Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
We report a rare case of an anomalous origin of the left circumflex artery (LCX) from the proximal right coronary artery (RCA), along with an independent origin of the left anterior descending artery (LAD) from the right coronary cusp. Recognition of this coronary anomaly was pivotal in the preoperative assessment of a patient undergoing surgical aortic valve replacement (SAVR) for severe aortic stenosis. This case highlights the critical role of detailed preoperative imaging in identifying coronary anomalies to optimize operative planning and minimize the risk of intraoperative complications.
Maturi BP¹*, Yelam RK², Kamsala C³, Sagwal A⁴, Hyun SJ⁵, Jakka B⁶ and Dunde A⁶
¹UT Houston School of Medicine, USA ²RVM Institute of Medical Science and Research Center, India ³Narayana Medical College, India ⁴Maharaja Agrasen medical college, India ⁵Korea University College of Medicine, Republic of Korea ⁶Baptist Medical Center South, United States
Abbreviations
LCX: Left Circumflex Artery; RCA: Proximal Right Coronary Artery; LAD: Left Anterior Descending Artery; SAVR: Surgical Aortic Valve Replacement; AAOCA: Anomalous Aortic Origin of a Coronary Artery; CAAs: Coronary Artery Anomalies; CT: Computed Tomography; TAVR: Transcatheter Aortic Valve Replacement; CABG: Coronary Artery Bypass Grafting.
Introduction
Anomalous aortic origin of a coronary artery (AAOCA) encompasses a spectrum of congenital malformations in which a coronary artery arises from the aorta outside its native sinus of Valsalva [1].
Coronary artery anomalies (CAAs) are uncommon, with a reported incidence ranging from 1% on invasive angiography to 5.8% on computed tomography (CT) coronary angiography [2]. While many CAAs are clinically silent, certain variants may be associated with myocardial ischemia, arrhythmias, and sudden cardiac death particularly in younger patients or during exertion [3].
A particularly rare anomaly involves the LAD arising independently from the right coronary cusp in the absence of a left main artery. This configuration can have significant implications during aortic root procedures [4]. Given the complex anatomy and potential for surgical risk, careful evaluation and individualized management are essential [5]. We present a case highlighting this rare dual anomaly—an LCX originating from the proximal RCA and an LAD arising independently from the right coronary cusp—identified during preoperative evaluation for severe aortic stenosis.
Case Presentation
A 77-year-old male with hypertension, peripheral arterial disease, and hyperlipidemia was referred for

evaluation of severe aortic stenosis. He reported no chest pain, syncope, or anginal equivalents.
- Coronary angiography demonstrated:
- RCA arising from the right coronary cusp (Clip 1),
- LCX originating as a proximal branch of the RCA (Clip 1),
- LAD arising independently from the right coronary cusp (Clip 2),
- Absence of a left main coronary artery (Clip 3),
- No obstructive coronary artery disease.
Clip 1: LCX arising from proximal branch of RCA. Clip 2: LAD arising from Right coronary cusp.
Clip 3: RCA and LAD coming from Right coronary cusp, No Left Main artery.
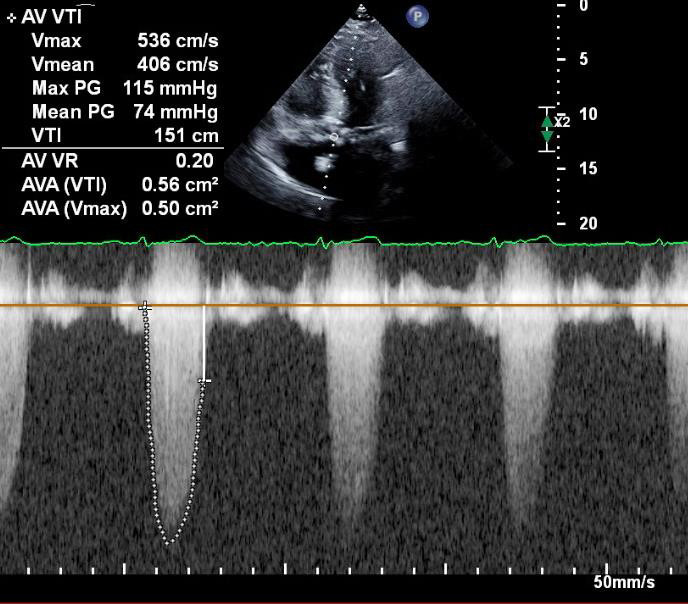
Transthoracic echocardiography revealed a heavily calcified, stenotic aortic valve with an area of 0.56 cm² and a mean gradient of 74 mmHg. Left ventricular ejection fraction was preserved.
Due to the identified coronary anomaly, transcatheter aortic valve replacement (TAVR) was considered high risk. The patient was referred for SAVR, with contingency planning for coronary artery bypass grafting (CABG) in case of intraoperative coronary compromise. An endoscopic saphenous vein harvest was performed prophylactically. The patient underwent successful bioprosthetic SAVR with a 25 mm Epic Max valve. Intraoperative assessment revealed preserved coronary flow, and CABG was not required (Figure 1).
Discussion
Coronary artery anomalies are present in less than 1% of the general population [6]. Anomalies originating from the right coronary cusp or right sinus of Valsalva are particularly rare [7], and clinical implications depend on the anomalous vessel’s course. The LCX typically follows a retroaortic trajectory, which is usually benign [8]. However, an LAD arising from the right coronary cusp—found in approximately 0.03% of patients—raises concern for a malignant interarterial course between the aorta and pulmonary artery, which is associated with increased risk of myocardial ischemia and sudden death [9]. Other courses, such as prepulmonic or trans- septal, are typically benign [10].
In our case, the LAD appeared to follow a benign course which is prepulmonic, but the concurrent presence of both anomalous vessels raised intraoperative risk. The absence of a left main coronary artery and the close proximity of both vessels to the aortic root increased the potential for iatrogenic injury during valve implantation. In one series, up to 16% of patients with an anomalous LCX experienced silent myocardial infarctions following SAVR, prompting consideration for prophylactic mobilization or grafting .
Although no standardized guidelines exist for managing CAAs in the context of SAVR, preoperative coronary imaging is strongly recommended to identify anomalies. Surgical planning should be individualized, incorporating anatomical and hemodynamic factors.
Contingency planning for CABG is prudent in case of compromised coronary perfusion during surgical manipulation.
Conclusion
This case highlights the importance of comprehensive preoperative imaging in patients undergoing aortic valve surgery. Identification of rare coronary anomalies enables tailored surgical planning, minimizing the risk of intraoperative complications and optimizing outcomes.
References
-
Jiang MX, Brinza EK, Ghobrial J, Tucker DL, Gupta S, et al. (2022) Coronary artery disease in adults with anomalous aortic origin of a coronary artery. JTCVS Open 10: 205-221.
-
Baz RO, Refi D, Scheau C, Baz A, Savulescu-Fiedler I, et al. (2024) Coronary Artery Anomalies: A Computed Tomography Angiography Pictorial Review. J Clin Med 13(13): 3920.
-
Evangelista M, Ferrero P, D’Aiello AF, Negura D, Micheletti A, et al. (2024) Coronary artery anomalies: what are they? when to suspect? how to treat? Transl Pediatr 13(7): 1242-1257.
-
Kanagala SG, Gupta V, Dunn GV, Kaur H, Zieneddine F, et al. (2023) Narrative Review of Anomalous Origin of Coronary Arteries: Pathophysiology, Management, and Treatment. Curr Cardiol Rev 19(6): 50-55.
-
Gentile F, Castiglione V, De Caterina R (2021) Coronary Artery Anomalies. Circulation 144(12): 983-996.
-
Liberthson RR, Dinsmore RE, Fallon JT (1979) Aberrant coronary artery origin from the aorta. Circulation 59(4): 748-754.
-
Villa AD, Sammut E, Nair A, Rajani R, Bonamin R, et al. (2016) Coronary artery anomalies overview. World J Radiol 8(6): 537-555.
-
Baldonado JJR, Greason KL, Crestanello JA, Dearani JA, Pochettino A, et al. (2022) Surgical Aortic Valve Replacement in the Setting of Anomalous Circumflex Coronary Artery. Ann Thorac Surg 113(2): 563-567.
-
Alameddine AK, Binnall BJ, Conlin FT, Broderick PJ (2019) Aortic Valve Replacement in 8 Adults with Anomalous Aortic Origin of Coronary Artery. Tex Heart Inst J 46(3): 189-194.
-
Roughneen PT, Al-Dossari GA (2016) The Anomalous Coronary Artery in Aortic Valve Replacement: A Case for Caution. Ann Thorac Surg 102(2): e113-e115.
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study
- The Hidden Impact of COVID-19 Lockdowns: A Study in Non COVID Venous Thromboembolism Cases-our Experience