Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study
Introduction: Heart attacks, or myocardial infarctions (MI), are a global health concern. Timely intervention hinges on public awareness and recognition of chest pain symptoms. This study delves into the correlation between basic chest pain knowledge, myocardial infarction, and demographic variables to uncover disparities influencing health outcomes. In the face of persistent cardiovascular challenges, understanding factors shaping awareness is vital. Demographics, including age, gender, socioeconomic status, education, and culture, impact health literacy. This research aims to illuminate the intricate relationship between these factors and fundamental knowledge essential for identifying and responding to chest pain, a potential indicator of myocardial infarction. Aim: This study systematically analyzes the correlation between chest pain knowledge, myocardial infarction, and demographic variables. The goal is to identify patterns and disparities for targeted interventions and improved public awareness. Methodology: Study highlighted stroke prevention as a priority for 83.7% (p) at a 5% significance level, determining a sample size of N=233 with a 10% non-response rate. Expert-validated questionnaire Annexure 1 was distributed to Uttar Pradesh residents through email and social media, ensuring anonymity and voluntary participation with consent. Statistical analysis involved presenting demographic variables as frequency (%), employing Chi-square Statistics to assess associations with knowledge outcomes, and using two independent sample proportion Chi-square tests to establish the Distribution of Association between basic chest pain and myocardial infarction knowledge and demographic variables, with P<0.05 as the significance threshold. Result: Significant associations were found between gender and occupation with basic knowledge of chest pain and myocardial infarction (heart attack) (Sig. < 0.05). No significant links were observed with education, economic status, and area of residence. Conclusion: The distribution of associations between basic knowledge of chest pain and myocardial infarction and demographic variables was examined in this survey-based study. Gender and occupation exhibited significant relationships, rejecting the null hypothesis. However, education, economic status, and area of residence showed no notable impact on understanding these health aspects.
Singh RR¹, Yadav PK², Jaiswal S³, Singh S³, Tripathi SK⁴* and Dikshit A⁵
¹Department of Emergency Medicine, Dr. Ram Manohar Lohia Institute, India ²Department of Forensic Medicine and Toxicology, Dr. Ram Manohar Lohia Institute, India ³Research Scholar Statistics, University of Lucknow, India ⁴Department of Forensic Medicine & Toxicology, King George’s Medical University, India ⁵Forensic Science Invertis University, India Embolism; eThrombosis
Abbreviations
MI: Myocardial Infarctions; Ho: Null Hypothesis.
Introduction
In the expansive domain of cardiovascular health, the connection between the basic comprehension of chest pain and myocardial infarction, colloquially known as a heart attack, stands as a critical juncture in the collective pursuit of public well-being [1]. Understanding the symptoms of chest pain and their correlation with demographic variables plays a pivotal role in formulating precise interventions and preventive strategies [2]. As the heartbeat of our communities reverberates through diverse backgrounds, lifestyles, and experiences, unraveling the intricate web that links basic knowledge of chest pain to myocardial infarction becomes imperative for fostering a healthier society [3, 4]. Chest pain, recognized as a cardinal symptom of myocardial infarction, often serves as the harbinger of a potentially life- threatening event [5]. Acknowledging the nuanced nature of chest pain and its association with heart health is paramount for the early detection and management of cardiovascular diseases [6].
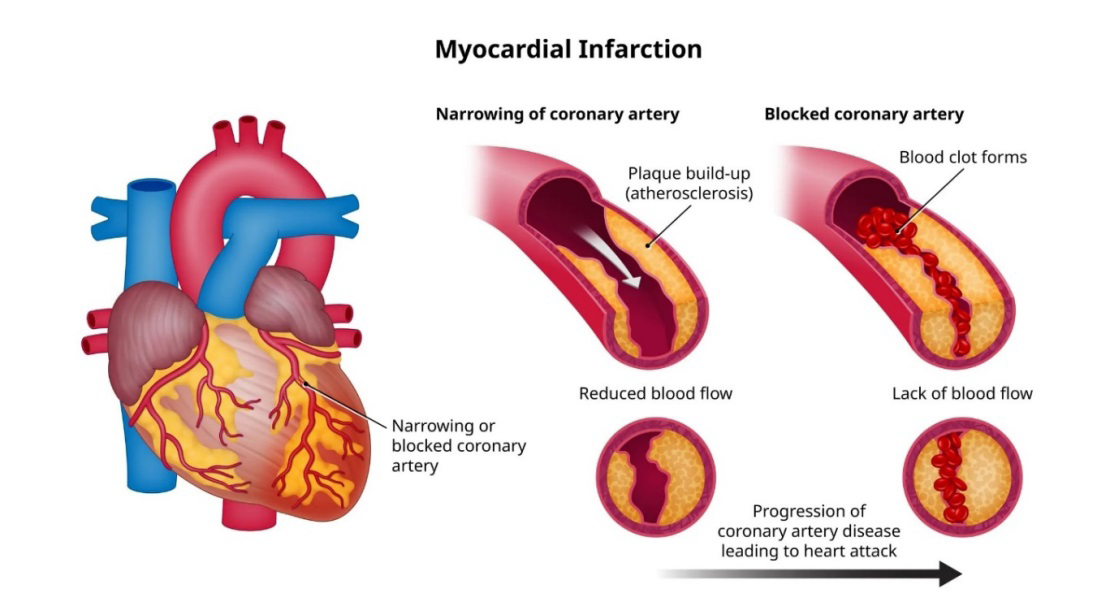
The primary factor contributing to a heart attack is the constriction of one or multiple arteries responsible for delivering blood to the heart (Figure 1) [7]. This occurrence stems from the accumulation of cholesterol deposits within the arterial walls, a phenomenon commonly referred to as atherosclerosis [8].
Consequently, this buildup limits the blood flow to the heart muscle, jeopardizing the delivery of essential oxygen [9]. Subsequently, the heart’s arteries may experience partial or complete blockage, and a heart attack may ensue in cases of sudden and severe obstruction.[10] A lack of awareness or misconceptions about chest pain symptoms can lead to delayed medical intervention, exacerbating the severity of myocardial infarctions and impeding positive health outcomes [11, 12]. This survey-based study embarks on a journey to discern the distribution of knowledge concerning chest pain and its link to heart attacks across diverse demographic spectra. Human societies are intricate mosaics woven from threads of age, gender, educational background, socio-economic status, and cultural nuances [13]. Understanding how these demographic variables intersect with the basic knowledge of chest pain and myocardial infarction is essential for tailoring health education initiatives and healthcare policies [14]. By unraveling the distribution of awareness within specific demographic groups, we aim to shed light on potential disparities in health literacy, allowing for targeted interventions to bridge the knowledge gap [15, 16].
While prior research has provided valuable insights into the relationship between chest pain awareness and myocardial infarction, numerous questions remain unanswered [17]. Some studies have explored general awareness levels, while others have delved into specific demographics, such as age or gender [18]. This survey explores the link between chest pain awareness, myocardial infarction, and demographic factors among cardiovascular patients. Additionally, those with comorbidities face higher COVID-19 susceptibility, potentially due to ACE2 expression and SARS-CoV-2’s impact on cardiovascular cells. Noteworthy risk factors for oxygen requirement include body mass index, low lymphocyte count, glucose intolerance, and dyslipidemia [19]. However, a comprehensive understanding necessitates a holistic examination that considers the intricate interplay of multiple demographic variables. This survey-based study seeks to build upon existing knowledge by providing a nuanced and detailed exploration of the distribution of association across a diverse range of demographic factors. By capturing data from various demographic backgrounds, including age groups, genders, educational levels, and socio- economic strata, we aim to create a comprehensive panorama of chest pain awareness. The survey instrument is designed to elicit responses that not only quantify the level of basic knowledge but also probe deeper into the factors influencing this awareness. Through rigorous data analysis, patterns will emerge, allowing us to draw meaningful conclusions about the distribution of association between chest pain awareness and myocardial infarction across diverse demographics. The findings of this study hold profound implications for public health strategies and interventions.
Methodology
Sample Size
Based on a previously published study by Hayashi et al. (2013), the need for information on preventing stroke recurrence was cited most frequently, accounting for 83.7% of responses (p) at a 5% level of significance. To achieve a margin of error (d) of 5%, the calculated sample size was determined to be n=210. Accounting for a 10% non-response rate, the optimal sample size required is N=n/ (1-0.1) =233. Thus, an optimum sample size of N=233 is needed.
Study Tool Development
A meticulously designed questionnaire was created after an extensive literature search. Comprising 17 open- ended multiple-choice questions, its purpose was to gather vital data on participants’ demographic details, their comprehension of chest pain & myocardial infarction (Heart attack), primary treatment methods to prevent stroke, and their awareness of these concepts in layman’s terms. Additionally, participants were encouraged to share their valuable opinions on the impact of these measures on patient care. Six experts (three faculty members and three residents) evaluated the questionnaire’s content validity by rating each item on a Likert scale (scoring 1-5) based on its simplicity, clarity, ambiguity, and relevance. Overall agreement was estimated as being 87.5% for simplicity (free marginal kappa - 0.82), 82.5% for clarity (free marginal kappa - 0.78), 92.3% for being free of ambiguity (free marginal kappa - 0.82), and 90% for relevance (free marginal kappa - 0.81), respectively.
Data Collection
The questionnaire was developed as a Google Form and sent to the target research population and all urban and rural regions of Uttar Pradesh via email and social media sites like WhatsApp. Participation in this online poll was entirely optional and fully anonymous. Before the poll could begin, all participants had to sign an informed consent form. Data computation only took completed forms into account.
Statistical Analysis
To discover trends and patterns in the knowledge level among stroke sufferers and their careers, the collected data was statistically examined. The percentage of demographic variables was presented as frequency (%). Chi- square Statistics determines the association between the demographic variable and knowledge outcome. P-value<0.05 was considered statistically significant. Two independent sample proportion Chi-square tests were used to determine the Distribution of Association between basic knowledge of chest pain & myocardial infarction (Heart attack) and demographic Variables categories.
Result
In the analysis of demographic variables, the chi-square test revealed a significant association between gender and basic knowledge of chest pain and myocardial infarction (heart attack), as indicated by the Sig. value of 0.015, which is less than the significance level of 0.05. Therefore, we reject the null hypothesis (Ho) and conclude that there is a noteworthy relationship between gender and the understanding of chest pain and myocardial infarction. Similarly, for the variable occupation, the chi-square test yielded a significant value of 0.026, also below the 0.05 threshold. This result suggests a meaningful association between occupation and basic knowledge of chest pain and myocardial infarction.
However, no significant associations were observed for other demographic variables, namely education, economic status, and area of residence, indicating that these factors do not have a significant impact on the basic knowledge of chest pain and myocardial infarction (Table 1).
- Demographic Variables
- Total (N=233) N (%)
- Chi-square p-value
- Gender
- Female
- 82(35.2)
- 6.453
- 0.015*
- Male
- 151(64.8)
- Education
- Illiterate
- 15(6.4)
- 0.666
- 0.414
- Literate
- 218(93.6)
- Occupation
- Government
- 55(23.6)
- 4.941
- 0.026*
- Private
- 178(76.4)
- Economic Status
- Below poverty line
- 43(18.5)
- 2.290
- 0.130
- Non-below-the-poverty line
- 190(81.5)
- Area
- Rural
- 96(41.2)
- 0.678
- 0.410
- Urban
- 137(58.8)
Table 1: Distribution of Association between basic knowledge of chest pain & myocardial infarction (Heart attack) and
Discussion
The level of knowledge of heart attack symptoms exhibited in our survey compares favorably with that of the few published reports from other studies. In a 1992 report from a survey regarding heart attack recognition conducted on 302 members of the general population in Dublin, Ireland, 67.5% of respondents we were reported that chest pain was an indicator of a heart attack [20]. In a survey of 1315 Mexican Americans and non-Hispanic whites in the general population in San Antonio, Tex, from 1979 to 1981, knowledge of heart attack symptoms differed by ethnicity and socioeconomic status, ranging from 39% to 82% for chest pain, from 26% to 51% for shortness of breath, and from 4% to 32% for the combination of sweating and nausea [21]. Investigate how gender influences the association between basic knowledge of chest pain and the occurrence of myocardial infarction. Discuss any observed disparities in awareness between men and women, and explore potential reasons for these differences.
Consider the impact on healthcare outcomes and the need for targeted educational interventions [22]. The proportion of MI patients who presented without chest pain was significantly higher for women than men (42.0% [95% CI, 41.8%-42.1%] vs 30.7% [95% CI, 30.6%-30.8%]; P < .001). There was a significant interaction between age and sex with chest pain at presentation, with a larger sex difference in younger than older patients, which became attenuated with advancing age [23]. Investigate the distribution of chest pain knowledge across different socioeconomic strata. Discuss whether there is a correlation between socioeconomic status and awareness of myocardial infarction symptoms. Consider how economic factors may influence access to healthcare information and resources, and discuss potential strategies to address disparities in awareness among different socioeconomic groups [24]. Examine the distribution of knowledge about chest pain and myocardial infarction based on participants’ educational backgrounds. Analyze whether individuals with higher educational attainment demonstrate better awareness. Discuss the role of education in shaping health literacy and how it can be leveraged to enhance public understanding of cardiac symptoms [25].
Conclusion
Our survey-based study investigated associations between demographic variables and knowledge of chest pain and myocardial infarction. Significant links were found with gender and occupation, leading to rejecting the null hypothesis. However, no notable impact on understanding these health aspects was observed with education, economic status, and area of residence. This underscores the nuanced nature of such associations, emphasizing the importance of considering specific demographic factors in health education and awareness programs.
Recommendations
Based on the significant associations between gender and occupation with knowledge of chest pain and myocardial infarction, it is recommended to implement targeted awareness campaigns focusing on gender-specific gaps and workplace-based health education programs, while continuing broad public health efforts to ensure widespread knowledge across all demographics; collaborations with healthcare institutions and further research are essential to refine strategies and address any underlying disparities, ultimately promoting better health outcomes and timely interventions.
Conflict of Interest: There is no conflict of interest.
Source of funding: None.
Ethical Clearance: The institutional ethics committee of the hospital gave its approval to the study protocol. The IEC Number is 26/15. All participants provided informed consent before the data was collected. It was promised to participants that their answers would be kept private and anonymous.
References
-
MacLachlan M (2004) Embodiment: Clinical, Critical and Cultural Perspectives on Health and Illness. McGraw-Hill Education, UK, pp: 207.
-
Buttar HS, Li T, Ravi N (2005) Prevention of cardiovascular diseases: Role of exercise, dietary interventions, obesity and smoking cessation. Experimental & clinical cardiology 10(4): 229-249.
-
Datta P, Nath S, Pathade AG, Yelne S, Datta Jr P (2023) Unveiling the Enigma: Exploring the Intricate Link Between Coronary Microvascular Dysfunction and Takotsubo Cardiomyopathy. Cureus 15(9).
-
Pearsall PP (1999) The heart’s code: Tapping the wisdom and power of our heart energy. Harmony, pp: 288.
-
Yee LL, Rubin AS, Bellamy RF (2000) Thoracic injuries. Anesthesia and Perioperative Care of the Combat Casualty–A Textbook of Military Medicine. A Publication of the Surgeon General Department of the Army of USA, pp: 455-477.
-
Blankstein R, Shaw LJ, Gulati M, Atalay MK, Bax J, et al. (2022) Implications of the 2021 AHA/ACC/ASE/ CHEST/SAEM/SCCT/SCMR chest pain guideline for cardiovascular imaging: a multisociety viewpoint. Cardiovascular Imaging 15(5): 912-926.
-
Harris PE (1987) Congestive cardiac failure: central role of the arterial blood pressure. Heart 58(3): 190-203.
-
Schwartz CJ, Valente AJ, Sprague EA, Kelley JL, Nerem RM (1991) The pathogenesis of atherosclerosis: an overview. Clinical cardiology 14(S1): 1-16.
-
Schremmer B, Dhainaut JF (1990) Regulation of myocardial oxygen delivery. Intensive Care Medicine 16: S157-S163.
-
Ritchie W (2024) So seriously as to cause partial block, or might be blocked completely.
-
Cytryn KN, Yoskowitz NA, Cimino JJ, Patel VL (2009) Lay public’s knowledge and decisions in response to symptoms of acute myocardial infarction. Advances in health sciences education 14(1): 43-59.
-
Horowitz CR, Rein SB, Leventhal H (2004) A story of maladies, misconceptions, and mishaps: effective management of heart failure. Social science & medicine 58(3): 631-643.
-
Fernandez L (2023) Unveiling Gender Dynamics: An In-depth Analysis of Gender Realities. Influence International Journal of Science Review 5(3): 61-70.
-
Sachdeva P, Kaur K, Fatima S, Mahak FN, Noman M, et al. (2023) Advancements in myocardial infarction management: exploring novel approaches and strategies. Cureus 15(9): e45578.
-
Palumbo R, Adinolfi P, Annarumma C, Catinello G, Tonelli M, et al. (2019) Unravelling the food literacy puzzle: Evidence from Italy. Food Policy 83: 104-115.
-
Schillinger D (2021) Social determinants, health literacy, and disparities: intersections and controversies. HLRP: Health Literacy Research and Practice 5(3): e234-243.
-
Sheifer SE, Manolio TA, Gersh BJ (2001) Unrecognized myocardial infarction. Annals of internal medicine 135(9): 801-811.
-
Przybylski AK, Murayama K, DeHaan CR, Gladwell V (2013) Motivational, emotional, and behavioral correlates of fear of missing out. Computers in human behavior 29(4): 1841-1848.
-
Yadav PK, Singh RR (2023) Oxygen Therapy and Associated Risk Factors for Home Isolated COVID-19 Patients: A Review. Journal of Clinical and Diagnostic Research 17(1): OE01-OE05.
-
Bury G, Murphy AW, Power R, Daly S, Mehigan C, et al. (1992) Awareness of heart attack signals and cardiac risk markers amongst the general public in Dublin. Ir Med J 85(3): 96-97
-
Hazuda HP, Stern MP, Gaskill SP, Haffner SM, Gardner LI (1983) Ethnic differences in health knowledge and behaviors related to the prevention and treatment of coronary heart disease: The San Antonio Heart Study. Am J Epidemiol 117(6): 717-728
-
Canto JG, Shlipak MG, Rogers WJ, Malmgren JA, Frederick PD, et al. (2000) Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. Jama 283(24): 3223- 3229.
-
Canto JG, Rogers WJ, Goldberg RJ, Peterson ED, Wenger NK, et al. (2012) Association of Age and Sex with Myocardial Infarction Symptom Presentation and In- Hospital Mortality. JAMA 307(8): 813-822.
-
Schultz WM, Kelli HM, Lisko JC, Varghese T, Shen J, et al. (2018) Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation 137(20): 2166-2178.
-
Kayaniyil S, Ardern CI, Winstanley J, Parsons C, Brister S, et al. (2009) Degree and correlates of cardiac knowledge and awareness among cardiac inpatients. Patient education and counseling 75(1): 99-107.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- The Hidden Impact of COVID-19 Lockdowns: A Study in Non COVID Venous Thromboembolism Cases-our Experience