and linens used by an infested individual.
Kaburi, et al. [9] further conducted environmental assessment of the state of classrooms, average class occupancy, seating arrangement, sleeping conditions during siesta, washroom hygiene, and the general state of cleanliness of the school premises. Close follow-up of cases and re-screening was reported only in two studies. The overall highest attack rate was recorded in Tanzanian prison 81.8% (followed by Ethiopian church and primary schools with an attack rate of 35 and 25% respectively. The lowest attack rate was recorded in Ghana and Ethiopia in the basic and primary schools. No case mortality was recorded in any of the studies (Figure 5).
Risk of Bias
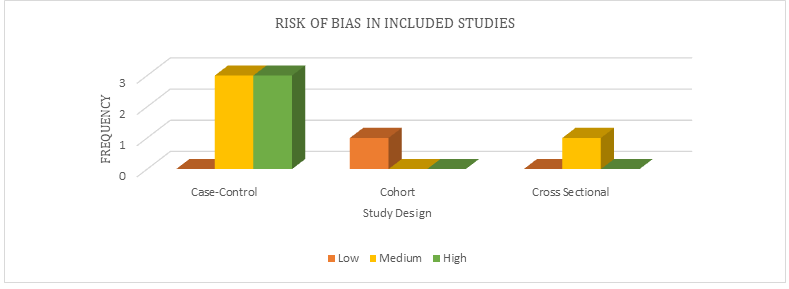
The quality of 8 studies was assessed and the results are summarized in Figure 4. Six studies scored high risk of bias for all the criteria points. Two studies were at low and medium risk for all criteria respectively [9, 25]. Problems related to recall bias and standardization of self-reported measurement created a high risk of bias for the measurement of the exposure domain in six studies. The problem related to missing data resulted in a high risk of bias.
Figure 6 demonstrates a preponderance of low-quality studies, which limits the strength of recommendations that this report can make due to the high potential for biased outcomes. The main problems were small sample sizes, subjective measures, missing information, and no adjustment for confounding.
Discussion
Infectious disease outbreaks cause millions of deaths across the African region annually [30]. This systematic review includes published studies from the past 20 years illuminating the continuous burden that scabies has presented to the Sub Saharan African region. Scabies outbreaks were most reported in rural communities. With lack of easy access to health facilities and poorer health infrastructure than urban communities, this can create a cyclical burden where most infected people will either receive delayed treatment or no treatment at al thus worsening the outbreak progression as observed in an institution based extended to community outbreak in Ethiopia [28].
Globally, most of the research on scabies outbreaks has been carried out in urban settings, and has focused mainly on prevalence and socio economic aspects [23]. However, these crucial data on scabies outbreaks in both rural and urban communities are greatly lacking in Sub Saharan region and is vital for control of institutional outbreaks [10].
The duration of outbreaks varied for each facility with the churches and prison recording the highest duration of outbreaks of more than 4 months. The possible reasons for the prolonged outbreak may be due to delay in identification of the index case, delayed diagnosis and prompt treatment of contacts and cases. Thereby, suggesting that accurate identification of how scabies spread is a fundamental step in outbreak control.
In the current systematic review, overall incidence (attack rate) in the general population ranged from 11-88%. Few papers presented a breakdown of scabies outbreaks prevalence rates by smaller age groups, making a reliable comparison of the disease distribution across age groups difficult between studies. However, the highest scabies incidence was described in preschool children less than 3 years (17%), in older children aged 5-14 (56%) and adults aged 20-29 (47%) years in prison.
Children in primary school were most affected populations, and most of them had sign of secondary infection attributable to scabies. This might be due to the fact that younger children, particularly, those at school are at high risk of scabies infestations as the school environments may increase the susceptibility of cross-infestation and increase contacts which can be passed to family members and others.
This high burden of scabies seems to support the hypothesis that infections occur more often in young children as it has been observed in other low and middle- income countries, where scabies is an endemic disease [10]. The high incidence of scabies among young adults in prison may be due to the frequent close interpersonal contact and overcrowding.
Another objective of this study was to identify factors associated with scabies outbreaks in institutions. Most of the reviewed studies pointed out several issues in practice that might have facilitated the occurrence and spread of outbreaks. The most frequently observed cause was person to person transmission through contact with infected person or sleeping in the same quarters. This result is consistent with the systemic review conducted on scabies in developing countries showing that overcrowding especially sleeping with scabies case is an important risk factor [1] and a systematic review on prevalence and associated risk factors in Ethiopia showing that sharing of bed with an infected person is a risk factor [5]. The diagnosis was mostly made clinically with no clear details on the criteria used. Only five studies reported a case definition and only two studies on specific diagnostic criteria for the health professionals to follow. No standardized method such as IACS was used.
It was also observed that there was lack of dermatologists or experienced doctors available to make accurate diagnosis relying heavily on community extension workers which may have led to delay in diagnosis. As the diagnosis of scabies was made clinically, false- positive and false-negative diagnoses may have occurred.
Strengths and Limitations
This is the first systematic review conducted in Sub Saharan Africa to bridge the gap on our knowledge and extent of the burden of institutional scabies outbreaks. This review also explored and summarized critical issues facilitating the spread of the outbreaks and certain control measures, which have not been addressed in detail in the previous review [23]. Lessons learned from the results of this review would enable better prevention and control of outbreaks in institutions in the future.
This review has several limitations. One of the major limitations of this study was that there were very few publications reports available thereby under reporting the real burden of scabies outbreaks in institutions. Secondly, there was considerable heterogeneity among the studies mostly to differences in study design, methodology and missing information. Parameters like case definition, details of diagnosis, treatment regimens, and number of individuals infected vs. the overall numbers of people exposed or prophylactically treated were not stated, precluding assessment of attack rates and definition of cure were often reported poorly or not at all .This reduced the precision of the study.
Recommendations
This systematic review identified several challenges to overcome in scabies outbreak management in institutions and the following recommendations have been proposed:
- Firstly, to mitigate the risk of institutional scabies outbreaks an improved scientific method of outbreak reporting should be implemented. This can be done by provision of resources, developing mandatory reporting standardized checklists for each facility including and encouragement to publish for peer review. The public health emergency management team should regularly perform institutional health inspection for early detection and prompt treatment of health-related problems.
- Secondly, due to the late detection and response to outbreaks as seen in this review, primary health care centres and district hospitals have to improve their active surveillance and control response Additionally, high index of suspicion among health care professionals should be maintained .This can be done through quality training of community health workers and collaborative efforts with multiple experts from the Field Epidemiological Laboratory Training on IACS.
- Finally, research attempts should be made to improve the geographic representation of data and the methodological rigor of the studies (including standardization of data recording), and to obtain more data documenting the frequency and consequences of scabies epidemics at the primary healthcare level and in the community, and the role of etiological factors of practical relevance.
Conclusion
The burden of institutional scabies outbreaks is under reported in Sub Saharan Africa. More research and practice emphasis must be paid to improve diagnostic methods, surveillance and prompt management of crusted scabies to prevent the development of scabies outbreaks in both community and institutional settings.
References
-
Hay RJ, Steer AC, Engelman D, Walton S (2012) Scabies in the developing world-its prevalence , complications, and management. Eur Soc Clin Infect Dis 18(4): 313-323.
-
Archipelago B, Id MM, Sammut T, Cabral MG, Teixeira E, et al. (2019) The prevalence of scabie, pyoderma and other communicable dermatoses in the 121: 1-9.
-
Engelman D, Steer AC (2018) Control Strategies for Scabies. Trop Med Infect Dis 3(3): 98.
-
Mitja O, Esteban S, Kafulafula J, Mtenje H, Thauzeni G, et al. (2021) A facility and community-based assessment of scabies in rural Malawi. PLoS Negl Trop Dis 15(6): e0009386.
-
Azene AG, Aragaw AM, Wassie GT (2020) Prevalence and associated factors of scabies in Ethiopia : systematic review and Meta-analysis. BMC Infectious Diseases 20: 380.
-
Ugbomoiko US, Oyedeji SA, Babamale OA, Heukelbach J (2018) Scabies in Resource-Poor Communities in Nasarawa State, Nigeria: Epidemiology, Clinical Features and Factors Associated with Infestation. Trop Med Infect Dis 3(2): 59.
-
Kouotou EA, Nansseu JRN, Kouawa MK, Zoung-Kanyi Bissek AC (2016) Prevalence and drivers of human scabies among children and adolescents living and studying in Cameroonian boarding schools. Parasites and Vectors 9(1): 400.
-
Collinson S, Timothy J, Zayay SK, Kollie KK, Lebas E, et al . (2020) The prevalence of scabies in Monrovia, Liberia : a population-based survey. PLoS Negl Trop Dis 14(12): e0008943.
-
Kaburi BB, Ameme DK, Asumah GA, Dadzie D, Tender EK, et al. (2019) Outbreak of scabies among preschool children, Accra, Ghana, 2017. BMC Public Health 19(1): 746.
-
Romani L, Steer AC, Whitfeld MJ, Kaldor JM (2015) Prevalence of scabies and impetigo worldwide: A systematic review. Lancet Infect Dis 15(8): 960-967.
-
Hengge UR, Currie BJ, Jäger G, Lupi O, Schwartz RA (2006) Scabies: a ubiquitous neglected skin disease. Lancet Infectious Diseases 6(12): 769-779.
-
Chosidow O, Fuller LC (2017) Scratching the itch: is scabies a truly neglected disease?. Lancet Infect Dis 17(12): 1220-1221.
-
dos Santos MM, Amaral S, Harmen SP, Joseph HM, Fernandes JL, et al. (2010) The prevalence of common skin infections in four districts in Timor-Leste: a cross sectional survey. BMC Infect Dis 10: 61.
-
Thornley S, Marshall R, Jarrett P, Sundborn G, Reynolds E, et al. (2018) Scabies is strongly associated with acute rheumatic fever in a cohort study of Auckland children. J Paediatr Child Health. 54(6): 625-632.
-
Mccarthy JS, Kemp DJ, Walton SF, Currie BJ (2004) Scabies: more than just an irritation. Postgrad Med J80(945): 382-387.
-
Thompson MJ, Engelman D, Gholam K, Fuller LC, Steer AC (2017) Systematic review of the diagnosis of scabies in therapeutic trials. Clin Exp Dermatol 42(5): 481-487.
-
Engelman D, Yoshizumi J, Hay RJ, Osti M, Micali G, et al. (2020) The 2020 International Alliance for the Control of Scabies Consensus Criteria for the Diagnosis of Scabies. Br J Dermatol 183(5): 808-820.
-
Engelman D, Fuller LC, Steer AC (2018) Consensus criteria for the diagnosis of scabies : A Delphi study of international experts. PLoS Negl Trop Dis 12(5): e0006549.
-
Brohman IT, Sherman W, Repasky M, Beuming T (2013) Improved Docking of Polypeptides with Glide. J Chem Inf Model 53(7): 1689-1699.
-
Weigl JAI (2018) Fallhäufungen von Skabies an Schulen und Einsatz von Ivermectin Outbreaks of Scabies in Schools and Use of Ivermectin. Gesundheitswesen 80(4): 360-364.
-
Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP (2010) Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Int J Surg 8(5): 336-341.
-
Downes MJ, Brennan ML, Williams HC, Dean RS (2016) Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 6(12): e011458.
-
Mounsey KE, Murray HC, King M (2020) Retrospective analysis of institutional scabies outbreaks from 1984 to 2013: lessons learned and moving forward. 144(11): 2462-2471.
-
Badeso MH, Ferede HA, Kalil FS (2020) Scabies outbreak investigation among madrasahs in Sinana district, Bale Zone, Oromia, Ethiopia, May 2019. Research Square.
-
Leppard B, Naburi AE (2000) The use of ivermectin in controlling an outbreak of scabies in a prison. Br J Dermatol, 143(3): 520-523.
-
Ejigu K, Haji Y, Toma A, Tadesse BT (2019) Factors associated with scabies outbreaks in primary schools in Ethiopia: a case–control study. Res Rep Trop Med 10: 119-127.
-
Town G, Yassin ZJ, Dadi AF, Nega HY, Derseh BT, et al. (2017) Scabies Outbreak Investigation among “ Yekolo Temaris ”. pp: 203-209.
-
Sara J, Haji Y, Gebretsadik (2018) A Scabies Outbreak Investigation and Risk Factors in East Badewacho District, Southern Ethiopia: Unmatched Case Control Study. Dermatol Res Pract 26: 7276938.
-
Alebachew H (2017) Scabies outbreak investigation in Addet town, West Gojjam Zone, Amhara region, Northwest Ethiopia.
-
Mboussou F, Ndumbi P, Ngom R, Kassamali Z, Ogundiran O, et al. (2019) Infectious disease outbreaks in the African region: overview of events reported to the World Health Organization in 2018-ERRATUM. Epidemiol Infect 147: e307.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria