Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
Introduction: Heart failure is a chronic disease that is one of the public health priorities of the World Health Organization. It represents the leading cause of unplanned hospitalizations. This study aimed to describe the epidemiological, diagnostic and evolutionary aspects of patients with heart failure admitted to the cardiology department of the Dalal Jamm national hospital. Patients and Methods: This was a retrospective study with descriptive and analytical aims over a period of 15 months from January 1, 2021 to March 31, 2022 at the cardiology department of Dalal Jamm National Hospital. The study focused on patients with heart failure, aged 18 years and above, hospitalized in the cardiology department during the study period. The data were analyzed using RStudio 4.6 software. Result: The prevalence of HF was 50.2%. The sex ratio was 0.64 and the mean age was 58.35±15.04 years. Fifty-two-point six percent (52.6%) of patients had a low socioeconomic level. Age was the most frequently found cardiovascular risk factor (80.3%). Dyspnea was the most common reason for consultation (95.8%). Decompensation factors were dominated by infections found in 20.4% of cases. The main electrocardiographic abnormalities were left ventricular hypertrophy and atrial fibrillation. Sixty percent of patients had heart failure with impaired ejection fraction. The etiologies of HF were dominated by dilated cardiomyopathy found (43.4%) followed by ischemic heart disease 25% and valvular heart disease 19.6%. Complications were noted in 6.3% including the occurrence of cardiogenic shock. The evolution was fatal in 13.1%. The causes of death were dominated by cardiogenic shock in 75% of cases. At discharge, 80.2% of patients were referred for day hospitalization. The average duration of hospitalization in the department was 8.77 ± 5.9 days (Figure 2). After 3 months of discharge 83.22% of patients were still stable, 11.30% were re-hospitalized and 5.5% died. Conclusion: Heart failure patients admitted to the cardiology department of the Dalal Jamm national hospital center are mostly women, the most common pathology is dilated cardiomyopathy and hospital mortality remains high.
Abbreviations
NYHA: New York Heart Federation; HF: Heart Failure; HBP: High Blood Pressure.
Introduction
Heart failure (HF) has been defined by the European Society of Cardiology as “a syndrome combining symptoms (dyspnea, ankle edema), sometimes with clinical signs (jugular vein turgor, pulmonary crackles), resulting from a structural or functional abnormality of the heart, which leads to a decrease in cardiac output or an increase in filling pressures during exercise or at rest”. It is a serious and frequent pathology whose progression is punctuated by numerous complications with a risk of sudden death at all stages. In addition, it constitutes a major public health issue due to its frequency, mortality, but also its morbidity as well as the significant medical and financial resources it absorbs [1].
It is a pathology that is part of the public health priorities of the World Health Organization. It affects approximately 64 million people worldwide and a 50% increase in hospitalizations for HF is expected over the next 25 years. At least 15 million Europeans are affected by this pathology, which remains the main cause of hospitalization for people over 65 years of age. It also represents the leading cause of unplanned hospitalizations [2, 3].
In Africa, heart failure is one of the main circumstances of discovery of cardiovascular diseases, moreover it faces an epidemiological transition marked by an emergence of cardiovascular pathologies. Its prevalence varies from one country to another; often only hospital data are available [4, 5, 6]. The THESUS-HF study, grouping together nine countries of sub-Saharan Africa, provided data on the extent of HF in this region of the globe and the expected unfavorable socio- economic impact [7]. The hospital prevalence of HF was 49.7%. The case fatality rate was 10.3%. This rate varies in the different African hospital series with 11.86% in Lomé, 9.03% in Yaoundé and 10.1% in Kano in Nigeria [8, 9, 10]. Nevertheless, it remains higher than those of higher income countries such as Morocco (6.1%) and France (7.5%) [11, 12].
The goal of this work was to describe the profile of heart failure patients hospitalized in the cardiology department of the Dalal Jamm National Hospital center.
Patients and Methods
This was a retrospective study with a descriptive and analytical aim over a period of 15 months from January 1, 2021 to March 31, 2022. Patient files were systematically recruited in the hospitalization unit of the cardiology department of the Dalal Jamm National Hospital. All heart failure patients, aged 18 years and over, admitted to hospital were included in the study. The data collected were sociodemographic, clinical, paraclinical, therapeutic and evolutionary hospital and in short term.
Parameters were collected on an Access questionnaire and the analysis was done with IBM SPSS software version 23. For quantitative variables, the results were described by their position and dispersion parameters; in numbers and percentage for qualitative variables.
Results
109 heart failure patient files were included. The hospital frequency was 50.2%. Forty-eight patients were male (39%) and 74 female (61%), the sex ratio was 0.64 and the mean age was 58.35 ± 15.04 years.
| CVRF | Number | Percentage % |
|---|---|---|
| Age | 98 | 80.3 |
| High blood pressure | 62 | 50.8 |
| Diabetes | 22 | 18 |
| Tobacco | 17 | 13.9 |
| Obesity | 16 | 13.9 |
| Dyslipidemia | 2 | 13.1 |
| Alcohol | 3 | 1.6 |
Table 1: Division of the study population according to the cardiovascular risk factor (N=122).
| Decompensation Factors | Number | Percentages % |
|---|---|---|
| No factor | 68 | 55.7 |
| Infection | 25 | 20.4 |
| Therapeutic interruption | 18 | 14.7 |
| Rhythm disorder | 13 | 10.6 |
| Acute coronary syndrome | 4 | 3.2 |
| Pulmonary embolism | 3 | 2.4 |
| Diet deviation | 2 | 1.6 |
| Anemia | 2 | 1.6 |
| Pregnancy | 1 | 0.8 |
| Conductive disorder | 3 | 2.4 |
| Etiologies | Number | Percentage % |
| Dilated cardiomyopathy | 53 | 43.4 |
| Ischemic heart disease | 30 | 25 |
| Valvular heart disease | 24 | 19.6 |
| Hypertensive heart disease | 4 | 3.3 |
| Toxic heart disease | 2 | 1.6 |
| Cardiothyreosis | 4 | 3.3 |
| Peripartum cardiomyopathy | 1 | 0.8 |
| Chronic cor pulmonale | 2 | 1.6 |
| Infective endocarditis | 1 | 0.8 |
| Pulmonary embolism | 1 | 0.8 |
Table 2: Division of the study population according to the decompensation factors (N=122).
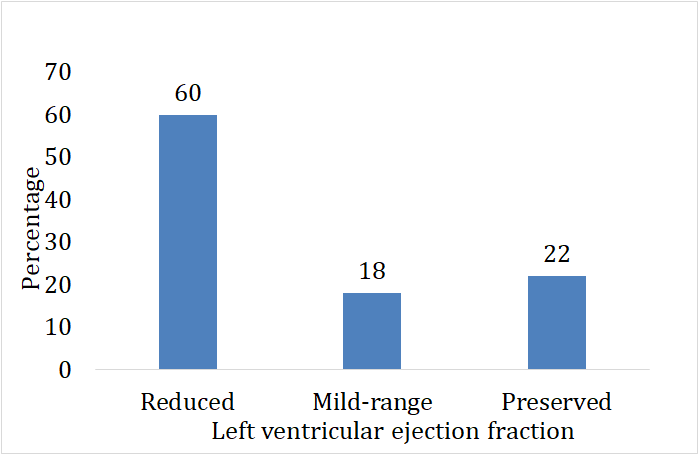
A low socioeconomic level was observed in 52.6% (n = 64) of patients. Age was the most common cardiovascular risk factor, found in 80.3% of patients followed by high blood pressure (HBP) (43.2%) and diabetes (19.9%) (Table 1). The association of HBP and diabetes was noted in 15.2% of cases. The main reason for consultation was dyspnea (95.8%) and two thirds (76%) had stage IV dyspnea according to the New York Heart Federation (NYHA) classification. The decompensation factors were dominated by infections found at 20.4% followed by therapeutic interruption 14.7% and rhythm disorders with 10.6% (Table 2). Anemia was recorded in 18% of patients and impaired renal function in 24.5%. Left ventricular hypertrophy was the main electrocardiographic abnormality (20.4%) and 13.1% of patients had atrial fibrillation. The mean left ventricular ejection fraction was 38.18±13.86%. Sixty percent of patients had heart failure with reduced ejection fraction with a mean of 28.52±13.75% (Figure 1). The etiologies were dominated by DCM found in 43.4% followed by ischemic heart disease (25%) and valvular heart disease found (19.6%) (Table 3). The majority of our patients were on loop diuretics (98.2%), anti-aldosterones (84.2%), beta-blockers and angiotensin converting enzyme inhibitors (63.7% each). In 80.6% of heart failure patients, the outcome was favorable during hospitalization with an improvement in signs.
Complications were noted in 6.3%, including the occurrence of cardiogenic shock. The outcome was fatal in 13.1% or 16 patients. The causes of death were dominated by cardiogenic shock in 75% of cases, followed by respiratory distress in 18.8%.
At discharge, 80.2% of patients were referred for day hospitalization, 17.9% for outpatient consultation and 1.9% were transferred. The average length of hospitalization in the department was 8.77 ± 5.9 days.
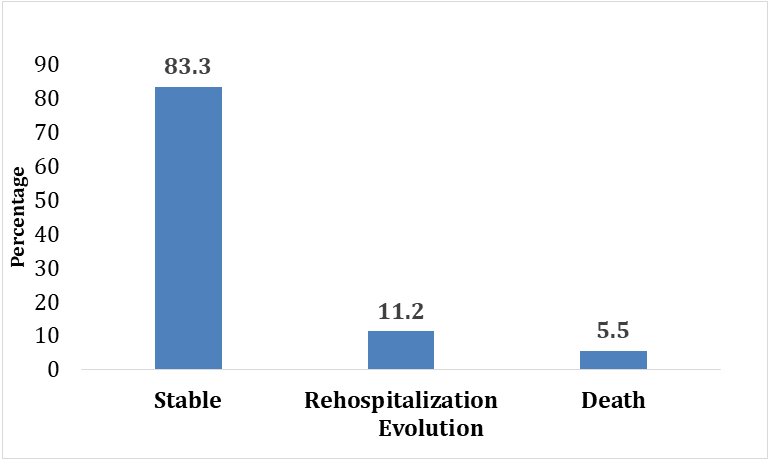
At 3 months of hospital discharge of the 106 patients, 83.2% were stable with 09 patients who were in NYHA stage 1, in stage II for 79 patients. 11.3% of patients were rehospitalized in the department and 5.5% passed away (Figure 2).
Discussion
Heart failure is the culmination of all heart diseases. Its prevalence is constantly increasing due to, on one hand, the aging of the population and, on the other hand, the increase in cardiovascular risk factors. In this series, the prevalence of heart failure is 50.2%. It is close to the prevalence found in hospitals in Burkina Faso and Dakar [13, 14].
The average age of patients was 58.7. This result is close to that of the multinational THESUS-HF study which found an average age of less than 60 years [7]. Our population is rather young compared to Western studies where the average age is over 60 years due to a higher life expectancy. The Senegalese population is mostly young and life expectancy at birth is around 67.4 years [15].
We noted a female predominance with a sex ratio of 0.64. The data are variable in the literature. This difference could be explained by the methodology used by the different authors. The National Agency of Statics and Demography in Senegal had found a percentage of men reporting suffering from a chronic disease lower than that observed in women [15].
The low socio-economic level was the most represented. This result is in line with the standard of living of the WAEMU member population, 49.4% of whom live below the poverty line [16]. In these countries, the emphasis should be placed on prevention and therapeutic education of patients to control cardiovascular risk factors.
The etiologies were dominated by DCM, ischemic and valvular heart disease. The high proportion of ischemic heart disease, which could be underestimated due to lack of exploration of DCM, confirms the notion of epidemiological transition in Africa. As for valvulopathies, they remain frequent because of the prevalence of acute rheumatic fever [17].
Infections and therapeutic interruption are by far the two most frequent decompensation factors in our study. These results are consistent with the data in the literature in terms of the prevalence of decompensation factors [18, 19, 20]. Therapeutic education helps prevent certain decompensation factors, in particular deviation from diet and therapeutic interruptions, and knowledge of decompensation factors is part of the educational objectives to be achieved [21].
The evolution was fatal in 13.1% which is close to the lethality found in the THESUS-HF study. The causes of death were dominated by cardiogenic shocks. Cardiogenic shock complicates approximately 5-10% of heart failures despite recent therapeutic advances [22]. According to Jones et al cardiogenic shock is the most deadly cardiovascular shock with 62.5% of deaths in his study [23].
More than three quarters of our patients had been called for day hospitalization after their discharge. This discharge method allows on the one hand to reduce the duration and cost of hospitalizations, on the other hand, it improves the efficiency of the use of hospitalization by reserving it for those who need it most.
This use of day hospital would explain the rate of short- term re-hospitalizations of the study lower than the data in the literature. The short-term mortality is comparable to the data of these studies [23, 24, 25].
Conclusion
With the epidemiological transition and the emergence of cardiovascular diseases, heart failure, the culmination of all these pathologies, is becoming more and more frequent in our regions. It would be necessary to optimize the management of cardiovascular risk factors to prevent it and promote therapeutic education in order to reduce acute episodes leading to hospitalization, which remains burdened by a still high mortality.
References
-
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, et al. (2021)ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 42(36): 3599‑3726.
-
Galinier M, Itier R, Fournier P, Delmas C, Roncalli J, et al. (2023) What’s new in heart failure?. Réalités Cardiologiques 357: 10-80.
-
Abassade P, Fleury L, Marty M, Cohen l, Fels A, et al. (2021) Epidemiological data from a cohort of patients hospitalized for heart failure. Single-center study over 3 years. Comparison with regional data. Ann Cardiol Angeiol 70(5): 294-298.
-
Ikama MS, Kimbally-Kaky G, Gombet T, Ellenga-Mbolla BF, Dilou-Bassemouka L, et al. (2008) Heart Failure in the Elderly in Brazzaville: Clinical, Etiological and Evolutionary Aspects. Med trop 68: 257-260.
-
Barry IS, Balde EY, Camara A, Samoura A, Koïvogui K, et al. (2020) Epidemiology and poor prognostic factors of heart failure in the cardiology department of the Ignace Deen National Hospital in Guinea. Cardiologie Tropicale 162.
-
Thiam M (2003) Insuffisance cardiaque en milieu cardiologique africain. Bull Soc Patholexot 96: 217-218.
-
Damasceno A, Mayosi BM, Sani M (2012) The causes, treatment, and outcome of acute heart failure in 1006 Africans from 9 countries. Arch Intern Med 172(18): 1386-1394.
-
Damorou F, Baragou S, Pio M, Afassinou YM, Pessinaba S, et al. (2014) Hospital-based morbidity and mortality from cardiovascular diseases in tropical areas: example of a hospital in Lomé (Togo). Pan Afr Med J 17: 62.
-
Kingue S, Dzudie A, Ménanga A (2005) A new look at adult chronic heart failure in Africa in the age of the Doppler echocardiography: experience of the medicine department at Yaounde General Hospital. Ann Cardiol Angeiol 54(5): 276-283.
-
Karaye KM, Sani MU (2008) Factors associated with poor prognosis among patients admitted with heart failure in a Nigerian tertiary medical centre: a cross-sectional study. BMC Cardiovasc Disord 8: 16.
-
Kheyi J, Benelmakki A, Bouzelmat H, Chaib A (2016) Epidemiology and management of heart failure in a Moroccan center. Pan Afr Med J 24: 85.
-
Gabet A, Lamarche-Vadel A, Chin F, Juillière Y, De Peretti, C, et al. (2014) Mortalité due à l’insuffisance cardiacaque en France, évolutions 2000-2010. Bull Epidémiol Hebd, pp: 386-394.
-
Jonas KK, Millogo GRC, Kambiré Y, Adoko H, Kagambéga LJ, et al. (2022) Heart Failure and Anemia in the Cardiology Department of the Yalgado Ouedraogo University Hospital: Epidemiological, Therapeutic and Prognostic Aspects: Heart failure and anemia in the cardiology department of the Yalgado Ouedraogo university teaching Hospital: epidemiology, management and prognosis. Health Sci Dis 23(2): 143-147.
-
Ngaide AA, Sow M, Gaye ND, Gnimbo B, Haris M, et al. (2020) Management and Etiological Profile of Heart Failure in a General Cardiology Department in Senegal: Cross- Sectional Study, Descriptive about 103 Cases. Ann Cardiol Cardiovasc Med 4(1): 1035.
-
Rapport des enquêtes (2023). Population data. ANSD.
-
UEMOA (2021) Program for the Harmonization and Modernization of Surveys on Household Living Conditions in UEMOA Member States. Union Économique Et Monétaire Ouest Africain.
-
Mirabel M (2019) Valvulopathies in sub-Saharan Africa. JE SFC.
-
Ngannou–Gnindjio I (2003) Heart failure in the African cardiology environment. Bull Soc Pathol Exot 96(3): 217-218.
-
Randriamihangy AN, Danielle MF, Rasamimanana NG, Andriamiharisoa S, Rakotoniaina MD, et al. (2020) Factors of decompensation in chronic heart failure at the Joseph Raseta Medical Academic Center Befelatanana, Antananarivo. Rev Anesth Réanim Med Urg Toxicol 12(1): 32-36.
-
Klip IT, Comin-Colet J, Voors AA, Ponikowski P, Enjuanes C, et al. (2013) Iron deficiency in chronic heart failure: an international pooled analysis. Am Heart J 165(4): 575- 582.
-
Bigot M (2021) Prise en charge globale de l’insuffisance cardiaque en réadaptation. Ann Cardiol Angeiol 61(1): 37-41.
-
Jovicic A, Holroyd-Leduc JM, Straus SE (2006) Effects of self-management intervention on health outcomes of patients with heart failure: a systematic review of randomized controlled trials. BMC Cardiovasc Disord 6: 43.
-
Jones NR, Roalfe AK, Adoki I, Hobbs FDR, Taylor CJ (2019) Survival of patients with chronic heart failure in the community: a systematic review and meta-analysis. Eur J Heart Fail 21(11): 1306-1325.
-
Jouini S, Manai H, Slimani O, Hedhli H, Hebaieb F, et al. (2019) Epidemiological and prognostic profile of acute heart failure: experience in the emergency department at the Charles Nicole Hospital of Tunis from 2013 to 2014. Pan Afr Med J 33: 251.
-
Adams KF, Fonaraww GC, Emermann CL, LeJemtel TH, Costanzo MR, et al. (2005) Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J 149(2): 209-216.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study
- The Hidden Impact of COVID-19 Lockdowns: A Study in Non COVID Venous Thromboembolism Cases-our Experience