The Violence Risk's Management and the Competent Act of Nursing Technicians
The article aims to show the work of nursing technicians in psychiatric patient care in a crisis care unit, revealing the difficulties found and the strategies built to meet the operational needs for the development of actions of assistance, competence and the construction of workers' health. The methodological approach used was based on the Ergonomic Work´ Analysis - EWA and Ergology whose sample was composed of 17 professionals, auxiliaries and nursing technicians, from an emergency sector of a public psychiatric hospital. The results revealed structural changes with the consequent impact on care: A) Regarding the organization of the psychiatric care network, two main inferring factors were evidenced: 1) The distance between the organization of psychiatric care advocated by the Psychiatric Reform and the actual structure and organization of the system; 2) Social transformations carry significant changes in the profile of patients; B) Norms´ conflicts originated in the debates between Psychiatry and Mental Health; C) Collective settings in the daily care and skills of the nursing technician. As conclusion, it can be affirmed that the competent action of nursing technicians, anchored in teamwork, is central to the risks´ management in the analyzed context.
Introduction
This study, carried out in a psychiatric hospital, is structured in the field related to the production of knowledge for the development of ergonomic and ergological criteria aimed at the design and management of work systems in the Health Sector, involving issues related to conditions of work performance and the repercussions of working conditions on the health of working people involved in mental health care, whose space and technique are undergoing a profound structural transformation. The hospital sector has been shown to be an important and serious focus of problems related to Occupational Health and Safety [1, 2, 3, 4] and is increasingly required preventive interventions [4, 5, 6]. These repercussions of the work activity on health have been shaped in various processes of attrition and illness, among which stand out the work-related repetitive strain injury, various manifestations of psychic illness and accidents at work [6, 7]. In hospital care in psychiatry, it has been observed, especially in psychiatric emergencies, but not exclusively, an increase in the potential risk of aggression to the working populations involved [1, 2, 3, 6, 7].
Some questions stand out: Has the clinic advocated by the Centers for Psychosocial Care (CAPS) been successfully managed the patient’s diversity? Are the patients who have reached psychiatric hospitals not those who have not been assisted by the substitute network because of the complexity of care and the risk of aggression? Have involuntary hospitalization patients been hosted by the CAPS? Has the dismantling of the system not been very fast, leading to disengagement? Mental health needs have grown and become increasingly complex, requiring a permanent updating and diversification of the forms of mobilization and political articulation, management and construction of innovative strategies of care. Debates and political clashes over the Psychiatric Reform have become more recurrent, especially with corporate mental health entities, especially the medical ones, but not only them - and relevant political actors in parliament, with a new emphasis on the biomedical model, as well as a strong and explicit campaign against psychiatric reform, often taking on the aspect of litigation where the doors to dialogue have become narrow. Deinstitutionalization has continued in all municipalities where psychiatric hospitals are located - 1700 beds are closed annually [8]. Some difficulties still have to be overcome, such as the sub-financing of therapeutic residences and the slow pace of incorporation of the graduates into the Back to Home Program. It is still insufficient to offset the opening of services in general hospitals and CAPS-III, impacting on the daily care provided in other network equipment and also on the strategies of care and risk management in psychiatric hospitals that receive patients in crisis (Mostly compulsory or involuntary hospitalizations) and with direct consequences on the health of the working populations involved. The pretension of the article, in its theoretical and methodological deepening, is to understand to transform. Some issues arise from this:
- How can competent action in this context arbitrate between hetero-determination (conditions established by technical, organizational, managerial norms, instruments, time, space) and the mobilization of knowledge and values embodied in practice?
- And the unfolding of this debate as a possibility of health / illness production, pleasure / displeasure, pain / suffering / regulation, risks / knowledge of prudence, at work?
• Faced with the questions raised, another, even more specific, emerges: how can this population of nursing assistants and technicians manage to "set themselves up" collectively and produce knowledge to deal with (unpredictable and risky) patients who have accessed the hospital under study? Analyzing risk management at work and the construction of health / disease implies access to the singularity of individual and collective experiences of recognition and hierarchy of risks in the face of the specificities of productive situations. The objective of the study, therefore, is to understand the work activities of nursing technicians in patient care in a psychiatric emergency, revealing the difficulties encountered and the strategies built to account for operational needs for the development of care, Workers' health, associated with the purposes of production.
Nursing in the Hospital Context and Mental Health
Nursing is a historically structured practice, constituted by different caring ways that are determined by the social relations of each historical moment [9, 10, 11]. Currently, nursing work is integrant to collective work in health, is specialized, divided and hierarchized among auxiliaries, technicians and nurses according to the complexity of conception and execution. Although nursing has relative autonomy in relation to other professionals, nursing is subordinated to the management of the health care act performed by physicians [4, 10, 11, 12, 13, 14]. The work process of health professionals aims at the therapeutic action of health and as object the individual or groups that are ill, healthy or exposed to risk, that demands curative measures, in order to preserve health or prevent disease and, as Instrumental work, instruments and conduits that represent the technical and practical level of knowledge, which is health knowledge. The final product is the provision of health care that is produced at the same time as it is consumed, characteristic of the service sector [9, 10, 11, 14, 15]. There is, in the literature, a shortage of studies that address the health of the nursing worker who works in psychiatric care. Among the national studies, most of them portray specific situations, such as dealing with suicide and the permanent state of alertness in the work routine that can compromise the mental health of the worker [12, 13, 16, 17].
The present moment of nursing work in mental health is characterized by the transition between a hospital care practice, aimed at containing the behavior of the "mentally ill", to incorporate new and unknown principles, an interdisciplinary practice, open to the contingencies of Subjects involved in each moment and in each context, overcoming the disciplinary perspective of their actions, from the psychiatric reform [10, 12, 18]. Since then, the actors in this process are not only the technicians belonging to the mental health teams, but also the family members and the community. The space for discussion about madness goes beyond the walls of hospices and occupies cities, institutions and the lives of citizens [19]. The profile of the mentally ill has changed, as a result of the deinstitutionalization and the greater exposure of the population to drugs and alcohol. The finding that the use of these substances has taken on the proportion of a serious public health problem in the country has resonance in the various segments of society, by the proven relationship between consumption and the social problems that result from or reinforce it. Addressing this problem is a global demand: according to the World Health Organization, at least 10% of the population in urban centers worldwide consumes harmful substances, regardless of age, sex, purchasing power [19]. Except for variations without significant epidemiological repercussions, this reality finds equivalence in Brazilian territory [9, 18]. In particular, drug´s use imposes on Brazil and the societies of all countries a global burden of undesirable and extremely costly diseases that afflict individuals in all areas of their lives. The magnitude and complexity of the epidemiological picture recommends a wide range of policy responses to coping with problems arising from consumption. In Brazil, the use of alcohol and other drugs has historically been associated with crime and antisocial practices and the offer of "treatments" inspired by exclusion / separation models of social interaction users [9, 19]. Government initiatives were restricted to few outpatient or hospital services, generally linked to university programs, as there was no national policy in the area of public health [20]. In 2002, the Health Ministry has began implementing the National Program of Integrated Community Care for Alcohol and Other Drug Users, recognizing the problem of harmful use of substances as an important public health problem and constructing a specific public policy to care for people who Use of alcohol or other drugs in the field of mental health, with a strategy of increasing access to treatment, full and dynamic understanding of the problem, promotion of rights and harm reduction approach [19, 20]. In practice it is noticed the change in the profile of the mental patient occurred in the last decade. As spoken by a nursing technician: "Working with psychiatric people is very difficult, we have to have a lot of patience and mine has already been exhausted for a long time. Here is a mix of everything: psychiatric patients, drug users, drug traffickers" [9]. This reality has been built, historically based, on how the individual with mental problems is being cared for by society, being excluded and reclusive [15]. This has repercussions until the present day, implying on the workers that assume the responsibility of the care [9].
Methodology
The methodological approach used in this study was based on the Ergonomic Work Analysis - EWA [21] and ergological [22]. This is a qualitative descriptive method of action of ergonomics and ergology with methodology and relevant analysis tools to identify relevant technical and organizational factors implied on the fields of health management opportunities at work in hospital productive contexts and generate together with the plaintiffs, proposals for preventive adequacy of current hospital production systems.
Materials Used and Procedures
The sample was composed of 17 professionals, nursing assistants and technicians, at an emergency department of a public psychiatric hospital, in Brazil. They were used in this study equipment to collect and record the information observed in the field. Recordings were made on each subject search separately using a digital recorder with the intention of facilitating the work of synthesis. The cut required for the methodological deepening was made in the Customer Crisis Center (CCC), through observation and interview in self-confrontation with the assistants and nursing technicians in this sector. The methodological procedures of this study were approved by the Ethics´ Committees in Research of the participating institutions and are in accordance with resolution 466/2012.
Results
Analysis of Technical and Organizational Structure
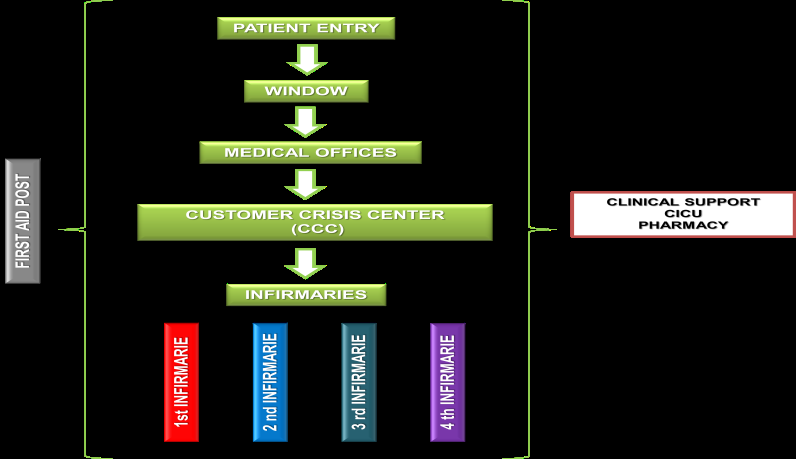
The institutional design is organized according to guidelines advocated by the Psychiatric Reform - the provision of specific clinical services for the adult in crisis. The hospital assumes the role of patient care in high complexity, which is most often brought in crisis, involuntary hospitalization or voluntary, is momentary (suffering due to dysfunctional use of drugs) and with imminent risk of flight in The reason for the abstinence crisis. This ongoing clinical reorganization in the service is based on the observation of the flow of demand, considering the moment of arrival, permanence and exit of the users. The emergency department of this hospital unit (CCC) is composed of mental health care, psychiatric care and systematized nursing evaluation. The CCC occupies a central position in this institution and the "locus", important and necessary for the management of beds and the risk of violence in the studied hospital. The role of the CCC in the hospital's organizational structure through the various mosaics compartmentalized fiefdoms - various professional groups - is to receive patients in crisis, assess, treat, refer to the wards (where applicable also demand greater permanence) and link to substitutive services of the mental health network, after rising. When indicated the continuity of patient care after a stay in the CCC, there is the hospital wards. Four, with the 1st and 2nd wards (female) - with 21 beds each and the 3rd and 4th wards (male) - with 30 beds each. There is also the Clinical Intermediate Care Unit (CICU), with six beds - suitable for the stay of patients with clinical instability. The beds of CICU are rear when used retain the position of the ward. At the hospital there, so, six beds in the CCC, 42 in women's wards, six male and six in the CICU, a total of 108 beds. Patient flow, according to the organizational structure depicted in Figure 1, with the necessary patient's stay in crisis (the CCC) for the stabilization of the clinical picture is of utmost importance, and the strategic sector for the management of beds, risks the patient himself and others and to conduct the clinic to be established. However, an increasing demand of compulsory admissions in this hospital was observed and, as a result, the beds and risk management strategies have been committed.
• Regarding the organization of the psychiatric care network, two main inferring factors were evidenced: (1) The distance between the organization of psychiatric care advocated by the Psychiatric Reform and the actual structure and organization of the system. According to the Psychiatric Reform, the role of hospitals depends on the efficiency of a less complex network of care, substitute services, public and municipal, whose responsibilities involve the reception and care of people with severe and persistent mental disorders, aiming at preserving the Ties of the patient in its territory.
Norms, instruments and knowledge, conflicts in the fulfillment of the objectives of the psychiatric reform and, as a result, the use of the model to which it is intended to overcome. Initiatives in the construction of a psychosocial care network were observed in the technical-assistance field, however, data on the quality of services provided, real working conditions both in terms of human and material resources, and possibilities Of the various network equipment . Associated with this, there are also discrepancies regarding the assembly of the health care network of the municipalities - some have progressed visibly more than others and there are still a considerable number of beds in psychiatric hospitals. In the theoretical-assistance field, there is an increase in the volume of publications, in the 1990s, full of optimism. These publications, mostly compilations of essays and reports of experiences, have brought the concepts and discussions about Italian Democratic Psychiatry, in which the models of Psychosocial Rehabilitation and Some studies have already revealed the work situations in the network substitution services [23, 24, 25, 26], the experiences developed, the transformations and difficulties encountered. One question that emerges in this study is whether the working conditions in the Caps would be better than those established in psychiatric hospitals. There is still a lack of studies on the interlocution of the various equipment of the mental health network. Deinstitutionalization are proposed, replacing the model of Traditional Psychiatry. These assumptions have also contributed actively to the consolidation of legal-political transformations, although they have not yet been properly incorporated into the professional training of doctors. In this field, it is observed the clash and debate of the clinics advocated by traditional psychiatry and mental health, in which there are also some similarities, especially in the care given to the patient said to be "difficult", of compulsory or involuntary hospitalization and, in crisis. Medication use has been high in both models (intensive use of medicalization as a control) and the physician has assumed the role of the prescriber and has often been isolated in the system. In the juridical-political field, one can see some achievements, such as Law 10216 [8], which provides for the rights of people with mental disorders, besides directives that propose guidelines for the structuring of care and the institutionalization of new models The network of care and services.
This instrumental gap, arising from the structuring and configuration process of the mental health network (in the process of construction) has a direct impact on the day-to-day care and composes the elements of decision making in the hospital under study. (2) Social transformations carry significant changes in the profile of patients, where 'drug addicts' today make up 65% of the demand of the hospital being investigated. Patients who access the service are, for the most part, patients who are said to be "difficult" by other institutions and therefore not linked to other services. Most of the entries are involuntary and patient in crisis, which substantially increases the various risks at the door, especially physical and psychic violence. Violence is established from the cultural question that surrounds the psychiatric patient and that surrounds all the social entanglement, bringing consequences on the vision one has of this population. The psychiatric patient is stigmatized, treated as a criminal or vagabond, which encompasses the drug user and the resulting social exclusion. The violence itself regarding hospitalization is justified as a response demanded by the State to Psychiatry and legitimized by the relatives. Violence is established by referring to an end that lies in the future: a therapeutic perspective that aims at the "good" of the subject or that aims at social harmonization. Most of the time, psychiatrists are under pressure (state - justice / police, society, family) to internalize their patients.
- Regarding the conflict of norms originated in the debates between Psychiatry and Mental Health - different disciplinary fields that support the practices of care and its instrumentality, the following factors can be highlighted: (1) As a result of the Psychiatric Reform, new forms (prescriptions) of work in the field of Mental Health were created, imposed on the workers, very often, abruptly, which did not allow a field of maneuver in the management of work. However, there were also situations where the prescriptions were laid loosely, in which the old one was allowed to be reproduced in the new, where the established relations of know-how were not moved - the wall of the asylum that was in the territory was deconstructed , But not what was rooted in culture. Mental Health has brought with it its clinic, the need to overcome the value attributed to the hospital- centered model, the scientific debate regarding the evidence and value of the results of work undertaken on psychosocial rehabilitation and harm reduction and the importance of Consolidation of interdisciplinary and intersectoral work, and, of course, the training of human resources for work in the area. Psychiatry, in turn, brings with it a counter-reform movement in which it questions the proposal of the deinstitutionalization and extinction of psychiatric hospitals and defends its own reform, through the humanization of care and greater articulation with the care network. The Brazilian Association of Psychiatry (BAP) advocates a comprehensive care proposal based on detoxification, abstinence maintenance and relapse prevention in which the psychiatric hospital is an integral part of the care network. The debates and clashes make up the norms and values that permeate mental health work and cross the activity, impacting on the dimensions of care, both in the hospital and in the CAPS. (2) The prevalence of entry of patients with involuntary or voluntary hospitalization momentary reinforces the approach used in the face of potential risk. As a strategy in view of the imminent risk, the psychiatrist's classification of risk at entry is associated with the Individual Therapeutic Plan (ITP). This classification reveals a potential risk of self-extermination, escape, fissure, robbery, aggression, sexual activity and pyromania that directs the necessary practices in the CCC and in the wards and, in a way, guides the instrumentality necessary for the assistance.
- Regarding the collective configurations in the daily care and the skills of the nursing technician: Specifically in CCC, the instrumentality of nursing technicians required for care is effective in the interaction of the various technologies that configure a certain sense in the way of producing care. Acting against the unpredictability of psychiatric care requires historicity, competence in dealing with the patient - imminent potential for risk of aggression. From the structural point of view, CCC works differently from morning to night. In the morning, there is a collective configuration necessary to manage patients' output according to the number of local beds and the availability of beds in the wards: it is anticipated due to the greater demand for patients to enter the area in the afternoon. As revealed in the micro-stories of the activity in the CCC: "today is ugly! We're going to be packed all day at the CCC and there are no vacancies in the wards. If they do, we'll all have to find a way". (Nursing Technician 3 - CCC).
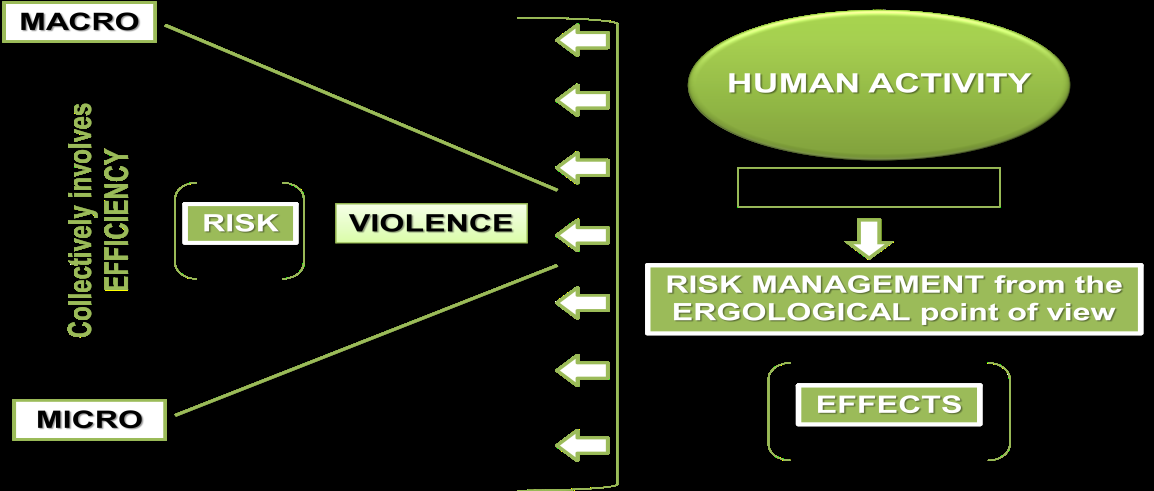
Outpatient discussion occurs routinely in the morning and the technicians occupy a fundamental role in the transfer of (in) / evolution information from the patients. The sequence of medical records established for the medical evaluation is not done randomly: the positioning of the charts from top to bottom is due to the prior evaluation of the technicians regarding the possibility of discharge. And always when picking up the medical record, a dialogue and a confrontation of competencies for decision making is established with the doctor. The nursing team brings up the day-to-day experience with the patient, the use and the medication response, the general condition of the patient. There is a position on the conduct to be established that is heard by the physician. After this listening, the doctor evaluates the patient and positions himself. The phrase is common: "It is my opinion, but you know what you do!" The knowledge / power is of the doctor and to him it is the final answer! Psychiatrists follow this routine, as do residents 2 and 3. Residents 1 (beginners) initially do not participate in the collective discussion. After a longer stay in the context they perceive the importance of knowledge sharing. This competent, strategic act for patients to leave, according to the technicians, is important to accelerate patient discharge and, in a way, regulate the workload. In the afternoon there is a demand for admission which causes a collective to be set up to decide the care path of the patient in the institution: entry and care; Care, medication and discharge - with substitutive network referencing; Care, medication and stay in the CCC. Due to changes in the profile of the patients that enter into the analyzed context and the risk characteristics of the assistance, it was necessary for the work group to structure new practices and competences in view of the specificity of the "care" to the drug user. In the collective configuration of the work, the skills of explicitation, intervention and evaluation of the technicians associated to the skills of the specialized technical team are resources of fundamental importance for the evaluation of the risk of violence and the definition of strategies to approach the imminent risk. The Figure 2, below, illustrates the human activity (activity), in the context of the study, mediated by a set of antecedent norms that cross and impact daily care. There is a necessary coherence between the individual and the environment, between the individual and social life. The matrix of human activity is the body of a subject, but an incarnate subject, impregnated with general and local knowledge and values that will direct his action. This subjectivity influences the choices made through the activity and determines the relationship with others and with the world in which one wants to live.
booked three vacancies there (infirmary). "Not understanding the situation said, that is, we interned the patient there and I observe the patient in the CCC, I was forced to ask the technician: how they interned the patient in the ward and he is here? I did not understand! Raul verbalizes: the question is this: "by the time it was crowded here we had to open space! The patient who showed signs of hospitalization was Gustavo. However, we could not send him to the infirmary because the way he is would be sexually abused or assaulted. What we did then was send him to the UCCI and, while it was crowded here, we kept him there! It caused a huge uproar there as well. As soon as we emptied it we brought it back to the CCC because of the greater control. As soon as his condition improves and the risk decreases he will be referred to the nursery. The excerpt exposes the conflicts of norms existing in the work situation of the study. Although there are a set of rules and procedures to follow, there is at the same time an absence of fundamental norms to mark the action established there. The subject / collective establishes a dramatic permeated of all the elements that make up the antecedent norm of that context, as: the rules, procedures and working instruments; The technical knowledge and those of the experiences at that moment demanded and the values circulating in the environment. Managing the beds presents itself as an art. However, it is not just about allocating patients between sectors. It is not a quantitative and operational change only. There is a set of necessary shared values that will influence the quality of care and the risks to the patient, other patients, and the working population of that and other sectors.
The absence of norms is presented in the context of an ongoing process and there is an immediate need to bring about the activity, as presented here, in order to demonstrate human action at work that, in the face of all the constraints of that context, still produces safety, quality in care and health. The nursing technician, as a member of the team who stays with the patient for the longest time, occupies a fundamental role in the evaluation of the evolution, the possible side effects of the medication and the risk of violent reactions on the part of the patient, besides participating as co-manager of the Medical / patient interfaces.
Discussion
The categorization of hospital organizations as complex systems extends to psychiatric hospitals [12, 28, 29, 30], where network information flows and collective work configuration are conditions for system efficiency [18, 31], which is structured by subjects (desires, needs and interests), work processes (knowledge and instruments), power (ways of establishing relationships) and public policies [12, 18, 32]. According to the manager of the institution, "the CCC is fundamental for making emergency care and assessing the possibility of hospitalization and / or attachment of patients to substitutive services after the crisis period". According to the same manager, to work in the CCC requires an expertise or a body of historical knowledge to deal with the inherent risk of the activity in that context. As stated: "Without CCC and risk-taking at the door, the number and severity of the assault would increase absurdly in the nurseries." This statement is in line with the notion of risk [33, 34, 35], since it is retained between two types of observation: "on the one hand, a hypertrophy of safety standards defined before the activity; On the other hand, the prudential know-how that is almost clandestine in the course of activities. " According to Echternacht [36], "work is to be managed in a medium circumscribed by technical, organizational, managerial norms, among productive structures that determine the objectives of human labor, its instruments, its time, your space". However, such levels of hetero-determination do not exclude human activity in its mobilization of knowledge and values embodied in practices, a condition for acting in competence. Ergology, based on the ergonomic assumption that the actual work is different from what is prescribed, adds that it is not only impossible but impossible to reproduce norms entirely [37]. In order to manage the variabilities, one must make "use of oneself, one's own capacities, one's own resources and choices", which is a "dramatic use of oneself". According to Schwartz and Durrive, "to work is to take risks, to make 'use of oneself'" [37]. At work, there is a continuous debate between the norms that are antecedents - relatively stabilized and protocolic knowledge and knowledge of the workers' experience - and the internal norms. From this debate of norms, choices are made, not always conscious, supported by values. Renormalization occurs when there is a rupture between the values that permeate the organization and, consequently, the antecedent norm and the values of the workers. According to Cunha [38], "even obeying the previous norms is already practicing choices. And by operating in the interstices of antecedent norms, man makes history. “Such choices determine "the relationship with others or the world in which you want to live" [37]. If, on the one hand, work is always a process of singularisation and re-singularization, on the other, the choices are always crossed by the collective dimension, an entity whose variable contours spontaneously constitute themselves "in relation to or in relation to the prescribed organization" [37]. If in the activity there is a wealth melting pot consisting mainly of prudence skills and know-how, renormalization is a process of invention of localized solutions and then consolidated and transmitted for effectiveness and health [33]. It is in this sense that human activities are the place of engagement of those who are its authors. For Echternacht [36], to arbitrate between "self-use and self-use by others" implies renormalization, in which the antecedent norms will be re-interpreted in order to readjust them to oneself and to the situation gift. In this context, changes in the profile of patients require the re-configuration of practices and competencies [12, 34, 35, 39] regarding the specificity of psychiatric care for drug users, where violence is commonly reported [40, 41]. As the worker acquires experience, he also develops individual and collective strategies for the management of everyday work situations; familiarity [42] gradual process of approaching work by building a knowledge that allows anticipating and managing the Variability of the clinic and, in a way, favor the control of the risk of violence and suffering.
The worker has the power to organize and fulfill the tasks of the clinic with relative autonomy tends to favor the development of regulatory strategies, even if the action is about an object in which one does not have much control. Familiarity with the situation contributed to the control and reduction of initial suffering, but at the cost of the trivialization of one's own suffering - situations over which the power to interfere was restricted or non-existent and the worker obliged to endure, tolerate and submit unsatisfactory working conditions. As verbalized by a CCC nursing technician, regarding the importance of the collective and the necessary experience to establish the clinic in that sector: They add up, they add up a lot. And when it is necessary to come employee of other units to act in the CCC for lack of professional, because something happened, had to leave, had to go to the doctor, you feel drastically the service getting more complicated. Because the person has no experience, there is not! It is not that they do not have dynamism, but it is that the dynamism of CCC is different. You already know this, the patient has arrived, one already starts to check vital signs, and another already directs him to the bath. This one that leads to the bath already goes taking his belongings and separating; another is already making his admission to the computer. It has to be something like that, agile! Because if you nurse get to do everything by yourself and another patient, what's up? There you will be tumultuous; you cannot let him upset the service (Nursing Technician 4 - CCC). The construction of skills and their updating is a fundamental need for risk management of violence in this context. The possible solutions to local dysfunctions and the risk of violence are not an increase in regulation and local protection measures (often necessary for certain types of risk), but in the definition of organizational forms that emerge the management capacity of the protagonists of the Work in the course of the activity.
Conclusion
At the CCC, and consequently the analyzed hospital, was observed on one hand, hypertrophy standards, including security defined activity and, secondly, know- how constructed and introduced almost in hiding in the course of activities: the offense It was placed there as a necessary condition for the production know-how of prudence, useful for effectiveness and health. The instrumentality used in dimensions of care established in the CCC, reinforces the approach on the potential risk. The expansion of the risk management ability of fields depends on the organizational conditions for upgrading the skills of the collective where nursing technicians occupy key role. Therefore, the appreciation of the work of these technicians, which involves the adaptation of effective, stability bonds, equity of workload and Technicians set the compensation procedures are essential. The working population analyzed in the study is neither a victim nor a malpractice of the system, that is, the established action was regulated within a possible horizon. In a need to permanently seek to renormalize productive 'constraints', due to this pressure on values, it redesigned the way of working and therefore also partly the nature of risks: without disconnecting from professional risks, it renewed its contours. The study does not pretend to bring elements to promote counter-reform. On the contrary, it is aimed at analyzing the activity of revealing the conflicts of norms that permeate the action of each of these "social authors" in these debates of society - crossed by the macroscopic and microscopic levels of social life - from the most local to the most general level Of living together. In this discussion of norms, local and general, values take form and meaning and, thus, direct care practices. The results presented here need to be confronted with other research carried out in the various mental health network equipment and focusing on other professionals, such as the physician, for example. The field work had as a perspective to understand to try to transform - both the assistance and the risk profile that this population is exposed through the confrontation of the specialist knowledge and the immanent of the activity (invested by those who work and updated in the day to day of work).
Conflict of Interest
The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.
References
-
Anderson L, Fitz Gerald M, Luck L (2010) An integrative literature review of interventions to reduce violence against emergency department nurses. J Clin Nurs 19(17-18): 2520-2530.
-
Chapman R, Styles I, Perry L, Combs S (2010) Examining the characteristics of workplace violence in one non-tertiary setting. Journal of Clinical Nursing 19(3-4): 479-488.
-
Unsal Atan S, Baysan Arabaci L, Sirin A, Isler A, Donmez S, et al. (2013) Violence experienced by nurses at six university hospitals in Turkey. J Psychiatr Ment Health Nurs 20(10): 882-889.
-
Freimann T, Paasuke M, Merisalu E (2016) Work- related psychosocial factors and mental health problems associated with musculoskeletal pain in nurses: a cross-sectional study. Pain Res Manag 2016: 9361016.
-
Keser özcan N, Bilgin H (2011) Violence towards healthcare workers in Turkey: a systematic review. Turkiye Klinikleri Jounal of Medical Science 31: 1442-1456.
-
Fornés J, Cardoso M, Castelló JM, Gili M (2011) Psychological harassment in the nursing workplace: an observational study. Archives of Psychiatric Nursing 25(3): 185-194.
-
Peek-Asa C, Casteel C, Allareddy V, Nocera M, Goldmacher S, et al. (2009) Workplace violence prevention programs in psychiatric units and facilities. Archives of Psychiatric Nursing 23(2): 166-176.
-
Brasil Casa Civil (2001) Dispõe sobre a proteção e os direitos das pessoas portadoras de transtornos mentais e redireciona o modelo assistencial em saúde mental.
-
Mendes D (2008) Um olhar sobre a atividade de trabalho de auxiliares e técnicos de enfermagem de uma instituição psiquiátrica: em busca de transformações. Anais do XV Congresso Brasileiro de Ergonomia, Porto Seguro, Bahia.
-
Oliveira A, Alessi N (2003) Mental health nursing work: contradictions and current potentialities. Latin American Journal of Nursing 11(3): 333-340.
-
Cho SH, Park M, Jeon SH, Chang HE, Hong HJ (2014) Average hospital length of stay, nurses work demands, and their health and job outcomes. J Nurs Scholarsh 46(3): 199-206.
-
Vasconcelos SC, Lopes de Souza S, Botelho Sougey E, de Oliveira Ribeiro EC, Costa do Nascimento JJ, et al. (2016) Nursing Staff Members Mental’s Health and Factors Associated with the Work Process: An Integrative Review. Clin Pract Epidemiol Ment Health 12: 167-176.
-
Sun S, Gerberich SG, Ryan AD (2017) The relationship between shift work and violence against nurses: a case control study. Workplace Health & Safety 1.
-
Arnetz JE, Hamblin L, Russell J, Upfal MJ, Luborsky M, et al. (2017) Preventing Patient-to-Worker Violence in Hospitals: Outcome of a Randomized Controlled Intervention. Journal of occupational and environmental medicine 59(1): 18-27.
-
Chang MJ, Chang YJ, Kuo SH, Yang YH, Chou FH (2010) Relationships between critical thinking ability and nursing competence in clinical nurses. Journal of Clinical Nursing 20(21-22): 3224-3232.
-
Fernandes JD, Ferreira SL, Albergaria AK, Conceicao FM (2002) Saúde mental e trabalho feminino: imagens e representações de enfermeiras. Revista Latino-americana de Enfermagem 10(2): 199-206.
-
Carvalho MB, Felli VEA (2006) O trabalho de enfermagem psiquiátrica e os problemas de saúde dos trabalhadores. Revista Latino-americana de Enfermagem 14(1): 61-69.
-
Mendes D (2014) O agir competente como estratégia de gestão do risco de violência no trabalho: o ponto de vista da atividade humana do trabalho dos técnicos de enfermagem de uma instituição pública psiquiátrica. Tese (Doutorado) – Universidade Federal de Minas Gerais; Belo Horizonte.
-
Abou-YD MN (2002) Hospitais psiquiátricos: saídas para o fim. Seminário FHEMIG.
-
Brasil (2005) Ministério da Saúde. Secretaria de Atenção à Saúde. DAPE. Coordenação Geral de Saúde Mental. Reforma psiquiátrica e política de saúde mental no Brasil. OPAS.
-
Guérin F (2005) Compreender o trabalho para transformá-lo: a prática da ergonomia. São Paulo: USP, Fundação Vanzolini, Edgard Blücher.
-
Schwartz YA (2000) comunidade científica ampliada e o regime de produção de saberes. Revista Trabalho e Educação 7(7): 38-46.
-
Sznelwar S (2008) Análise Ergonômica do Trabalho: ação ergonômica. In: Lancman S (Eds.), Políticas públicas e processos de trabalho em saúde mental. Paralelo 15, Brasília.
-
Silva ER (2010) A atividade de trabalho do psiquiatra no CAPS - Centro de Atenção Psicossocial: pois é José... Dissertação (Mestrado em Psicologia), Universidade Federal de Minas Gerais.
-
Ramminger T, Brito JC (2011) Cada Caps é um Caps: uma coanálise dos recursos, meios e normas presentes nas atividades dos trabalhadores de Saúde Mental. Psicologia & Sociedade 23(S1): 150- 160.
-
Almeida DT (2012) Análise do trabalho de uma equipe multiprofissional em um centro psicossocial álcool e drogas [manuscrito]. Dissertação (mestrado em Engenharia de Produção) - DEP/Universidade Federal de Minas Gerais pp: 207.
-
Merhy E, Cecílio L, Nogueira R (1992) Por um modelo tecnoassistencial da política de saúde em defesa da vida: contribuição para as Conferências de Saúde. Conferência Nacional de Saúde, Descentralizando e Democratizando o Conhecimento pp: 91-96.
-
Pavard B (2000) Apport des théories de La complesité à l’étude des systèmes coopératifs. In: Benchekroun TH, Weill-Fassina A (Eds.), Le travail collectif: Perspectives actuelles en ergonomie Toulouse, France: Octarès Éditions pp: 19-34.
-
Benchekroun TH (2000) Les espaces de coopération proxémique. In: Benchekroun TH, Weill Fassina A (Eds.), Le travail collectif: Perspectives actuelles en ergonomie. Toulouse, France: Octarès Éditions pp: 19-34.
-
Gomes JO, Vidal MC, Benchekroun TH (2000) A terceirização em um hospital de grande porte sob a ótica da Ergonomia de sistemas complexos: contribuições teóricas e metodológicas para uma macroergonomia situada de organizações em rede. Ação Ergonômica 1(1): 11-36.
-
Grosjean M, Lacoste M (1999) Comunication et intelligence collective: Le travail à L’hôpital. Paris, PUF pp: 225.
-
Barros M, Mori M, Bastos S (2007) O desafio da humanização dos/nos processos de trabalho em saúde: o dispositivo “Programa de Formação em Saúde e Trabalho/PFST”. In: Santos-Filho S, Barros M (Eds.), Trabalhador da saúde: muito prazer! Protagonismos dos trabalhadores na gestão do trabalho em saúde. Ijuí. Editora Unijuí.
-
NOUROUDINE, A (2004) Risco e atividades humanas: acerca da possível positividade aí presente. In: Figueiredo M, Athayde M, Brito J, Alvarez D (Eds.), Labirintos do trabalho: interrogações e olhares sobre o trabalho vivo. Rio de Janeiro, DP&A.
-
Loro MM, Zeitoune RCG (2017) Collective strategy for facing occupational risks of a nursing team. Rev. esc. enferm. USP 51: e03205.
-
Martinez AJS (2016) Managing workplace violence with evidence-based interventions: a literature review. J Psychosoc Nurs Ment Health Serv 54(9): 31-36.
-
Echternacht E (2008) Atividade humana e gestão da saúde no trabalho: elementos para reflexão a partir da abordagem ergológica. Laboreal 4(1): 46-55.
-
Schwartz Y, Durrive L (2010) Trabalho e Ergologia: conversas sobre atividade humana.1st (Edn.), EdUFF, Niterói.
-
Cunha DM (2007) Notas conceituais sobre atividade e corpo-si na abordagem ergológica do trabalho. In: Reunião anual da ANPED, Caxambu. Anped: 30 anos de pesquisa e compromisso social.
-
Rogalski J, Rabardel P, Janin R (2001) L’identification des dimensions des changements de technologie, d’organisation du travail et d’évolution des compétences. In: Leplat J, Montmollin M (Eds.), Les compétences en ergonomie Toulouse, Octarès Éditions, France, pp: 95-100.
-
Goetsch D (2007) Occupational Safety and Health for Technologists, Engineers, and Managers. Prentice Hall.
-
Bourrier M, Bieder C (2013) Trapping Safety into Rules. How Desirable or Avoidable is Proceduralization? Ashgate Publishing Limited, Farnhan pp: 30.
-
Sato LA (1993) Representação social do trabalho penoso. In: Spink MJP (Eds.), O conhecimento no cotidiano: as representações sociais na perspectiva da psicologia social. Brasiliense, São Paulo pp: 188- 211.
- The Expanding Landscape of Road Rage: A Systematic Review of Conflicts Involving Drivers, Pedestrians, and Micromobility
- Validating Cognitive Models of Royal Navy Performance on Control Systems
- Comparing Standard and State-of-the-art Firefighter Coats on Postural Balance and Gait in a Live Burn Environment
- Investigating the Integration of Telemedicine into Clinicians Workflow: A Review of Methods
- Risk Assessment of Ergonomic Factors in a Textile Firm by RULA, REBA and Fine Kinney Methods
- Impact of Self-Esteem Training on Individuals with Disabilities Aged 17-30