Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
Introduction: Peripheral arterial disease provides evidence of the relationship between this pathology and other types of cardiovascular and cerebrovascular complications, currently showing high mortality rates. Objective: Estimate the relationshipbetween the topography of peripheral arterial disease and mortality. Method: An observational, descriptive, retrospective study was carried out with all the medical records of patients hospitalized with a diagnosis of peripheral arterial disease due to obliterative atherosclerosis of the aortoiliac and femoropopliteal sectors in the arteriology service of INACV, during the years 2018 and 2019 and a sample of 220 patients was selected. Results: An overall mortality of 9.5% was found, with 13.5% of deaths from the aortoiliac sector and 6.9% from the femoropopliteal. In the aortoiliac sector, deaths were associated with female sex and ischemic heart disease, while in the femoropopliteal it was associated with smoking. The main cause of death for the aortoiliac sector was hydroelectrolytic imbalance and for the femoropopliteal bronchopneumonia. Finally, no association was found between the occlusive pattern and the time at which death occurred, but the longer the disease duration, the more likely the amputation was to occur prior to death. Conclusions: The aortoiliac sector is approximately twice as likely to cause death as the femoropopliteal sector, which seems to be influenced by smoking as an associated factor.
Carménate AL¹, Zamora JLC²*, Figueroa AA³ and Gómez ML¹
¹Especialista de 1er Grado en Angiología y Cirugia Vascular, Instituto Nacional de Angiología y Cirugia Vascular, Cuba ²Máster en Ateroesclerosis, Instituto Nacional de Angiología y Cirugia Vascular, Cuba ³Doctor en Ciencias Médicas, Especialista de 2do Grado en Fisiología Normal y Patológica, Cuba Keywords: Peripheral Arterial Disease; Occlusive Pattern; Mortality
Abbreviations
PAD: Peripheral Arterial Disease; FP: Femoropopliteal; IC: Confidence Interval; Mean ± SD: Mean Standard; Deviation; HTA: High Blood Pressure; CI: Ischemic Heart Disease; ECV: Cerebrovascular Disease; EO: Stenoocclusive.
Introduction
Peripheral arterial disease (PAD) of the lower limbs is a major health problem not only because of its direct impact but also because of the systemic nature of the disease process and in many cases amputation of the lower limbs is necessary, thus increasing the risk of death [1]. Arteriosclerosis obliterans is the most common cause of arterial occlusive disease in adults. Its incidence increases annually and is recorded in 15 to 20% of subjects over 70 years of age. The definition of arterial occlusive disease of the lower limbs refers to any occlusive lesion or ante-stenos, which generates or does not generate a reduction in blood flow to said extremities [1, 2].
PAD is becoming more common in modern society, partly due to the increase in life expectancy. This pathology affected 202 million people worldwide in 2010. The growing interest in early diagnosis has occurred because it is related to atherosclerotic disease in other areas, such as coronary, cerebral, and carotid arteries, and increases the risk of cardiovascular events (death, acute myocardial infarction, stroke), in the order of 4 to 6% per year, in patients with the disease. Cardiovascular diseases remain the main cause of morbidity and mortality in developed and emerging countries. They are the main cause of death in Brazil, having been responsible, in 2006, for 29.4% of deaths in the country, while neoplasias were 15.1%. Because it is a chronic disease, the resources required for its treatment are high. In the North American population, the estimated cost per year was $5,955 per patient, with a tendency to continue increasing [3].
The main causes of mortality found by some researchers were cardiovascular diseases (42.2%), neoplasias (17.1%) and respiratory diseases. It is estimated that after age 40, the risk of PAD increases two to three times for every 10 years of age increase. PAD, in addition to increasing with age, also contributes to the increase in morbidity since it is the most common indication for lower limb amputations. The high association between PAD, coronary artery disease and carotid artery disease is evident, which predisposes these patients to a significant increase in the risk of developing acute myocardial infarction, ischemic stroke and vascular death. In this context, PAD is interpreted as an essential marker of systemic atherosclerosis and a predictor of infarction and stroke [4].
Since 1990, there has been an increase in the number of patients with PAD, with a 23% increase in the last decade due to total population growth, general aging, the increase in the incidence of diabetes worldwide and smoking in low- and middle-income countries [5].
In a prospective study with 10-year follow-up to evaluate mortality associated with PAD, a three-fold increased risk of death in general, 5.9 times higher for cardiovascular disease and 6.6 times higher for coronary heart disease was determined [5]. Classically, clinical factors such as age, heart disease, CKD and COPD and other associated factors such as malnutrition, anemia and hypoalbuminemia are associated with higher early and late mortality [6].
Death from coronary heart disease linked to PAD accounts for 40-60% of deaths, followed by stroke (10-20%) and only 20-30% of patients with arterial insufficiency of the lower extremities die from non-cardiovascular causes. Associated with higher mortality are: advanced age at presentation, smoking, diabetes, renal failure on hemodialysis, presentation with critical ischemia and involvement of the distal arteries (legs) [7].
Another factor frequently associated with cardiovascular mortality is obesity, its definition is based on the calculation of the body mass index (BMI = weight / height2, weight is represented in kilograms and height in meters). The risk of sudden death in obese people is three times higher than in non-obese people, and is double for the development of cardiovascular diseases [8].
Peripheral arterial disease of the lower limbs affects 8.5 million Americans aged 40 years and is associated with morbidity and mortality. The proportion of patients with coronary artery disease and peripheral arterial disease is 15- 40%. It is also suggested that the ankle-brachial index used to assess PAD has been considered an important marker of cardiovascular disease and predicts mortality from this cause [9].
Mortality from this disease in Europe increased between 1990 and 2010, reaching 3.5/100,000 people in Western Europe in 2010. These figures refer to mortality directly related to PAD; it should be noted that most of these patients die from complications related to coronary heart disease and stroke [10].
Gallardo PUJ, et al. [11] conducted a study in Cuba in 2005 on mortality in patients with PAD addressing the different causes of death, obtaining as a result that 1.6% of the total cases registered in the same, were deaths due to this disease specifically.
In the Statistical Yearbook of Health published by the Ministry of Public Health in 2017, it was reported that diseases of the arteries, arterioles and capillaries were the 7th cause of death in that year. Despite this, they do not quantify the PAD separately, so its real value is not estimated [12].
In the context of lower extremity PAD, the affected arteries include the distal aorta and the iliac, internal iliac, external iliac, femoral, popliteal and infra popliteal vessels, thus allowing a topographic classification that includes aortoiliac, femoropopliteal or distal disease depending on the affected arterial sector [13].
The absence or decrease of pulses will give us a topographic diagnosis of the location of the lesions. In case of occlusive disease of the aortoiliac sector, we will have an absence or decrease in the amplitude of the pulses in the entire extremity. In femoropopliteal disease, the femoral pulse will be present, but it will be absent in the popliteal and distal arteries [14].
An epidemiological study by Vogt MT, et al. [15] aimed to identify the correlation of the risk of becoming ill or dying associated with the presence of stenosis of segments of the major artery of the leg, indicated that smoking and high systolic blood pressure were the key risk factors associated with isolated aortoiliac and femoropopliteal arterial disease, both in men and women. The relative risk of mortality was 2 to 7 times higher in men and women with uni and multisegmental disease, involving the aortoiliac and femoropopliteal segments; the presence of tibioperoneal disease did not significantly increase relative mortality. These results suggest that the etiology and risk of mortality associated with atherosclerosis in the lower extremities may vary according to the anatomical site and/or severity of the lesion, where the sectors most frequently associated with the occurrence of death are the aortoiliac and femoropopliteal; taking into account the topographic extension of the disease to larger vessels, and therefore, with greater hemodynamic and clinical impact both locally and systemically.
Although we do not have exact figures, from what has been published in the literature we can infer that obliterative atherosclerosis, being one of the forms of peripheral arterial disease, is not an uncommon entity in our country. Specifically in Cuba there are no studies that relate the different locations of PAD with mortality; others mention the subject briefly as part of other research on PAD; even though it is a condition that is easy to diagnose, preventable and has very disabling consequences in its most advanced forms, we therefore consider it important to insist on the relevance of its systematic search in medical practice. There are contradictions regarding mortality due to steno- occlusive sectors, these two (femoropopliteal and aortoiliac) being the ones that generate the most controversy. However, it is extremely important to carry out this study because, by knowing the patient’s steno-occlusive pattern and the risk factors that could influence the occurrence of death, we could then offer individualized treatment aimed at avoiding future complications and death.
Methodological Design
Type of Study
A retrospective, longitudinal, descriptive observational study was conducted to describe the associationbetween the topography of peripheral arterial disease and mortality,in patients diagnosed with this pathology, hospitalized in the INACV arteriology service, during the years 2018 and 2019.
Universe
The universe consisted of hospitalized patients diagnosed with peripheral arterial disease.due to obliterative atherosclerosis of the aortoiliac and femoropopliteal sectorsin the arteriology service of INACV, during the years 2018 and 2019.
Sample
A sample of 220 patients diagnosed with peripheral arterial disease due to Fontaine grade 3 and 4 obliterative atherosclerosis was selected who met the proposed inclusion criteria. Inclusion Criteria:
- Patients over 18 years old
- Patients of both sexes
- Patients with a history of PAD due to Fontaine stage 3 and 4 obliterative atherosclerosis. Exclusion Criteria:
- Patients with medical records that do not contain the necessary data to carry out this study.
Operationalization of Variables (Annex I)
• Dependent Variables: Main output variable: AFrequency of deaths for each arterial sector: Ratio of quotient between the number of deaths and the total number of patients for each location. • Secondary Output Variables: Time in which death occurs for each sector: Time elapsed from the moment of diagnosis until death. Note that the date of diagnosis will be taken as the date that coincides with the day of the first admission for this pathology in the clinical history. It will be measured in days, months and years.
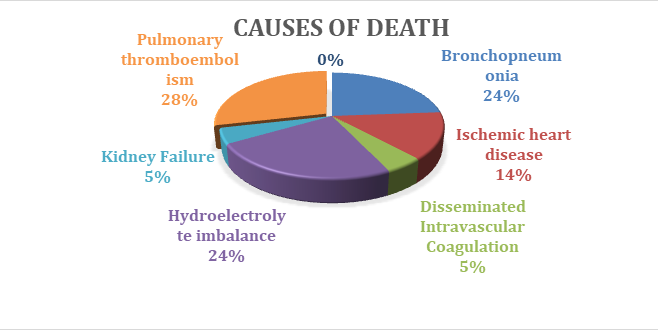
Causes of Death
Associated factors • Age: According to the date of birth recorded in the medical history and will be expressed in years completed. • Sex: Depending on the patient’s gender, the patient will be classified as female or male. According to the patient’s medical history. • Smoking: According to the WHO, it is a chronic addictive disease associated with tobacco consumption that develops with relapses. According to medical history • Smoker: Person who has smoked at least one cigarette in the last 6 months. • Ex-smoker: A person who has been a smoker but has remained abstinent for at least the last 6 months. • Non-smoker: A person who has never smoked or has smoked less than 100 cigarettes during his or her lifetime. • Personal Medical History: According to the data recorded in the medical history: high blood pressure (HBP), obesity, chronic kidney failure, ischemic heart disease and obesity • History of Major Amputation: Infra or supracondylar.
Independent or Explanatory and/or Confounding Variables:
- Stenoocclusive pattern: According to clinical history
- Aortoiliac
- Femoropopliteal Lower Limb Amputation: It will be determined by the presence or absence of major amputations in all the patients studied. According to the clinical history
Techniques for Obtaining Information
The information was obtained through the review of medical records by the 4th year angiology resident at the National Institute of Angiology and Vascular Surgery (INACV),during the months of April to December 2021, for which a spreadsheet was prepared where the data was collected.
Statistical Analysis Technique
The information was processed on a Dell laptop. Microsoft Word and Excel were used to create text, tables and graphs. The data was processed using the Statistical Package for the Social Sciences (IBM SPSS Statistics) version 21.0. The results were presented through summary measures for qualitative variables, such as (absolute and relative frequencies) and quantitative variables, such as the mean. The results were presented in tables and graphs for better understanding. The X2 test was performed to look for an association between the occlusive pattern and the possible causes of death, with a significance level of p˂ 0.05.
Ethical Considerations
The study was governed by the principles established in the Helsinki codes [16] and the standards of the Council for International Organizations of Medical Sciences (CIOMS) [17] and complied with the ethical requirements of value, scientific validity, respect and responsibility. All the standards of professional medical ethics were respected in carrying out the study. The data used were collected from the clinical history without any variation and with total confidentiality regarding the identity of the patients and the database of the information obtained was protected in compliance with computer security protocols.
Authorization to review the clinical histories of the patients was requested in writing from the center management. The work was carried out after being approved by the Research Ethics Committee (CEI) and the Scientific Council of INACV.
Results
To meet the objectives set out in the study, 220 patients were included. Regarding their general characteristics, hypertension was the most common risk factor (71.4% of patients), followed by smoking (60.5%) and ischemic heart disease (27.3%). The most common topography was femoropopliteal with 59.5%, with a higher number of patients in Fontaine stage 4 (74.1%). Major amputation was performed in 56.4% of the individuals and 21 died, representing 9.5% of the total sample Table 1.
| ♯ | Variables | Mean ± SD (No) | % | IC 95% |
|---|---|---|---|---|
| 1 | Age | 66.3 ± 11.2 | - | - |
| 2 | Female gender | 92 | 42 | 35.1 - 48.1 |
| 3 | HTA | 158 | 72 | 65.7 - 77.9 |
| 4 | CI | 60 | 27 | 21.2 - 33.2 |
| 5 | CVD | 8 | 4 | 1.1 - 6.1 |
| 6 | Obesity | 15 | 7 | 3.4 - 10.2 |
| 7 | Smoking Habit | |||
| Smoker | 133 | 61 | 53.9 - 67.1 | |
| Non-smoker | 39 | 18 | 12.6 - 22.8 | |
| Ex-smoker | 48 | 22 | 16.2 - 27.4 | |
| 8 | EO Pattern | |||
| Aortoiliac | 89 | 41 | 33.9 - 47.1 | |
| Femoropopliteal | 131 | 60 | 52.9 - 66.1 | |
| 9 | Fontaine Stadium | |||
| Grade 3 | 57 | 26 | 20.0 - 31.8 | |
| Grade 4 | 163 | 74 | 68.2 - 80.0 | |
| 10 | AMP pre- | |||
| Amputees | 124 | 56 | 49.7 - 63.0 | |
| 11 | Deaths | |||
| Deaths | 21 | 10 | 5.5 - 13.5 |
Table 1: General characteristics of the included patients.
IC: Confidence interval Mean ± SD: Mean standard deviation HTA: High Blood Pressure CI: Ischemic heart disease. ECV: Cerebrovascular disease. EO: Stenoocclusive. Table 1: General characteristics of the included patients.
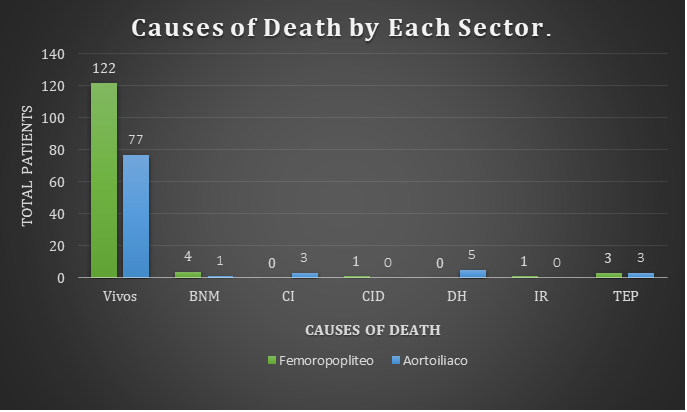
Table 2 shows the factors associated with mortality in the aortoiliac (AI) sector. Of the 89 patients with PAD included in this sector, 12 had died by the time of completion of our study, 7 of whom were women, representing 58.3%. These results suggest a tendency for women with aortoiliac involvement to die more often. Ischemic heart disease appears to be an important predictor of death for this sector, with 41.7%. It is striking that obesity was not directly related to death in this sector, being present only among the living (10.4%), with statistically significant values.
| ♯ | Variables | Total (89) | Alive (77) | Deaths (12) | P<0.05 |
|---|---|---|---|---|---|
| 1 | Age(Mean±SD) | 65.0 ± 10.6 | 64.0 ± 10.3 | 67.1 ± 11.5 | |
| Variables | N (%) | N (%) | N (%) | ||
| 2 | Female gender | 35 (39.3) | 28 (36.4) | 7 (58.3) | - |
| 3 | HTA | 63 (70.8) | 54 (70.1) | 9 (75.0) | - |
| 4 | CI | 25 (28.1) | 20(26,0) | 5 (41.7) | - |
| 5 | CVD | 4 (4.5) | 4 (5,2) | 0(0) | - |
| 6 | Obesity | 8 (9.0) | 8 (10.4) | 0 (0) | * |
| 7 | Smoking Habit | ||||
| Non-smoker | 7 (7.9) | 5 (6.5) | 2 (16.7) | - | |
| Smoker + Ex-smoker | 82 (92.1) | 72 (93.5) | 10 (83.3) | - | |
| Smoker | 60 (67.4) | 53 (68.8) | 7 (58.3) | - | |
| Ex-smoker | 22 (24.7) | 19 (24.7) | 3 (25.0) | - | |
| 8 | AMP pre- | ||||
| Amputees | 48 (53.9) | 43 (55.8) | 5 (41.7) | - | |
| 9 | Fontaine | ||||
| Grade 3 | 29 (32.6) | 24 (31.2) | 5(41,7) | - | |
| Grade 4 | 60 (67.4) | 53 (68.8) | 7 (58.3) | - |
Table 2: Factors associated with mortality in the aortoiliac sector.
| ♯ | Variables | Total (131) | Alive (122) | Deaths (9) | P<0.05 |
|---|---|---|---|---|---|
| 1 | Age (Mean±SD) | 67.1 ± 11.5 | 66.3 ± 11.2 | 67.1 ± 11.5 | - |
| N (%) | N (%) | N (%) | |||
| 2 | Female gender | 57 (43.5) | 53 (43.4) | 4 (44.4) | - |
| 3 | HTA | 95 (72.5) | 90 (73.8) | 5 (55.6) | - |
| 4 | CI | 35 (26.7) | 32 (26.2) | 3 (33.3) | - |
| 5 | CVD | 4 (3,1) | 4 (3,3) | 0 (0) | - |
| 6 | Obesity | 7 (5.3) | 7 (5.7) | 0 (0) | - |
| 7 | Smoking Habit | ||||
| Non-smoker | 32 (24.4) | 31 (25.4) | 1 (11,1) | - | |
| Smoker + Ex-smoker | 99 (75.6) | 91 (74.6) | 8 (88.9) | - | |
| Smoker | 73 (55.7) | 66 (54.1) | 7 (77.8) | - | |
| Ex-smoker | 26 (19.8) | 25 (20.5) | 1 (11,1) | - | |
| 8 | AMP pre- | ||||
| Amputees | 76 (58.0) | 70 (57.3) | 6 (66.7) | - | |
| 9 | Fontaine | ||||
| Grade 3 | 28 (21.3) | 25 (20.5) | 3 (33.3) | - | |
| Grade 4 | 103 (78.6) | 97 (79.5) | 6 (66.7) | - |
Table 3: Factors associated with mortality in FP.
Table 3 shows the factors associated with mortality in the femoropopliteal (FP) sector. Of the 131 patients with PAD included in this sector, 9 had died by the time our study was completed. The most relevant variable was smoking, which occurred in 88.9% of the deceased.
Table 4 shows the factors associated with the steno- occlusive pattern. Here, the higher frequency of presentation of PAD with femoropopliteal topography (131) than aortoiliac (89) is evident. Regarding smoking, we found that those patients who smoked at some point in their life predominated in patients with aortoiliac patterns, however, the higher number of non-smokers in the femoropopliteal sector (24.4%) was significant.The percentage of deaths was predominantly in the aortoiliac sector (13.5%).
| ♯ | Variables | Aortoiliac (89) | Femoropopliteal (131) | P<0.05 |
|---|---|---|---|---|
| 1 | Age(Mean±SD) | 65.0 ± 10.6 | 67.1 ± 11.5 | - |
| N (%) | N (%) | |||
| 2 | Female gender | 35 (39.3) | 57 (43.5) | - |
| 3 | HTA | 63 (70.8) | 95 (72.5) | - |
| 4 | CI | 25 (28.1) | 35 (26.7) | - |
| 5 | CVD | 4 (4.5) | 4 (3,1) | - |
| 6 | Obesity | 8 (9.0) | 7 (5.3) | - |
| 7 | Smoking Habit | |||
| Non-smoker | 7 (7.9) | 32 (24.4) | * | |
| Smoker + Ex-smoker | 82 (92.1) | 99 (75.6) | ||
| Smoker | 60 (67.4) | 73 (55.7) | ||
| Ex-smoker | 22 (24.7) | 26 (19.8) | ||
| 8 | Deaths | |||
| Deaths | 12 (13.5) | 9 (6.9) | - | |
| 9 | AMP pre- | |||
| Amputees | 48 (53.9) | 76 (58.0) | - | |
| 10 | Fontaine | |||
| Grade 3 | 29 (32.6) | 28 (21.4) | - | |
| Grade 4 | 60 (67.4) | 103 (78.6) | - |
Table 4: Factors associated with the steno-occlusive level.
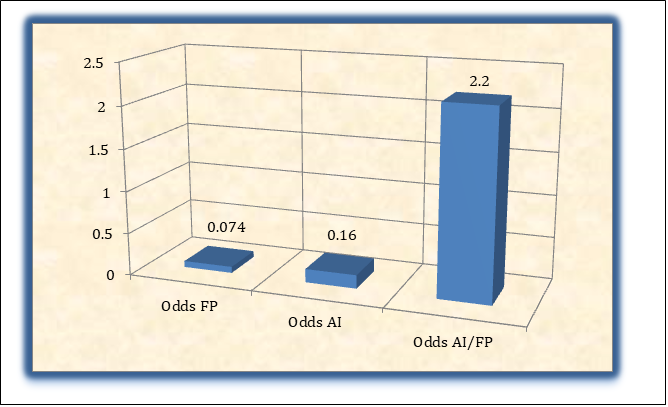
As can be seen in Figure 1-3, the odds for the FP sector was 0.074, which means that for every 100 patients with this topography, 7 die. As for the AI sector, the odds were 0.16 (for every 100 patients with AI disease, 16 die). The AI/FP odds with a value of 2.22% means that there is approximately twice the probability of dying for the aortoiliac sector compared to the femoropopliteal sector.
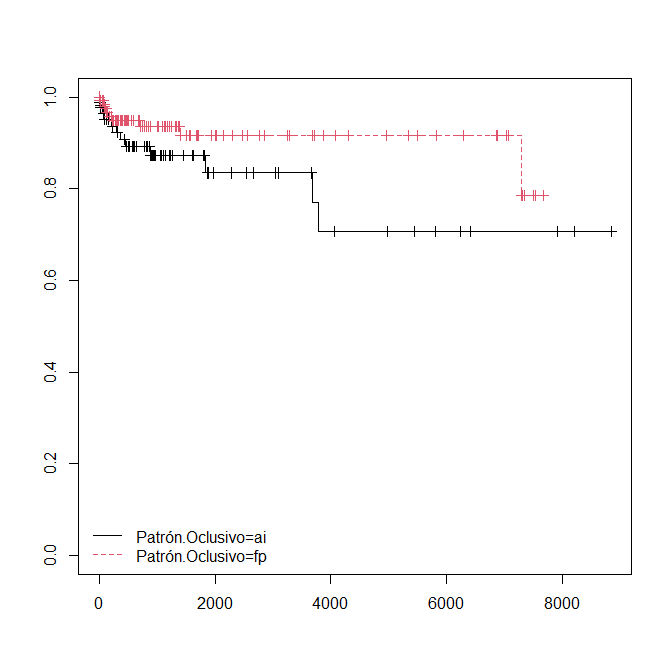
Vertical Axis: Probability of dying Horizontal axis: Time in days AI: Aortoiliac FP: Femoropopliteal Figure 4: Relationship between occlusive pattern and time at which death occurs.
It is shown that both curves representing the occlusive patterns decrease practically together, from the diagnosis of the disease, which shows that the occlusive pattern did not significantly influence the occurrence of death over time (Figure 4).
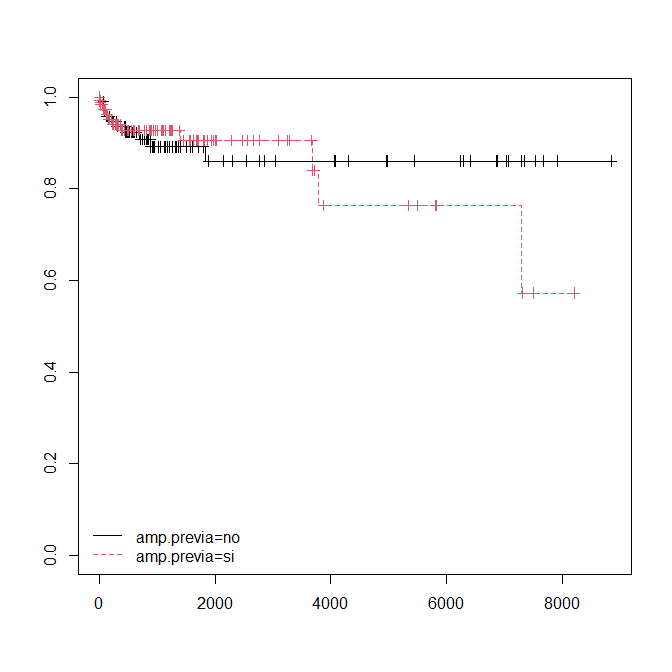
Vertical Axis: Probability of dying Horizontal axis: Time in days Amp: Amputation Figure 5: Relationship between previous amputation and time of occurrence of death.
It shows (Figure 5) how prior amputation initially does not seem to influence the occurrence of death, however, as the disease progresses, the curves separate, showing a slight tendency to die earlier in those patients who have already had a major amputation previously.
Discussion
There are many studies on the prevalence of mortality in patients with peripheral arterial disease, showing high rates of coronary events, stroke mortality and total mortality at 10 years. After 5 years, 20% of patients present intermittent claudication, myocardial infarction or stroke and mortality is 10-15%. We Martínez BI, et al. [18] and Zamora JL, et al. [19] found a similar mortality rate in general. Other research, however Arango CG, et al. [20], reveals a lower mortality rate (3.6%), which could be due to their diagnosis of this pathology.
Looking at the general characteristics described in the histories of the patients included in the study, we compare with other results such as those of Shabhay A, et al. [8], who concluded that more than half of the patients studied with peripheral arterial disease (23/42; 54.76%) underwent a major limb amputation, and also found a mean age of 60.06 ± 11.33 years; we found similar figures in our research. Our results are consistent with the medical literature regarding the risk factors associated with the disease [21, 22].
Leo SG, et al. [23], who found that the most affected steno-occlusive sector in peripheral arterial disease was the femoropopliteal, most of the patients we included had this occlusive pattern.
Regarding the factors that were most associated with mortality, Pinto in his study found that mortality was associated with the presence of renal failure, hypoalbuminemia and advanced stages of Fontaine, however, we did not find a significant association of these variables with the occurrence of death; not so with the publication of Leandro GS, et al. [24], where cardiovascular pathologies, ischemic heart disease in particular, are associated with the occurrence of death; comorbidities that in our work seemed to be relevant as a predictor of death.
On the other hand, Hasanadka R, et al. [25] demonstrated that myocardial infarction, congestive heart failure, chronic obstructive sleep apnea and dialysis use were predictive factors of death; although we were able to relate heart disease with the possible occurrence of death, kidney disease was not important as associated comorbidities. Criqui MH, et al. [26] demonstrated the incidence of cardiovascular disease in patients with peripheral arterial disease of up to 14.9% of patients with this pathology, however in our work we found a greater presence of these events in the patients studied.
Norgren L, et al. [7] found that death was associated with the femoropopliteal steno-occlusive pattern; however, in their study, the patients died mostly from ischemic heart disease, a pathology that in our study was not important for that steno-occlusive sector. In other publications in which the disease of the femoropopliteal sector is related to a higher mortality, it was observed that they were older patients, with more comorbidities and that they attended health services later [26]. Similarly, Pérez F, et al. [27] found that 58.50% of the patients belonged to the femoropopliteal sector and the most frequent cause of death was pulmonary thromboembolism; we differ, since the pathologies that were found as a cause of recurrent death in the infra inguinal sectors were respiratory infections (bronchopneumonia). Zamora C, et al. [28] found that ischemic heart disease in this sector was the most relevant risk factor, followed by smoking.
Gallardo PUJ, et al. [11], in their study, referred to the excessive male mortality and the majority of the deceased were 80 years old and older; however, our research found that the age (mean ± SD) was 67.1 ± 11.5 and one or the other sex did not predominate among the deceased. Regarding the specific causes of death due to peripheral vascular diseases, Gallardo PUJ, et al. [11] observed that the highest mortality rate was for abdominal aortic aneurysms; similar data were found by Cañas G, et al. [29] and Saiki M, et al. [30], who reaffirmed that they were the first cause of death due to atherosclerotic disease. Knowing that obliterative atherosclerosis of the aortoiliac sector constitutes the fundamental cause for both aneurysmal and steno-occlusive disease; it is not unusual to find in our study a higher number of deceased with high occlusive patterns.
Bizueto H, et al. [31], report in their study that the sector with the highest mortality found was the aortoiliac, with ischemic heart disease being the most frequent cause of death followed by acute renal failure and infections, although we agree as to the sector with the most deaths and we found causes such as heart disease and respiratory infections, pulmonary thromboembolism was the most frequent cause in our work in general and in the aortoiliac sector it was hydroelectrolytic imbalance. Bertele V, et al. [32] also associate mortality with more proximal steno-occlusive lesions.
Martínez C, et al. [33], during the year 1977, found that the most frequent causes of death were pulmonary thromboembolism, followed by ischemic heart disease, cerebrovascular accidents and infections. We agree with the majority of the causes despite not having deaths due to cerebrovascular disease.
Unkart JT, et al. [34] associated more extensive steno- occlusive disease with the occurrence of death from cardiovascular events. We agree with this study since in patients with aortoiliac involvement, ischemic heart disease seemed to be the most important predictor of death, finding that all patients who died as a result of ischemic heart disease belonged to this sector; on the other hand, other authors reveal that heart disease was more relevant in the femoropopliteal sector [34].
Limonta O, et al. [35], in their study on Clinical and surgical characterization of patients with aortoiliac peripheral arterial disease during the years 2010 to 2012, found that the predominant risk factors for aortoiliac disease were smoking followed by hyperlipidemia and diabetes mellitus; while we found female sex as a possible predictor of death and ischemic heart disease in that same order of importance.Multiple studies have suggested thatAortoiliac disease occurs more frequently in male patients, smokers, obese patients with associated arterial hypertension, similar to what we found in the patients included in our research [36, 37, 38].
Onur-Beyaz M, et al. [39] attributed higher mortality to patients with steno-occlusive lesions of the aortoiliac sector, associating deaths with the most advanced stages of the disease. We agree on the occlusive pattern that causes the most deaths, however, no significant relationship was found between death and Fontaine evaders 3 and 4.
Since peripheral arterial disease, coronary artery disease and cerebrovascular disease are manifestations of the same process, it is not unusual for all three to occur at the same time, and most deaths are due to heart disease, or other vascular causes, criteria with which we agree, although ischemic heart disease was not among the main causes of death [40, 41, 42, 43].
Redondo F, et al. [44] obtained a total mortality of 2.21% and associated with cardiovascular events of 3.23%, coinciding with our work, although they found cerebrovascular disease in 6.45% of the deceased, we did not find it among the deceased in our study.
In the PARTNERS study, it was found that 32% of patients had either coronary disease or cerebrovascular disease, and 24% had involvement of all 3 territories. On the other hand, the main cause of late death in patients with PAD was ischemic heart disease (up to 50%), while Regalado, et al. [45] found a higher percentage (70%) for this same cause, unlike our study where pulmonary thromboembolism, followed by bronchopneumonia and hydroelectrolytic imbalance were the main causes of death; and although ischemic heart disease was found among them, it was not the most striking, representing 14% [46, 47, 48].
Regarding ischemic manifestations, Regalado found extensive lesions in 32.57%, while we had a significantly higher percentage in our work since we work with patients in advanced stages of the disease.
Vega MA, et al. [49] reported that mortality was higher in the group of patients with more severe peripheral vascular disease, the crude mortality of the population studied was 6%, 18% and 24% at 1, 2 and 3 years respectively., which coincides with our work; however, Vega MA, et al. [49] related the occurrence of death with advanced age, which differs from our study since age in years did not seem to influence the occurrence or not of death.
In Spain, data from February 2017 published by the National Institute of Statistics hold PAD responsible for 29.4% of deaths, with ischemic heart disease being the most frequently involved in men and stroke in women. Vega MA, et al. [49], Mercedes G [50], although we did not relate sex with the possible cause of death, none of them was due to cerebrovascular disease; in addition, the percentage of deaths we found was much lower.
In a study on the prevalence and risk factors associated with peripheral arterial disease in Brazil in 2011, it was found that cerebrovascular diseases constitute a significant socioeconomic burden that accounted for about 31% of all deaths in that year, not coinciding with our study where these pathologies were not found as a cause of death [51]. Another clinical trial with patients with PAD where their causes of death were investigated found a mortality rate of 9.1% in the sample studied, associated with advanced stages of Fontaine, and comorbidities such as acute myocardial infarction, cerebrovascular diseases and diabetes mellitus. The most frequent cardiovascular causes of death were sudden death and stroke, while the non-cardiovascular causes of death were tumors; although we found cardiovascular causes in our study, we did not have deaths due to cerebrovascular diseases or tumors [52].
Muluk SC, et al. [53] found that the main cause of death was coronary origin (40-60%), followed by cerebrovascular accidents (10-20%) and only 20-30% of the patients with PAD died from non-cardiovascular causes, which was not the case in our study. The following were associated with higher mortality: advanced age at presentation, smoking, diabetes and renal failure, factors that were also found by us, despite not working with diabetic patients. Muluk SC, et al. [53] also suggest that death is mostly associated with distal occlusive patterns, which was not the case in our study where the largest number of deaths were in the aortoiliac sector, where we also did not include diabetic patients who could contribute a greater number of patients with involvement of infrainguinal sectors.
Koon Y, et al. [54] found that 45.7% of patients with a previous amputation died within 3 years after surgery, and Kennedy GEM, et al. [55] found that 44% of amputated patients had died within a 2-year period. Although we found a higher death expectancy in previously amputated patients, we observed that they were more likely to die after 10 years, similar to what was observed by Barbosa B [56] who at the same time found that 68% of amputated patients had died. On the other hand, Escarreño L, et al. [57], in their study on the Epidemiology of PAD in Mexico, found an annual mortality of 4-6% due to peripheral arterial disease and when a major amputation was performed as a complication of this disease, mortality increased up to 30%, which coincides with our study where patients with a previous amputation seem to die earlier than those who have not been amputated (Figure 5).
According to a study on diagnosis and treatment of peripheral arterial disease of the lower limbs carried out by the Mexican Social Security Institute, a mortality rate of close to 50% at 5 years and 70% at 10 years was determined. We agree with this study since after 10 years of evolution of the disease there is a greater probability of death occurring, regardless of the steno-occlusive sector affected by the patients, which was what really occupied us in our research. (Figure 4) [58].
When comparing our results with other studies conducted worldwide, we found similar patterns in terms of disease prevalence, being higher in men than in women, associated with risk factors such as smoking, high blood pressure, ischemic heart disease and obesity. Mortality rates continue to rise, even more so after 10 years of disease progression, with deaths mostly due to cardiovascular and cerebrovascular events, associated with advanced forms of the disease and prior amputation [59, 60, 61, 62, 63, 64, 65, 66, 67, 68].
Conclusions
- The aortoiliac sector is approximately twice as likely to die compared to the femoropopliteal sector, which appears to be influenced by smoking as an associated factor [69, 70, 71, 72, 73].
- 9.5% of patients died, of which 13.5% occurred in the aortoiliac sector and 6.9% in the femoropopliteal sector [74, 75, 76, 77].
- The predominant cause of death in the aortoiliac sector was hydroelectrolytic imbalance followed by ischemic heart disease, while in the femoropopliteal sector it was bronchopneumonia [78, 79, 80, 81].
- No relationship was found between the steno-occlusive pattern and previous amputation with respect to the time at which death occurred [82, 83, 84].
Recommendations
To include in future studies on the subject a greater number of patients with peripheral arterial disease due to diabetic macroangiopathy, with distal patterns, minor amputations and Fontaine stage IIb, as well as to increase the total number of deaths studied.
References
-
Parra BAJ (2009) Peripheral arterial disease: Current treatment recommendations. Pontificia Universidad Javeriana, Colombia, pp: 11.
-
Cabrera M, Fernández J, Marrero I, Ramírez N, Álvarez K, et al. (2009) Autologous hematopoietic stem cell transplantation in ischemic lower limbs of patients with atherosclerosis obliterans in stages III-IV of the Fontaine classification. Experience in Cienfuegos. Cuban Rev Hematol Inmunol Hemoter 25.
-
Mota DC, Santos J DM, da Silva (2017) Peripheral obstructive arterial disease: integrative review. Uningá Magazine 53(1): 120-125.
-
Mota MI, Mota I, Matheus F, Max O, Villar L, et al. (2019) Occurrence of depressive symptoms in ideosos patients with peripheral arterial disease. Electronic Journal Acervo Saúde / Electronic Journal Collection Health 32.
-
Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber MR, et al. (1992) Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med 326(6): 381-386.
-
Cabezuelo Adame X, Vega de Ceniga N, Aramendi Arietaaraunabe C, González Fernández A, Estallo Laliena L (2018) Overall prognosis of patients with critical limb ischemia. Elsevier Spain, SLU.
-
Norgren L, Hiatt W, Dormandy J, Nehler M, Harris K, et al. (2007) Inter-Societ Consensus for the Management of Peripheral Arterial Disease (TASC II).J Vasc Surg 45: S5-S67.
-
Anderson H, Márquez M, Barboza H, González L (2020) Anthropometric indicators and cardiovascular risk in overweight and obese adults. Legal deposit.
-
Shabhay A, Horumpende P, Shabhay Z, Mganga A, Van Baal J, et al. (2021) Clinical profiles of diabetic foot ulcer patients undergoing major limb amputation at a tertiary care center in North-eastern Tanzania. BMC Surg 21(1): 34.
-
Rev Esp Cardiol (2018) ESC Guidelines 2017 on the diagnosis and treatment of peripheral arterial disease, developed in collaboration with the European Society for Vascular Surgery (ESVS) 71(2): 111.e1-e69.
-
Gallardo Pérez UJ, Seuc Jo AH, Chirino Carreño N, Puentes Madera I (2008) Mortality due to peripheral vascular diseases in Cuba in 2005. Rev cubana Invest Bioméd 27(2).
-
Ministry of Public Health (2019) Health Statistics in Cuba. Statistical Yearbook 2019. Havana Cuba: Directorate of Medical Records and Health Statistics.
-
Sibley RC, Reis SP, MacFarlane JJ, Reddick MA, Kalva SP, (2017) Noninvasive physiologic vascular studies: A guide to diagnosing peripheral arterial disease. Radiographics 37(1): 346-357.
-
Ducajú GM, Conejero AM (2017) Chronic lower limb ischemia. Peripheral arterial disease. Medicine 12(41): 2440-2447.
-
Vogt MT, Wolfson SK, Kuller LH (1993) Segmental arterial disease in the lower extremities: correlates of disease and relationship to mortality. J Clin Epidemiol 46(11): 1267-1276.
-
World Medical Association (2013) Declaration of Helsinki. Ethical principles for medical research involving human subjects. 64th WMA General Assembly. Fortaleza, Brazil, October 2013. Updated Helsinki guidelines for clinical research get mixed reviews. JAMA.
-
Cuello M, Ramos P, Etcheverry J (2017) Update of the guidelines of the Council for International Organizations of Medical Sciences (CIOMS). ARS MEDICA Rev. de Ciencias Médicas 42(3).
-
Bolaños Martínez I, Chaves Chaves A, Gallón Vanegas L, Morera MI, López Barquero H (2019) Peripheral arterial disease in the lower limbs. Med Leg Costa Rica 36(1): 84- 90.
-
Cabrera Zamora JL, Hernández Seara A, Viña Cisneros H, Jaime Cabrera Z (2021) Cardiovascular risk factors associated with peripheral arterial disease of the lower limbs in its early stages. Rev Cubana Angiol Cir Vasc 22(1): e194.
-
Arango CG, Álvarez JC, García JF, Correa MO (2017) Epidemiological profile of patients with peripheral artery disease affiliated to an eps in colombia in 2016. pp: 1-58.
-
Onofrei AV, Ceasovschih A, Marcu DTM, Adam CA, Mitu O, et al. (2022) Mortality risk assessment in peripheral arterial disease-the burden of cardiovascular risk factors over the years: A single center’s experience. Diagnostics (Basel) 12(10): 2499.
-
Rozo-Ortiz EJ, Vargas-Rodríguez LJ, Agudelo-Sanabria MB (2019) Leriche syndrome. Med Int Mex 35(4): 627- 631.
-
Leo GS, Montbriand J, Eisenberg N, Roche-Nagle G (2022) Outcomes of Hybrid Procedures for Treating Peripheral Arterial Disease: A 5-Year Single-Center Experience. Cir Cir 90(5).
-
Leandro GS, Parolin SC, Moro CMC, Carvalho DR (2018) Mining of data in the assessment of deaths after amputation surgery. J Vasc Bra Joinvile 17(1): 1018.
-
Hasanadka R, McLafferty RB, Moore CJ, Hood DB, Ramsey DE, et al. (2011) Predictors of wound complications following major amputation for critical limb ischemia. J Vasc Surg 5(5): 1374-1382.
-
Criqui MH, Matsushita K, Aboyans V, Hess CN, Hicks CW, et al. (2021) Lower extremity peripheral artery disease: Contemporary epidemiology, management gaps, and future directions: A scientific statement from the American heart association. Circulation 144(9): e171- 191.
-
Franco Pérez N, Valdés Pérez C, Lobaina González R, Inglés Maury N (20010 Behavior of morbidity and mortality in patients with diabetic foot. Rev cuba Angiol y Cir vasc pp: 52-57.
-
Zamora CJL, Seara HA, Cisneros VH, Guzmán MAH, Díaz LM, et al. (2013) Characteristics of major amputations in patients with acute thrombotic arterial ischemia of the lower limbs. Cuban Journal of Angiology and Vascular Surgery 14(1): 1-7.
-
González-Cañas E, Giménez-Gaibar A, Perendreu- Sans J, Falcó-Fagés J, Bellmunt-Montoya S, et al. (2007) Spontaneous abdominal aortic rupture due to penetrating ulcer treated by endovascular repair. Angiology 59(2): 173-177.
-
Saiki M, Nishimura K, Ikebuchi M, Hiroe T, Tachibana M, et al. (2003) Mycotic abdominal aortic pseudo aneurysm caused by a penetrating atherosclerotic ulcer: report of a case. Surg Today 33(9): 698-701.
-
Bizueto-Rosas H, Martínez-Blanco DF, Serrato-Auld RC, Hernández-Pérez DNA, Leyva-Rivera DPE, et al. (2021) Arteriographic pattern and morbidity and mortality of atherosclerotic lesions of the lower limbs in the beneficiaries of the “Dr. Antonio Fraga Mouret” Specialty Hospital Medigraphic.com pp: 1-9.
-
Bertele V, Roncaglioni MC, Pangrazzi J, Terzian E, Tognoni EG (1999) Clinical outcome and its predictors in 1560 patients with critical leg ischaemia. Chronic Critical Leg Ischaemia Group. Eur J Vasc Endovasc Surg 18(5): 401- 410.
-
Martínez CJ, Maranges L, de Armas Vicent Y, EdreiraPerez J, García AG, et al. (2021) Major amputations of the lower limbs due to vascular causes. Epidemiological study 22: 517-540.
-
Unkart JT, Allison MA, Araneta MRG, Ix JH, Matsushita K, et al. (2020) Burden of peripheral artery disease on mortality and incident cardiovascular events. Am J Epidemiol 189(9): 951-962.
-
Ortiz Limonta D, Sánchez de la Guardia D, ChércolesCazate L (2013) Clinical and surgical characterization of patients with aortoiliac peripheral arterial disease. Median 17(8): 3049-3059.
-
Martinez J, Diaz JJ, Lujan VP, Fernandez MR, Ramirez E (2017) Aortoiliac occlusive disease or Leriche syndrome. Rev Colomb Cir 32(3): 214-222.
-
Restrepo M, Castro M, Munoz M, Daboin J (2018) Clinical case of interest: Leriche syndrome. An unusual manifestation of peripheral arterial disease. Biosalud 17(2): 105-111.
-
Azañero-Haro J (2022) Leriche Syndrome: Its Diagnosis in Peripheral Arterial Disease. Gac Med Bol 45(1): 75-78.
-
Onur-Beyaz M, Demir I, Ozer-Ulukan M (2021) Comparison of Atherectomy, drug-eluting balloon, and combined treatment efficiency by near infrared spectroscopy. Cir Cir 89(3): 342-346.
-
Colantonio LD, Hubbard D, Monda KL, Mues KE, Huang L, et al. (2020) Atherosclerotic risk and statin use among patients with peripheral artery disease. J Am Coll Cardiol 76(3): 251-264.
-
Pabon M, Cheng S, Altin SE, Sethi SS, Nelson MD, et al. (2022) Sex differences in peripheral artery disease. Circ Res 130(4): 496-511.
-
Matsushita K, Ballew SH, Coresh J, Arima H, Ärnlöv J, et al. (2017) Measures of chronic kidney disease and risk of incident peripheral artery disease: a collaborative meta- analysis of individual participant data. Lancet Diabetes Endocrinol 5(9): 718-728.
-
Alonso-Pérez M, Estevan J, Domínguez L (2003) Epidemiology, forms of presentation of occlusive arteriosclerotic pathology of the distal femoropopliteal sector 55 (S1): S5-S19.
-
Félix-Redondo FJ, Subirana I, Baena-Diez JM, Ramos R, Cancho B, et al. (2020) Prognostic significance of peripheral arterial disease diagnosed by the ankle- brachial index in the general Spanish population. Aten Primaria 52(9): 627-636.
-
Regalado-Solís F, Ziga-Martínez A, Olivares-Cruz S, Sierra-Juárez MÁ, Santillán-Aguayo E, et al. (2021) Perioperative mortality and comorbidities in patients with vascular amputations. Mexican Journal of Angiology 49(3): 80-87.
-
Kullo IJ, Rooke TW (2016) Peripheral artery disease. N Engl J Med 374(9): 861-871.
-
Hirsch AT, Criqui MH, Treat-Jacobson D, Regensteiner JG, Creager MA, et al. (2001) Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 286(11): 1317-1324.
-
Criqui MH, Aboyans V (2021) Epidemiology of peripheral artery disease. Circ Res 116(9): 1509-1526.
-
Vega Martínez A, Pérez García R, Abad S, Verde E, López Gómez JM, et al. (2008) Peripheral vascular disease: prevalence, mortality, and association with inflammation in hemodialysis. Nephrology 28(3): 311-316.
-
Mercedes G (2019) Spanish Society of Angiology and Vascular Surgery (SEACV). Chapter on Endovascular Surgery. Madrid, Spain.
-
Makdisse M, Pereira A da C, Brasil D de P, Borges JL, Machado-Coelho GLL, et al. (2008) Prevalence and risk factors associated with peripheral arterial disease in the Hearts of Brazil Project. Arq Bras Cardiol 91(6): 370- 382.
-
Kochar A, Mulder H, Rockhold FW, Baumgartner I, Berger JS, et al. (2020) Cause of death among patients with Peripheral Artery Disease: Insights from the EUCLID trial. Circ Cardiovasc Qual Outcomes 13(11): e006550.
-
Muluk SC, Muluk VS, Kelley ME, Whittle JC, Tierney JA, et al. (2001) Outcome events in patients with claudication: a 15-year study in 2777 patients. J Vasc Surg 33(2): 251- 257.
-
Koon Y, Muder RR (2012) Identifying the incidence of and risk factors for reamputation among patients who underwent foot amputation. Ann Vasc Surg 26(8): 1120- 1126.
-
Kennedy GEM, Mcgarry K, Bradley G, Harkin DW (2019) All-cause mortality among patients undergoing above and below knee amputation in a regional vascular center within 2014 2015. Ulster Med J 88(1): 30-35.
-
Barbosa B (2020) Profile of amputee patients: A prevalence study. Course Completion Work presented to the Nursing Graduation Course. Faculdade de Educação e Miio Ambiente- FAEMA Brazil: Júlio Bordignon Library – FAEMA.
-
Laparra-Escareno H, Anaya-Ayala JE, Lozano-Corona R, García-Alva R, Cuen-Ojeda C, et al. (2019) Epidemiology of peripheral arterial disease in Mexico. Mexican Journal of Angiology 47(2).
-
Mexican Social Security Institute (2017) Diagnosis and treatment of peripheral arterial disease of the lower limbs. Clinical practice guide, update.
-
Suarez C, Lozano F (2012) Spanish Multidisciplinary Consensus Guideline on Peripheral Arterial Disease of the Lower Extremities. In: 1st (Edn.), Madrid: Luzan SA, Spain.
-
Pereira Filho AJG, Sartipy F, Lundin F, Wahlberg E, Sigvant B (2022) Impact of ankle brachial index calculations on peripheral arterial disease prevalence and as a predictor of cardiovascular risk. Eur J Vasc Endovasc Surg 64(2-3): 217-224.
-
Chen S, Dai Y, Ma X, Peng H, Wang D, et al. (2022) Personalized optimal nutrition lifestyle for self obesity management using met algorithms. Sci Rep 12(1): 12387.
-
Forés R, Alzamora MT, Pera G, Baena-Díez JM, Mundet- Tuduri X, et al. (2018) Contribution of the ankle-brachial index to improve the prediction of coronary risk: The ARTPER cohort. PLoS One 13(1): e0191283.
-
Hershson AR, Belcastro F, Santos AD, Giorgi MA, Giunta G, et al. (2015) Consensus on Peripheral Vascular Disease Argentine Society of Cardiology Area of Consensuses and Standards. Rev Argentina de Cardiología pp: 83.
-
(2018) Asymptomatic peripheral arterial disease in patients with risk factors for metabolic syndrome. Rev Cuba Angiol Cir Vasc 19(2): 91-103.
-
Castañeda-Zúniga F, Joffre CL (2021) Percutaneous Revascularization Techniques. In: Maynar-Moliner M (Ed.), pp: 1-70.
-
Pérez de Isla L, de Isla LP, Fernández PLS, Walther LÁ- S, Alonso VB, et al. (2017) Comments on the 2016 ESC/ EAS guidelines on the treatment of dyslipidemias. Rev Esp Cardiol 70 (2):72-77.
-
Cheng SW, Ting AC, Lau H, Wong J (1999) Epidemiology of atherosclerotic peripheral arterial occlusive disease in Hong Kong. World J Surg 23(2): 202-206.
-
Sousa PP (2021) Analytical markers that condition the results of revascularization surgery in patients with peripheral arterial disease. Rev Angiología e Cirurgia Vascular / Publicação Official SPACV.
-
Cura F, Jozami S, Albertal M, Zaefferer P, Pfund G, et al. (2010) Treatment of critical limb ischemia. Rev Argent Cardiol 78(2): 129-133.
-
Kiwan G, Mohamedali A, Kim T, Zhuo H, Zhang Y, et al. (2022) The impact of clinical follow-up after revascularization on the outcomes of patients with chronic limb threatening ischemia. Ann Vasc Surg 86: 286-294.
-
Rubio JA, Jiménez S, Álvarez J (2017) Clinical characteristics and mortality of patients treated in a Multidisciplinary Diabetic Foot Unit. Endocrinol Diabetes Nutr 64(5): 241-249.
-
Sabatine MS, Giugliano RP, Keech AC, Honarpour N, Wiviott SD, et al. (2017) Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med 376(18): 1713-1722.
-
García RV, Tamayo CNT, Martínez YTG, Pacheco JB, González MEM (2017) Clinical and epidemiological characteristics of amputee patients at the General Hospital of Ciego de Ávila. Medi Ciego 23(4): 29-35.
-
Rodríguez Rodríguez Y, Rodríguez Mayoral JA (2020) Characterization of aortoiliac steno-occlusive disease. Rev Cuba Angiol Cir Vasc 21(2).
-
Talledo O, Valdez LM, Torres L, De la Peña O, Calle A (2021) Aorto-iliac occlusive disease: From surgical to endovascular treatment. Rev Medica Hered 26(3): 177.
-
Aday AW, Matsushita K (2021) Epidemiology of peripheral artery disease and polyvascular disease. Circ Res 128(12): 1818-1832.
-
Levin MG, Klarin D, Assimes TL, Freiberg MS, Ingelsson E, et al. (2021) Genetics of smoking and risk of atherosclerotic cardiovascular diseases: A Mendelian randomization study. JAMA Netw Open 4(1): e2034461.
-
Barrios V, Beato P, Brotons C, Campuzano R, Merino- Torres JF, et al. (2022) Comprehensive management of risk factors in peripheral vascular disease. Expert consensus. Rev Clin Esp (Barc) 222(2): 82-90.
-
Costa L de O, Fonseca WM, Reis Júnior NNA, Gomes GB, Gonçalves BCC, et al. (2020) Risk Factors related to patients hospitalized for Peripheral Arterial Disease. Minas Gerais Medical Rev 30(1): 1-8.
-
Flores Hernán M, Sabatel Pérez F, Martín Sierra C, García Camacho E, Robles Gamboa C (2017) Treatment protocol for ischemic heart disease in patients with vascular pathology. Medicine 12(37): 2256-2261.
-
Selvin E, Erlinger TP (2004) Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999-2000. Circulation 10(6):738- 743.
-
Troncoso-Pantoja C, Martínez-Sanguinetti MA, Ulloa N, Celis-Morales C (2020) Most cardiovascular diseases are attributed to risk factors that could be modified with lifestyle changes. Rev Med Chil 148(1): 126-128.
-
Mondragón-Zamora J, Marina López-de Dicastillo BP, Gutiérrez-Nistal M, Concepción-Rodríguez NA, David Zafra-Angulo J, et al. (2022) Outcomes and prosthesis procedure of major amputations in patients with peripheral arterial disease in our center. Angiology 74(6): 278-285.
-
Frank U, Nikol S, Belch J, Boc V, Brodmann M, et al. (2019) ESVM Guidelines on peripheral arterial disease. Vasa 48(S102): 1-79.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study
- The Hidden Impact of COVID-19 Lockdowns: A Study in Non COVID Venous Thromboembolism Cases-our Experience