Prevalence of Polycystic Ovarian Syndrome (PCOS) Like Symptoms in the General Practice of an Obstetrics and Gynecological Office on the Island of Tobago: A Retrospective Chart Analysis
Introduction: Polycystic ovarian syndrome (PCOS) is one of the most common endocrinopathies found in reproductive age women. It is characterized by anovulatory infertility, menstrual dysfunction, and hirsutism. It is thought to be associated with an increased risk of metabolic aberrations, including insulin resistance, hyperinsulinism and type 2 diabetes mellitus (T2D). Due to the racial disparities associated with insulin resistance and T2D, we hypothesized that the prevalence of PCOS like symptoms would be increased on the island of Tobago where women were predominantly of Afro-Caribbean descent. Study Design: A retrospective chart review of 1000 women seen in an obstetrics and gynecological office over a 7-year period was conducted. Inclusion criteria included race, body mass index (BMI)<50, and no diagnosis of a co-morbid endocrinopathy. Of the 1000 women, 884 Afro-Caribbean women were included in the analysis. PCOS diagnosis was made based on clinical signs and symptoms verified on ultrasound. The diagnosis was considered if a patient presented with ≥2 of the following signs and symptoms: infertility after >1yr of unprotected sex; irregular menses with periods >35 d, <21 d or <6/yr; overweight/ obese (BMI>25); hirsutism; and acne. Results: Within the study population, 15.7% of participants had irregular menses, 9.2% had infertility, 4.0% had hirsutism and 0.4% developed acne. The prevalence of PCOS based on clinical diagnoses and ultrasonographic evidence was 19.7%. No statistical difference (p<0.05) was found between the two groups with regards to BMI, age and parity. When stratified by age, differences in infertility were found in the 20-24 and 35-39 year old age groups with rates at 10.5 v 18.9% and 15.4 v. 30.2%, respectively. The incidence of irregular menses also differed among age groups, with PCOS patients reporting significantly higher percentages between 30-50%. Conclusion: PCOS appears to be a common disorder on the island of Tobago with a prevalence of 19.7%. This prevalence is higher than in North American studies but is in line with data excluding biochemical analysis. As PCOS is a heterogeneous disorder with diverse phenotypes and probable ethno-genetic variations, the next step would be to further characterize the characteristics of PCOS in the Tobago population. This includes obtaining a full battery of biochemical profiles of women diagnosed with PCOS-like symptoms and the consideration of gene environment interactions including exposure to endocrine disruptors thought to be involved in the etiology of PCOS.
Introduction
Polycystic Ovarian Syndrome (PCOS) is the most common endocrinopathy found in reproductive age women. It is a genetically complex endocrine disorder whose underlying pathophysiology is thought to involve beta cell dysfunction and insulin resistance, which characterizes 50-90% of women with PCOS [1]. PCOS is a common cause of anovulatory infertility, menstrual dysfunction, and hirsutism [2, 3]. It is associated with an increased risk of metabolic aberrations, including insulin resistance and hyperinsulinism, type 2 diabetes mellitus, obesity, dyslipidemia, cardiovascular disease, and endometrial carcinoma [4, 5, 6]. The prevalence of PCOS varies with ethnicity and race, with a rate of up to 52% reported in women from the Indian subcontinent [7]. A Greek study conducted by Diamanti-Kandarakis et al. [8] reported a prevalence of 6.8%, with a Spanish study by Asuncion, et al. [9] of women of Caucasian descent reporting a similar rate of 6.5%. An American study conducted by Azziz, et al. [2] in an unselected population reported results for Caucasian and Black women at 4.8% and 8%, respectively. The current estimates therefore predict that PCOS affects between 5-10% of women [1, 2, 10] though studies from Europe have suggested prevalence rates that are 60–100% higher [2].
There has long been debate about the criteria necessary for the diagnosis of PCOS. The European definition requires
- A polycystic ovary diagnosed via ultrasound, usually according to the Adams, et al. [11] criteria,
- Menstrual disturbance: often oligo- or amenorrhea,
- And/ or signs of hyperandrogenism such as hirsutism, acne or alopecia.
It should be noted that under this system, the diagnosis of PCOS can be made via ultrasound but without any clinical symptoms is not regarded as the syndrome [12]. The North American definition established by the 1990 conference of the National Institutes of Health (NIH) recommended that the diagnostic criteria include the biochemical analysis of the following:
- Ovulatory dysfunction,
- Hyperandrogenemia and /or clinical evidence of hyperandrogenism (hirsutism, acne, and androgenic alopecia), and
- Exclusion of other related endocrinopathies [13]. The debate continues as ultrasound studies have shown approximately 21-23% of randomly selected young women have PCOS [14, 15, 16]. Previous studies have also demonstrated that PCOS on ultrasonography has been seen in 92% of women with idiopathic hirsutism and 87% of women with oligomenorrhea [17].
A recent systematic review Srnovršnik T, et al. [18] summarized the investigations of the association of endocrine-disrupting chemicals (EDCs) with PCOS. The authors conducted an electronic literature search using PubMed for studies published between January 2007 and October 2022 on EDCs related to PCOS, and evaluated the association of PCOS with bisphenols, parabens and triclosan in 15 articles. Their review revealed an association of bisphenol A (BPA) with PCOS and negative effects of BPA on human ovaries and concluded that more research is needed to assess the potential associations of parabens and triclosan with PCOS. Low half-lives (7.7-20.3 hours) have been reported for environmental phenols including three parabens, triclosan, and two benzophenones as measured in urinary concentrations which are not persistent making it quite challenging to determine long-term exposure to these chemicals [19]. However, other EDCs such as organochlorine pesticides, polychlorinated biphenyls (PCBs), and brominated flame retardants (BFRs) may be more widespread and/or have longer half-lives [20].
There have been few studies conducted on the prevalence of PCOS in non-Caucasian individuals and none conducted on the island of Tobago. The population under investigation consisted primarily of individuals of Afro-Caribbean (90%) and East Indian (10%) descent. The racial disparity in the prevalence of type 2 diabetes, with a higher incidence in people of African descent compared with Caucasians, has long been described and is often attributed to higher levels of obesity and insulin resistance [19]. It has also been shown that, compared to women of Caucasian descent, African American, Caribbean-Hispanic and South Asian women, with PCOS, tend to have higher insulin levels and higher levels of insulin resistance [21, 22]. From these findings it may be possible to extrapolate, that based on genetic disposition, the women of Tobago may have a higher prevalence of PCOS than the Caucasian women in whom many of the previous studies have been conducted.
Case Selection
Patient records were obtained from the Obstetrics and Gynecological practice of Dr. V. Wheeler on the Island of Tobago. Charts were randomly sampled. One thousand charts, in which the patients were between the ages of 18-40 at their last visit, were reviewed. Inclusion criteria for analysis of data included race, body mass index (BMI) <50 kg/m2, and no diagnosis of a co-morbid endocrinopathy. Nine patients were excluded on the basis of a co-existing endocrinopathy: hyperprolactinemia or hypo-/hyperthyroidism. Since race was not recorded on the chart it was based on a physician executed questionnaire. Based on physician recall, 90.7% were determined to be of Afro-Caribbean descent, 5.5% of Asian Indian, 3.6% of Caucasian and 0.2% were undetermined. Thirty-eight patients not of Afro-Caribbean or Asian Indian descent were excluded from the analysis. Most of these patients were thought to be Caucasian immigrants and therefore not reflective of the base demographic of the island. Six patients were excluded on the basis of BMI as their calculated values were >50 kg/m2 increasing the likelihood of a recording error.
The diagnosis of PCOS was made by consultant Dr. V. Wheeler based on clinical signs and symptoms and on ultrasound. The diagnosis was considered if a patient presented with at least two of the following signs and symptoms: infertility (>1yr of unprotected sex), oligomenorrhea or irregular menses (>35d or <21d or <6/ yr), overweight/obese hirsutism, and acne. The patient was then sent for a follow-up pelvic ultrasound. If the pelvic ultrasound showed ‘polycystic ovaries’ then the diagnosis was confirmed, and treatment was offered depending on symptoms or fertility concerns.
If, for some other reason, the patient was sent for an ultrasound and found to have polycystic ovaries but did not report any of the signs and symptoms listed above then she was not diagnosed with PCOS. Due to cost constraints, hormonal profiling, follicular stimulating hormone (FSH) and luteinizing hormone (LH), were not routinely available. It should be noted however that there are individuals who do not have polycystic ovaries on ultrasound but have abnormal FSH to LH ratios. Parity was defined as pregnancy >24 weeks.
Ultrasounds
All ultrasounds were conducted by radiographer H. Alleyne. Most of the ultrasounds were transvaginal unless the patient had never been sexually active and then an abdominal ultrasound was conducted. It was not noted which type of ultrasound was performed. Within this paper, ultrasounds are reported as either PCOS positive or PCOS negative. The patients who had the signs and symptoms of PCOS but who were diagnosed with another condition on ultrasound, such as fibroids, were considered for the purpose of this paper to have negative ultrasounds.
Due to their increased resolution transvaginal ultrasounds are currently considered the gold standard for the diagnosis of polycystic ovaries. The following table lists the accepted criteria for the diagnosis of PCOS using either transabdominal or transvaginal techniques (Table 1).
| Ultrasound | Variables | Criteria | |
|---|---|---|---|
| Adams, et al. [17] | Transabdominal | Ovarian volume | > 15 cm³ |
| Adams, et al. [17] | Transabdominal | No. of follicles 4-10 mm | > 10 |
| Atiomo, et al. [14] | Transvaginal | Ovarian volume | > 9 cm³ |
| Atiomo, et al. [14] | Transvaginal | No. of follicles 2-8 mm | > 10 |
| Atiomo, et al. [14] | Transvaginal | Increased echogenicity of ovarian stroma | Present |
Table 1: Criteria for the Diagnosis of PCOS [14].
Statistical Analysis
The results are expressed as the mean or percentage in the text and tables. One-way ANOVA followed by the least significant difference test and the student’s t-test were used to compare the means of the different groups of women. A X2 test was used for discontinuous variables. P < 0.05 was considered significant. The statistical software package used to perform the analyses was Statistical Package for the Social Sciences (SPSS for Windows, version 13.0).
Results
Of the 55 Asian Indian subjects, 53 were included in the PCOS analysis. Of these patients 32.7% were determined to have PCOS by clinical diagnosis, all of which were confirmed via ultrasound. Due to the small percentage of Asian Indian patients, the remainder of the results focuses on the Afro- Caribbean patients. Of the 907 eligible Afro-Caribbean subjects, 884 were included in the analysis. Based on the assessed characteristics, 15.7% of the population was noted to have irregular menses, 9.2% had infertility, 4.0% had hirsutism and 0.4% had developed acne. Of these patients, 176 (19.9%) were determined to have PCOS by clinician diagnosis. Of the patients diagnosed with PCOS, 174 (98.7%) were confirmed via ultrasound. The other two patients were referred for ultrasound but lost due to follow up.
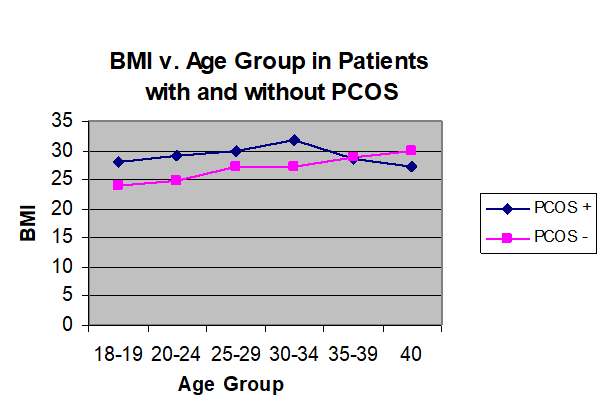
The age distributions of the patients are recorded in Table 2. Here it can be seen that the patients were concentrated in the 20-34 year age range, with the highest proportion of PCOS patients in the 20-29 year old group. The average age (Table 3) of the patients in this study with PCOS was 26.6 ± 5.6 and without PCOS was 27.96 ± 6.6 years old. The average BMI was calculated at 29.5 ± 6.4 kg/m2 for the patients with PCOS and 26.5 ± 6.0 kg/m2 for those without the diagnosis. When distributed by age in Figure 1, the women with PCOS had higher BMIs until the 35-39 age groups where the means converged. The mean parity was calculated at .53 ± 1.0 for the patients with PCOS and 1.06 ± 1.4 for patients without PCOS. There was however no statistical difference between these means with a p<0.05 for any of these variables.
| Age Group (years) | N | PCOS (N, % of Age Group) | |
|---|---|---|---|
| 18-19 | 82 | 12 | (14.6) |
| 20-24 | 255 | 63 | (24.7) |
| 25-29 | 207 | 54 | (26.1) |
| 30-34 | 163 | 23 | (14.1) |
| 35-39 | 143 | 17 | (11.9) |
| 40 | 28 | 4 | (14.3) |
| Total | 878 | 173 | (19.7) |
Table 2: Age distribution of PCOS patients1. 1Age missing for one case.
| PCOS | N | Mean | Std. Deviation | Std. Error Mean | |
|---|---|---|---|---|---|
| Age | yes | 173 | 26.62 | 5.615 | 0.427 |
| Age | no | 702 | 27.96 | 6.569 | 0.248 |
| BMI (kg/m2) | yes | 135 | 29.49 | 6.469 | 0.557 |
| BMI (kg/m2) | no | 485 | 26.50 | 6.011 | 0.273 |
| Parity | yes | 176 | 0.53 | 1.036 | 0.078 |
| Parity | no | 708 | 1.06 | 1.355 | 0.051 |
Table 3: Characteristics of Women by PCOS Status.
Approximately 88% of the patients with PCOS and 54% of the controls had at least one of the signs and symptoms indicative of PCOS (Table 4). When evaluated by age group (Table 5), rates of infertility were different between the groups with and without PCOS in the 20-24 and 35-39 year old age group at 10.5% v. 18.9% and 15.4% v. 30.2%, respectively.
There was also a difference in the 40 year old age group that was not reported as only 27 patients comprised this group. The incidence of irregular menses also differed among all age groups, with the PCOS patients reporting significantly higher percentages of between 25-51%. Only 12 charts had any reference to acne with four patients noted to have a problem.
Fifty-three charts had some mention of hirsutism with 35 patients noted to have the condition. Of these 35 patients 24, 72.7% also held a diagnosis of PCOS.
| PCOS (n=176) | Without PCOS (n=708) | Total (n=884) | |
|---|---|---|---|
| Sign and/or Symptom | n (%) | n (%) | n (%) |
| No | 22 (12.5%) | 326 (46.0%) | 348 (39.4%) |
| Yes | 154 (87.5%) | 382 (54.0%) | 536 (60.6%) |
Table 4: The Presence of One or More Sign and/or Symptom (Infertility, Irregular menses, Acne, and Hirsutism).
| PCOS | Without PCOS | |||
|---|---|---|---|---|
| Age Group | Infertility (%) | Irregular Menses (%) | Infertility (%) | Irregular Menses (%) |
| 18-19 | 0 | 41.7 | 0 | 11.9 |
| 20-24 | 10.5 | 50 | 18.9 | 11.4 |
| 25-29 | 28.6 | 51 | 28.3 | 6.7 |
| 30-34 | 37.5 | 45 | 20.8 | 6.2 |
| 35-39 | 15.4 | 31.3 | 30.2 | 8.7 |
| 40 | 50 | 25 | 1.9 | 4.2 |
Table 5: Rates of Infertility and Irregular Menses.
Discussion
Though PCOS is one of the most common endocrine disorders affecting women, there is virtually no data on its prevalence in a predominantly Afro-Caribbean population. The current estimation of the prevalence of PCOS has varied based on the diagnostic criteria applied. In many of the European based studies, the prevalence has been reported at rates upward of 20%, while using the NIH/National Institute of Child Health and Human Development (NICHD) criteria the rates have varied between 5-10%. Using the European approach, the retrospective analysis revealed an estimated cross sectional prevalence of 19.7% on the island of Tobago. This value is very close to the reports that indicate that 20- 23% of unselected women in a Caucasian population will have polycystic ovaries [14, 15, 16]. As United States (US) based studies do not include ultrasound in the diagnosis of PCOS, the number of individuals that would have been included in the presumptive diagnosis of PCOS without ultrasound but with a clinical history of hyperandrogenism and/or chronic anovulation is 14.4%. The discrepancy in the percentages was in part due to chart documentation, as the duration of symptoms were not recorded and therefore the diagnosis of infertility (>1yr of unprotected sex without conception) or oligomenorrhea (menses >35d, <21d, or <6/yr) could not be assessed. Previous studies have also demonstrated that PCOS on ultrasonography has been seen in 92% of women with idiopathic hirsutism and 87% of women with oligomenorrhea [17]. It should therefore not have been surprising, since most of our patients diagnosed with PCOS had positive ultrasounds, that 87.5% of the patients diagnosed using this method had at least one symptom of PCOS. For the other 22 patients (12.5%), it was simply noted that they had a positive diagnosis of PCOS; it was not possible to determine which signs and symptoms led to their diagnosis. It should be mentioned that the charts used in this study were of women seeking medical treatment and there is an inherent bias to our study design. The variables of acne and hirsutism were also not well recorded and should be reassessed in follow up studies.
Results indicated that while the mean rates of infertility were not significantly different between the groups, there were some obvious differences when stratified by age. Based on the previous research, it would have been predicted that the rates of infertility should increase as the patients increased in age and with the diagnosis of PCOS [2, 3]. This was only true for patients in the 30-34 year age group. The rates in the 18-19 and 25-29 year old age groups were equivocal, while those in the 20-24 and 35-39 year old age groups were opposite to the expected values. This difference may be in part explained by the fact that the majority of patients with PCOS were in the 20-34 year old age group. Based on their age, these patients may not have yet attempted to become pregnant or yet decided that they are having problems with infertility. The inability to draw any clear inferences from this data is further compounded that neither the marital status nor their desire to get pregnant was evaluated. As with infertility, the evaluation of parity (pregnancy >24 weeks), which was not significantly different between groups, was limited by the fact that marital status and reasons for possible terminations were not recorded and evaluated.
The prevalence rate of reported menstrual dysfunction in our population was 15.7%, intermediate between 14.6% in the Greek study by Diamanti-Kandarakis E et al. [8] and 19.5% in the Spanish study by Asuncion M, et al. [9]. The rates of menstrual irregularities were higher in all the age groups of patients with PCOS as compared to the rest of the population. The fact that irregular menses are common and one of the earliest symptoms reported in PCOS differentiates these results from those seen in regard to infertility.
Of the patients diagnosed with PCOS, the highest prevalence rates were found in the 25-29 year old group. This is consistent with the fact that PCOS is most often diagnosed in the early reproductive years. The convergence of the BMIs as the recorded ages increased in the 35-39 year old age group raises the question of the impact of weight in the prevalence of PCOS. In the studied population, 27.6% of subjects were overweight and 29.7% were obese. These rates were similar to those of the general female population aged ≥20 years old of Trinidad, et al. [21] which is recorded at 21.1% obesity and 32.6% overweight. The prevalence of obesity and not overweightness was higher in the women with PCOS than the rest of the population. Approximately 51% of the PCOS population versus 23.9% of the rest of the study population was obese. This was higher than the values in the American unselected study population [13] (42%), the Spanish study by Asuncion M, et al. [9] (30%), and the Greek study by Diamanti-Kandarakis E, et al. [8] (38%). Our findings suggest that there are significant ethnic differences in the prevalence of obesity in PCOS and that obesity is not necessarily a universal feature of PCOS.
Conclusion
In conclusion, we found a 19.9% prevalence of clinically diagnosed PCOS with 98.7% of those confirmed by ultrasound, as defined by the generalized European criteria, on the island of Tobago in a single obstetrics and gynecological office. This prevalence is higher than those seen in any of the North American studies but is in line with data that excludes biochemical analysis [2]. While US based studies do not include ultrasound in the diagnosis of PCOS, the number of individuals that would have been included in the presumptive diagnosis of PCOS without ultrasound but with a clinical history of hyperandrogenism and or chronic anovulation was 14.4%. As PCOS is a heterogeneous disorder with diverse phenotypes and probable ethno-genetic variations, the next step would be to assess for exposure to endocrine disruptors thought to be involved in the etiology of PCOS as well as to determine the biochemical profiles of those women diagnosed with PCOS. This could evaluate the differences in this diagnostic technique with those recommended in the 1990 NIH/NICHD conference as well as further catalogue the characteristics of PCOS on the island of Tobago.
References
-
Goodarzi (2005) β-Cell Function: A Key Pathological Determinant in Polycystic Ovary Syndrome. J Clin Endocrinol Metab 90 (1): 310-315.
-
Azziz R, Woods K, Reyna R, Key T, Timothy J, et al. (2004) The Prevalance and Features of the Polycystic Ovary Syndrome in an Unselected Population. J Clin Endocrinol Metab 89 (6): 2745-2749.
-
Azziz (2003) The evaluation and management of hirsutism. Obstet Gynecol 101: 995-1007.
-
Ovalle (2002) Insulin resistance, polycystic ovary syndrome, and type 2 diabetes mellitus. Fertil Steril 77(6): 1095-1105.
-
Talbott E, Guzick D, Clerici A, Berga S, Detre K, et al. (1995) Coronary Heart Disease Risk Factors in Women with Polycystic Ovary Syndrome. Arteriosclerosis, Thrombosis and Vascular Biology 15(7): 821-826.
-
Wild (2002) Long-term consequences of PCOS. Hum Reprod Update 8(3): 231-241.
-
Rodin DA, Bano G, Bland JM, Taylor K, Nussey SS (1998) Polycystic ovaries and associated metabolic abnormalities in Indian subcontinent Asian women. Clin Endocrinol 49(1): 91-99.
-
Diamanti-Kandarakis E, Kouli C, Bergiele A, Filandra F, Tsianateli T, et al. (1999) A Survey of the Polycystic Ovary Syndrome in the Greek Island of Lesbos: Hormonal and Metabolic Profile. J Clin Endocrinol Metab 84 (11): 4006- 4011.
-
Asuncion M, Calvo R, San Millan J, Sancho J, Avila S, et al. (2000) A Prospective Study of the Prevalence of the Polycystic Ovary Syndrome in Unselected Caucasian Women from Spain. J Clin Endocrinol Metab 86 (7): 2434-2438.
-
Gambineri (2004) Glucose Intolerance in a Large Cohort of Mediterranean Women with Polycystic Ovary Syndrome: Phenotype and Associated Factors. Diabetes 53(9): 2353-2358.
-
Adams J, Franks S, Polson DW, Mason HD, Abdulwahid N, et al. (1985) Multifollicular ovaries: clinical and endocrine features and response to pulsatile gonadotrophin releasing hormone. Lancet 2(8469-8470): 1375-1378.
-
Homburg R (2002) What is polycystic ovarian syndrome? A proposal for a consensus on the definition and diagnosis of polycystic ovarian syndrome. Human Repro 17(10): 2495-2499.
-
Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, et al. (1998) Prevalence of the Polycystic Ovary Syndrome in Unselected Black and White Women of the Southeastern United States: A Prospective Study. J Clin Endocrinol Metab 83(9): 3078-3082.
-
Lakhani K, Seifalian AM, Atiomo WU, Hardiman P (2002) Review article: Polycystic ovaries. Brit J of Radiology 75: 9-16.
-
Clayton RN, Ogden V, Hodgkinson J, Worswick L, Rodin DA, et al. (1992) How common are polycystic ovaries in normal women and what is their significance for the fertility of the population? Clin Endocrinol (Oxf) 37: 127-134.
-
Farquhar CM, Birdsall M, Manning P, Mitchell JM, France JT (1994) Prevalence of polycystic ovaries on ultrasound scanning in a population of randomly selected women. Aust NZ J Obstet Gynaecol 34: 67-72.
-
Adams J, Polson DW, Franks S (1986) Prevalence of polycystic ovaries in women with anovulation and idiopathic hirsutism. Br Med J (Clin Res Ed) 293(6543): 355-359.
-
Srnovršnik T, Virant-Klun I, Pinter B (2023) Polycystic Ovary Syndrome and Endocrine Disruptors (Bisphenols, Parabens, and Triclosan)-A Systematic Review. Life (Basel) 13(1): 138.
-
Diamanti-Kandarakis E, Bourguignon JP, Giudice LC, Hauser R, Prins GS, et al. (2009) Endocrine-disrupting chemicals: an Endocrine Society scientific statement. Endocr Rev 30(4): 293-342.
-
Nguyen HT, Isobe T, Iwai-Shimada M, Takagi M, Ueyama J, et al. (2023) Urinary concentrations and elimination half-lives of parabens, benzophenones, bisphenol and triclosan in Japanese young adults. Chemosphere 349: 140920.
-
Centers for Disease Control and Prevention (2003) Prevalence of diabetes and impaired fasting glucose in adults-United States, 1999-2000. MMWR Morb Mortal Weekly Rep 52: 833-837.
-
Ehrmann (2005) Effects of Race and Family History of Type 2 Diabetes on Metabolic Status of Women with Polycystic Ovary Syndrome. J Clin Endocrinol Metab 90(1): 66-71.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria