Most Ignored ECG Lead, aVR can be Lifesaver! “Short of Breath in Seattle!”
As if to rhyme with the famous Hollywood movie titled, 'Sleepless in Seattle', I saw a 64-year old man in my office in cardiac consultation who after having dinner with his son and daughter-in-law in Seattle was extremely short of breath while walking up a few stairs to his hotel room. He is from upstate New York area and was visiting them in Seattle. He never had any symptoms like this before. He did have some chest discomfort at the time but the shortness of breath was quite concerning to him. He did not have palpitations, dizziness, diaphoresis or syncope.
Introduction
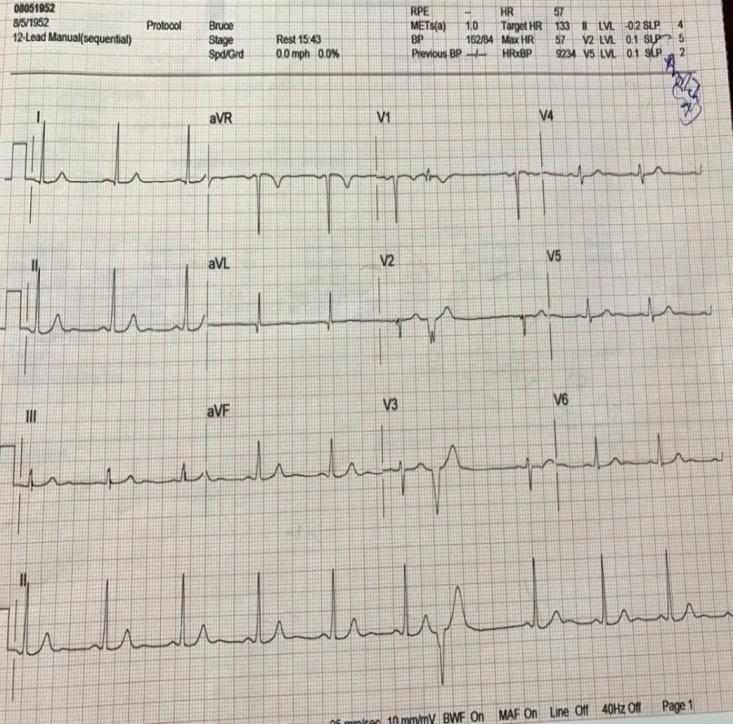
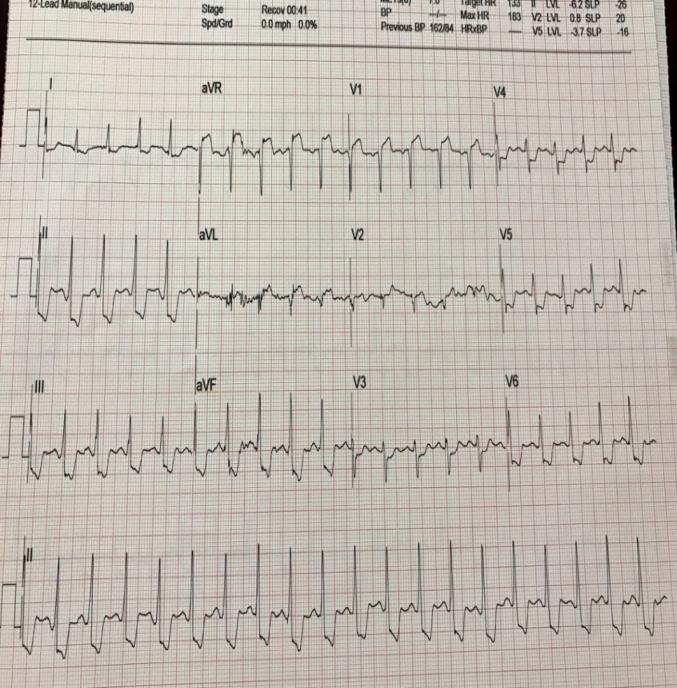
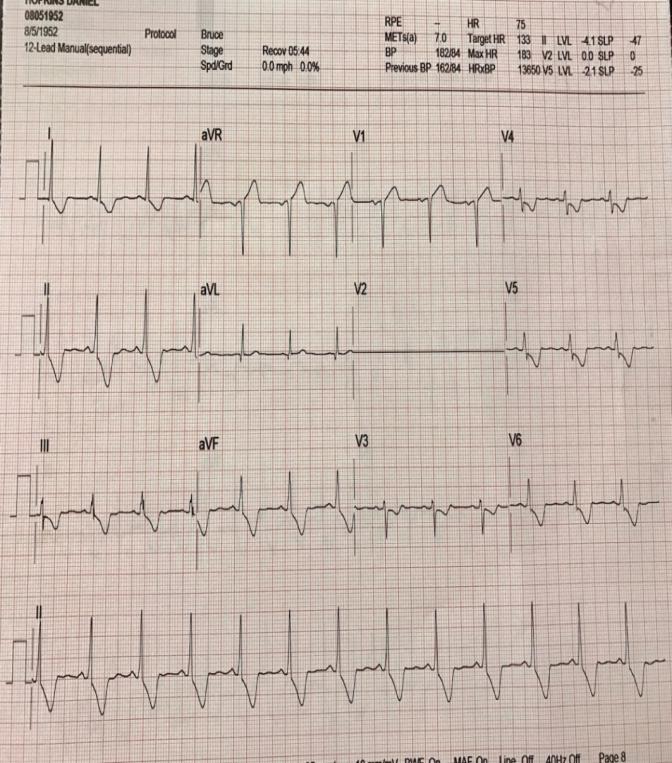
As if to rhyme with the famous Hollywood movie titled, 'Sleepless in Seattle', I saw a 64-year old man in my office in cardiac consultation who after having dinner with his son and daughter-in-law in Seattle was extremely short of breath while walking up a few stairs to his hotel room. He is from upstate New York area and was visiting them in Seattle. He never had any symptoms like this before. He did have some chest discomfort at the time but the shortness of breath was quite concerning to him. He did not have palpitations, dizziness, diaphoresis or syncope. He did not seek any medical help in Seattle and made an appointment to visit his primary care physician upon return to Upstate, NY. He was then requested to come and see me the next day. This event of shortness of breath in Seattle took place a month before coming to see me. He did not have any known history of cardiac events. No known history of coronary artery disease (CAD), myocardial infarction (MI), congestive heart failure (CHF), cerebrovascular events (CVA) or atrial fibrillation. He did not have any history of hypertension, tobacco smoking, diabetes, dyslipidemia or known family history of premature CAD. He was diagnosed with prostate cancer 15 years ago and was treated then. His baseline 12-lead electrocardiography (ECG) was normal (Figure 1) except a few PVCs (premature ventricular contractions) seen, asymptomatic. After initial evaluation and vital check-ups, he underwent a stress echocardiography in the office. Total exercise duration was only 4 minutes. After being on the treadmill for 2 minutes, he started to notice being short of breath and the Opinion Article test was stopped at 4 minutes due to extreme dyspnea. He had started to manifest markedly abnormal ECG changes on the treadmill after 2 minutes and the changes continued to get worse for another few minutes. Abnormal ST changes included: about 8 mm down sloping ST depression in inferior leads and 6 mm down sloping ST depression in leads V4-6 (Figure 2). There was 4 mm ST elevation in aVR and 3 mm ST elevation in lead V1. These ST changes lasted for more than 7 minutes into recovery (Figure 3). He had shown significant wall motion abnormalities on his 2D echocardiography: transient left ventricular dilation with exercise, multiple wall motion abnormalities including anterior wall, LV apex and inferior wall. Baseline LV ejection fraction (LVEF) was 60% which dropped to 40% at peak exercise. He was advised admission to the local hospital, however, instead he agreed to take an aspirin, a beta blocker, a statin in my office and had blood samples for testing drawn and wanted to have a diagnostic coronary angiography the next morning which revealed: 90% ostial left main stenosis, 100% mid-LAD (left anterior descending artery) stenosis with collaterals from the right coronary artery (RCA), 100% second diagonal stenosis and 95% distal RCA stenosis. LV systolic function was preserved. He underwent coronary artery bypass surgery x 4 the next day. His hospital course was uneventful. A few weeks later, he returned to my office and performed a low-level treadmill exercise with no shortness of breath or ST changes. As of writing of this article, he has been undergoing cardiac rehabilitation program uneventfully.
ECGs
Discussion
There are at least 4 pertinent points of discussion that emerge from this case:
- Shortness of breath in men versus women as ‘Angina Equivalent’.
- Role of any regular stress testing in such cases.
- Abnormal stress echo findings.
- Markedly abnormal ST changes with treadmill.
To keep the discussion more relevant to my point of interest related to this case, I will focus mostly on the last point: Markedly abnormal ST changes during a treadmill. As per coronary angiography, he had multi-vessel CAD with 90% left main stenosis, therefore I will like to discuss the possible ST changes in the setting of left main stenosis and LAD stenosis and how to use that knowledge in a clinical setting.
ST Changes during Treadmill Stress Test
Exercise-induced ST depression although the most common criterion for the diagnosis of ischemic CAD is unable to discriminate the hemodynamically significant coronary artery obstruction [1]. Exercise induced ST elevation is less frequent than depression but it can identify ventricular wall motion abnormalities [2], ventricular aneurysm [3], and ischemia due to vasospasm or severe proximal coronary stenoses [4]. Lead aVR has not only been under-studied for CAD diagnosis but also mostly ignored in the past [5]. Identifying the LMCA obstruction will be of tremendous clinical importance for urgent treatment option and that is where the role of aVR needs to be explored. Because lead aVR monitors the left ventricular cavity viewing from apex to base [6], it is highly anticipated for this lead to be sensitive to proximal, anterior septal ischemia appearing as an injury current (ST elevation) when viewed from the left ventricular cavity [7].
ECG Changes: Left Main and Proximal Lad Stenoses
In most individuals, the left main coronary artery (LMCA) supplies approximately 75% of the left ventricular myocardial mass. Significant LMCA disease is present in 4-10% of patients undergoing coronary angiography but its total occlusion is rare and seen in 0.04-0.40% cases only [7] and can lead to severe hemodynamic deterioration resulting in rapid fatality [8]. Therefore the diagnosis of severe LMCA obstruction is of dire consequences in terms of appropriate treatment plans and estimating the prognosis.
Role of lead aVR in Ischemia Assessment: (aVR= Augmented Vector Right)
The lead aVR also referred to as "no man's lead", the "orphan lead", or "dead or simply forgotten lead" is directed downward and into the left ventricular cavity and therefore is thought to reflect inter ventricular septal ischemia [9, 10]. Originally, the lead aVR was made to obtain the electrical changes as viewed from the upper right side of the heart to include the right ventricular outflow tract and inter ventricular septum [10]. ST elevation can locate the coronary ischemic territory but the ST depression usually does not, however the latter abnormalities can help locate the anatomic territory if simultaneous myocardial perfusion imaging is performed [11]. The lead aVR is also helpful in clinical conditions like pericarditis, pulmonary embolism, tricyclic antidepressant toxicity, tension pneumothorax, stress cardiomyopathy and as a means of differentiating atrial tachyarrhythmias. The presence of ST elevation in lead aVR greater than ST elevation in lead V1 is 81% sensitive, 80% specific and has 81% overall accuracy for the prediction of acute LMCA obstruction. It has been shown that in patients undergoing coronary angiography, the prevalence of LMCA or 3-vessel CAD was 56% in those with ST elevation of more than 1 mm in lead aVR [12]. ST elevation in lead aVR in not an uncommon finding on exercise treadmill tests with an incidence of 10-25% [13]. ST elevation in aVR has the excellent sensitivity of 93% but an average specificity of 49% for the diagnosis of more than 50% left main stenosis in patients with Duke Treadmill scores of 11 or less. The specificity is remarkably improved to 82% when ST elevation in lead aVR is accompanied by ST elevation in V1 [14]. There are different theoretical explanations for ST elevation in aVR in the setting of LMCA obstruction/disease. Some consider ischemia of the basal inter ventricular septum with an injury vector in the frontal plane pointing in a superior direction toward lead aVR. Less ST elevation in V1 than aVR in LMCA obstruction has been explained by counterbalance in lead V1 of electrical forces from both anterior and posterior LV walls. In addition, aVR records a mirror-like image of leads V5-6 and therefore ST depression in V5-6 will show up as ST elevation in aVR [15]. An interesting study from Athens, Greece [13] revealed that the concomitant appearance of exercise-induced ST elevation in lead V1, Stelevation in lead aVR and ST depression in lead V5 as well as the isolated appearance of ST elevation in lead V1 detect significant LAD stenosis as single-vessel disease or significant stenoses of LAD and LCx (left Circumflex) in patients with double-vessel disease, whereas the appearance of ST elevation in aVR and ST depression in V5 but without ST elevation in V1 correlates strongly with significant LAD and RCA stenoses and usually indicates double-vessel CAD. In one study [7], it was reported that lead aVR ST elevation was noted in acute obstruction of the LAD proximal to the major septal branch but not in acute LAD obstruction distal to the major septal branch. Lead aVR ST elevation during angina pectoris has been reported in patients with significant LMCA stenosis [8]. Both acute LMCA and LAD obstruction generally produce anterior wall ischemia resulting in ST elevation in the precordial leads. Based on the prior knowledge, a study was conducted to test the concept that treadmill exercise-induced ST elevation in ECG lead aVR is an important indicator of significant left main coronary artery or ostial LAD stenosis [9]. The data from this study supported this hypothesis. Sensitivity, specificity and overall predictive accuracy were approximately 75-80% with high negative predictive accuracy (94%) but only modest positive predictive accuracy (44%). The finding of 1 mm or more ST elevation in aVR almost rippled the post-test likelihood of finding significant LMCA or ostial LAD stenosis. In addition, there was a strong relationship noted between the ST elevation in aVR and myocardial perfusion defect on a nuclear stress test (in my case reported here, similar association was noted between ST elevation in aVR and wall motion changes on stress echocardiography).
Shortness of Breath (Angina Equivalent)
This is another part of my case report that I simply want to touch upon without going into much detail. This patient's most significant symptom was extreme shortness of breath with exertion (walking up the stairs in his case). This shortness of breath (dyspnea) is as serious a symptom as angina in the assessment of patients with established or suspected coronary artery disease and thus sometimes it may manifest as shortness of breath which is painless equivalent of angina [7]. Dyspnea is considered to be angina equivalent by many clinicians and researchers [15]. In various studies, up to 25% older patients with known CAD reported dyspnea as the primary symptom in the absence of angina and also the reported incidence of dyspnea in women can be much higher than men [16]. Therefore, even though the symptoms of exertional shortness of breath are more common in women, as the present case shows it can be equally challenging and may represent angina equivalent in men as well.
Conclusions
ST elevation in aVR with a treadmill stress test:
ST depression in leads I, II and V4-6. ST elevation in aVR: more than 1 mm. ST elevation in aVR: generally more than in V1.
Other possibilities with ST elevation in aVR:
Proximal LAD occlusion. Severe triple-vessel CAD. Diffuse subendocardial ischemia Predictive Value of ST elevation in aVR:
ST elevation in aVR: 1 mm or more indicates proximal LAD/LMCA or 3-vessel CAD.
ST elevation in aVR: more than 1 mm predicts the need for CABG. ST elevation in aVR more than in V1 differentiates LMCA from proximal LAD occlusion. No ST elevation in aVR: almost excludes a significant LMCA disease.
In patients undergoing treadmill stress testing:
ST elevation more than 1 mm in aVR predicts LMCA or ostial LAD stenosis. Higher the ST elevation in aVR, worse is the mortality.
In enclosing this case report, I would like to remind the readers following two points:
1. Left main disease is the most feared and potentially most fatal CAD. Strangely it can be diagnosed with the assistance of the most ignored lead: aVR!
2. He had a very concerning extreme shortness of breath a month before visiting me. He did not see any physician and did not take any medical Rx for a month and remained ‘asymptomatic’. He had been walking ‘just fine’ for a month with severe 3-vessel CAD with 90% left main disease without any angina, myocardial infarction, arrhythmia or sudden cardiac death!
Can I dare say? “Is ignorance truly a bliss?” Not really.
References
-
Simonetti I, Rezai K, Rossen JD, Winniford MD, Talman CL, et al. (1991) Physiological assessment of sensitivity of noninvasive testing for coronary artery disease. Circulation 83 (5S3): 43-49.
-
Bruce RA, Fisher LD, Pettinger M, Weiner DA, Chaitman BR (1988) ST elevation with exercise: a marker for poor ventricular function and poor prognosis. Circulation 77(4): 897-905.
-
Mason RE, Likar I, Biern RO, Richard SR (1967) Multiple lead exercise ECG. Experience in 107 normal subjects and 67 patients with angina and comparison with coronary cine arteriography in 84 patients. Circulation 36: 517-525.
-
Nosration FJ, Froelicher VF (1989) ST elevation during exercise testing. Am J Cardiol 63(13): 986-988.
-
Engelen DJ, Gorgels AP, Cheriex EC, De Muinck ED, Ophuis AJ, et al. (1999) Value of ECG in localizing the occlusion site in the LAD artery in acute myocardial infarction. J Am Collcardiol 34(2): 389- 395.
-
Ward DE, Valantine H, Hui W (1983) Occluded left main stem coronary artery: report of five patients and review of published reports. Br Heart J 49(3): 276- 279.
-
Cheng TO (2007) Acute dyspnea on exertion is an angina equivalent. International Journal of Cardiology 115(1): 116.
-
Kligfield P, Gettes LS, Bailey JJ, Childers R, Deal BJ, et al. (2007) Recommendation and interpretation of the ECG: part I. J Am Cardiol 49(10): 1109-1127.
-
Uthamalingam S, Zheng H, Leavitt M, Pomerantsev E, Ahmado I, et al. (2011) Exercise-induced ST elevation in ECG lead aVR is a useful indicator of significant left main or ostial LAD coronary artery disease. JACC: Cardiovascular Imaging 4(2): 176-186.
-
Yamaji H, Iwasaki K, Kusachi S, Murakami T, Hirami R, et al. (2001) Prediction of left main coronary artery obstruction by 12-lead ECG. ST elevation in lead aVR with less ST segment elevation in lead V1. J Am Coll Cardiol 38(5): 1348-1354.
-
Michaelides AP, Psomadaki ZD, Aigyptiadou MK, Dimitris JR, George KA, et al. (2003) Significance of exercise-induced ST changes in leads aVR, V5 and V1. Discrimination of patients with single or multivessel coronary artery disease. Clin Cardiol 26(5): 226-230.
-
Kosuge M, Kimura K, Ishikawa T, Ebina T, Hibi K, et al. (2006) Combined prognostic utility of ST segment in lead aVR and troponin T on admission in non-ST elevation acute coronary syndromes. Am J cardiol 97(3): 334-339.
-
Neill J, Shannon HJ, Moton A, Muir AR, Harbinson M, et al. (2007) ST elevation in lead aVR during exercise testing is associated with LAD stenosis. Eur J Nucl Med Mol Imaging 34(3): 338-345.
-
Antono BD, Dupuis G, Burelle D, Andre Arsenault (2008) Silent Ischemia: Silent after all? Can J Cardiol 24(40): 285-291.
-
Fuller CM, Raizner AE, Chanine RA, Nahormek P, Ishimori T, et al. (1980) Exercise induced coronary arterial spasm: angiographic demonstration of ischemia by myocardial scintigraphy and results of pharmacologic intervention. Am J Cardiol 46(3): 500- 506.
-
Tuna KM, Tolga KH, Tekin A, Erol T, Tekin G, et al. (2008) Exercise induced ST elevation in leads aVR and V1 for the prediction of left main disease. Int J Cardiol 128(2): 240-243.
-
Viik J, Lehtinen R, Tech L, Niemela K, Malmivuo J (1997) The effect of lead selection on traditional and heart rate adjusted ST segment analysis in CAD detection during exercise. Am Heart J 134(3): 488- 494.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study