Mitral Valve Replacement vs Mitral Valve Repair
Mitral regurgitation, mitral stenosis, and other types of mitral valve disease are very bad for heart health and usually need surgery to fix or replace the mitral valve. The study’s goal is to find deep differences and similarities between these two types of therapy. Repairing the mitral valve is the best option because the patient doesn’t have to take blood thinners for the rest of their lives, the original valve is kept, and the results are better in the long run and there are fewer problems. A number of repair methods are talked about, along with their uses and advantages. These include commissurotomy, annuloplasty, and leaflet or chordal repair. The mitral valve should be fixed whenever possible, but if that is not possible, it needs to be replaced in more advanced or complex cases. Both biological and mechanical replacement valves have pros and cons. The two biggest ones are the need for anticoagulant and how long they last. This study looks at these methods side by side and compares them in terms of how hard they are to operate on, how long they last, how many complications they have, and how well they work with patients. According to recent trends, mitral valve repair is still the best option, even though replacement is important for some groups of patients.
Introduction
The mitral valve, located between the left atrium and left ventricle, ensures blood flow. It controls the return of oxygenated blood from the left atrium to the left ventricle during cardiac contractions. Normal cardiac physiology requires the mitral valve to operate properly to circulate blood efficiently. Interference with its regular operation might cause pulmonary hypertension, arrhythmias, or heart collapse. A healthy mitral valve is essential for cardiac function. The mitral valve often develops stenosis and regurgitation. Mitral regurgitation occurs when an imperfectly closed mitral valve causes blood to flow backwards into the left atrium [1]. Since the heart works harder, palpitations, tiredness, and trouble breathing might follow. In mitral stenosis, the mitral valve aperture is narrow, forcing the heart to pump blood harder. Failure to treat either issue can harm a patient and raise the risk of death. Mitral valve repair or replacement is the principal treatment for these conditions. Mitral valve repair preserves the patient’s valve structure, while mitral valve replacement replaces the injured valve with a mechanical or biological valve. The patient’s condition, disease severity, and surgeon’s expertise determine which treatment to use. Each surgery has its own indications, pros, and cons.
Common Mitral Valve Diseases
Mitral valve diseases are among the most common heart valve disorders, with mitral regurgitation (MR) and mitral stenosis (MS) being the primary conditions affecting the mitral valve’s function.
Mitral Regurgitation (MR)
Blood overflows into the left atrium when the mitral valve fails to seal properly during left ventricle contraction, causing mitral regurgitation (MR). Due to backflow, the left atrium grows and weakens as it manages more blood. Long- term cardiac failure and left ventricular hypertrophy result from compensatory hypertrophy. Both acute and chronic MR exist, but chronic is more common [2]. Acute MR may result from a heart attack or trauma, unlike chronic MR, which develops over time due to preexisting conditions. There is no single mitral regurgitation cause. Mitral valve prolapse, a degenerative disease that weakens and bulges valve leaflets, is common. Untreated streptococcal infections can cause rheumatic heart disease, which scars and distorts the mitral valve, causing improper closure. MR can also result from valve-supporting muscle injury from coronary artery disease or a heart attack. Other causes include congenital defects and endocarditis. The clinical impact of magnetic resonance depends on sickness severity. Mild instances may initially have no symptoms. As the illness advances, individuals may have trouble breathing, excessive fatigue, abnormal heartbeats, and swollen legs. Chronic MR can cause atrial fibrillation, pulmonary hypertension, and congestive heart failure if untreated. Echocardiography is the gold standard for assessing valve function and regurgitation severity. It is frequently part of a diagnostic imaging investigation that also involves a physical exam to detect a heart murmur.
Mitral Stenosis (MS)
Mitral stenosis (MS) narrows the mitral valve, preventing blood flow from the left atrium to the left ventricle. Due to the bottleneck, left atrial pressure and pulmonary circulation increase, enlarging it. Reduced blood flow affects left ventricle blood flow, which lowers cardiac output and can lead to heart failure. Rheumatic fever, which inflames and damages the mitral valve after untreated strep throat, is the main cause of mitral stenosis. Scarring can thicken, fuse, and harden valve leaflets, shrinking the valve opening. Age-related valve calcification stiffens leaflets, causing mitral stenosis in elderly persons [3]. In rare cases, valve abnormalities might induce MS from birth. The severity of mitral stenosis impacts clinical outcomes. Mild MS individuals may not experience symptoms for years. However, as the condition progresses, dyspnea, especially with exertion, palpitations, fatigue, and atrial fibrillation can occur. In extreme cases, congestive heart failure and pulmonary hypertension can cause fluid retention, swollen legs, and shortness of breath. Mitral stenosis can cause left atrium blood clots, which raise stroke risk. Echocardiography evaluates the mitral valve pressure gradient and constricted valve for stenosis severity.
Mitral Valve Repair
Introduction to Mitral Valve Repair
Mitral valve repair is a surgical procedure for mitral regurgitation or stenosis. Mitral valve repair aims to restore normal valve function, preserve the valve’s structure, and ensure blood flow from the left atrium to the left ventricle. Mitral valve repair aims to preserve the patient’s native valve because it usually operates better than a new one. Keeping the natural tissue helps the heart function normally and reduces foreign element risks [4]. Mitral valve repair is often the first-line treatment for many reasons. Repairing instead of replacing improves longevity, quality of life, and complication rates, according to study. Repair does not require lifelong anticoagulant treatment, unlike mechanical valve replacements. In younger patients, bioprosthetic valve replacements survive less than repaired valves. The original valve tissue allows the heart to retain more of its native activities, which is vital to its long-term health.
Types of Mitral Valve Repair
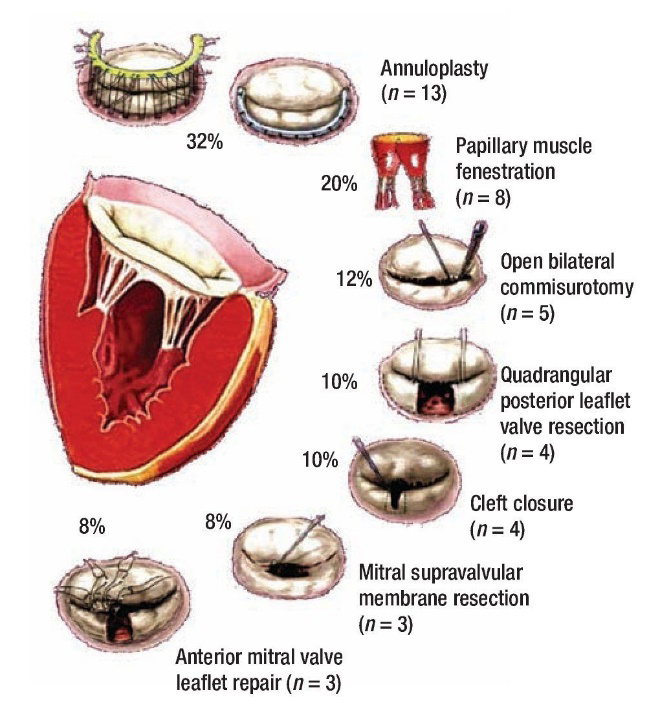
Several surgical techniques are used in mitral valve repair, depending on the specific pathology of the valve. The main types of repair procedures include: Annuloplasty: Annuloplasty, which implants a ring around the mitral valve annulus, is a common mitral valve repair treatment. Mitral valve annuli may enlarge or distort over time, especially with mitral regurgitation. The surgeon can place an annuloplasty ring to repair the valve’s leaflet closure and restore its size and shape [5]. Stabilising the annulus, reducing regurgitation, and preventing dilatation improve valve function after surgery. Commissurotomy: Mitral stenosis can fuse valve leaflets, requiring a commissurotomy. This surgery widens the valve aperture and separates fused leaflets to promote blood flow. Open-heart surgery or balloon catheter percutaneous commissurotomy are less invasive. This technique cures rheumatic mitral stenosis and restores valve blood flow. Leaflet Repair: Leaflet repair addresses mitral regurgitation, a typical complication of mitral valve leaflet abnormalities such too much or too little motion. Leaflet resection and plication increase valve closure by removing or folding and suturing the leaflet. Patients with mitral valve prolapse, where one or both leaflets are too moveable to close, often have this treatment. Chordal Replacement or Shortening: Chordae tendineae, slender fibrous cords, attach mitral valve leaflets to heart muscle. Too long or ruptured wires can halt the valve. Chordal repair replaces torn cords with Gore-Tex ones to restore tension and leaflet motion. You can also shorten existing chords to modify their length. Both treatments improve valve function and are used in degenerative mitral valve disease [6].
Indications for Repair
If the mitral valve is physically recoverable, mitral regurgitation and stenosis patients should have it repaired. Mitral valve prolapse and other degenerative mitral valve diseases are ideal for this operation because they restore valve leaflets and supporting components. Repair is also chosen in rheumatic heart disease if the damage is not too severe. Ischemic mitral regurgitation induced by coronary artery disease may be repaired depending on the valve and heart tissue damage. Repair is usually better for younger patients, those with less severe sickness, and those with good cardiac function because a repaired valve lasts longer. In severe cases of structural deterioration or calcification, valve replacement may be necessary [7].
Advantages of Mitral Valve Repair
Preserving the patient’s original mitral valve helps the heart to function normally, improving long-term benefits. This is essential because it maintains the valve’s dynamic, three-dimensional motion, which artificial valves cannot.
Repairing mitral valves reduces the risk of blood clots. Patients who receive valve repairs do not need blood thinners for life, unlike those who have mechanical valve replacements. This reduces anticoagulant issues like bleeding [8].
Mitral valve repair uses the patient’s own tissues, reducing the risk of endocarditis. In younger patients, a mended valve lasts longer than a tissue valve replacement, reducing future surgery.
Disadvantages of Mitral Valve Repair
Mitral valve repair is a complicated surgery that requires extensive expertise. Successful procedures depend largely on the valve pathology and the surgeon’s skill. No matter how diligent the expert is, the repair may not be enough to avoid reoperation or valve replacement. Serious calcification, leaflet damage, or extensive mitral disease may preclude repair. Changing the valve is usually the only option. In patients with severe rheumatic disease or ischemic mitral regurgitation, repair may be difficult or impossible.
Mitral valve repair is preferred by many mitral valve disease patients due to its pros and downsides, but it’s not for everyone [9]. Valve repair or replacement depends on the patient’s health, valve damage degree, and disease causation.
Mitral Valve Replacement
Introduction to Mitral Valve Replacement
When repair is impossible, mitral valve replacement involves surgical removal and prosthetic valve replacement. To restore normal blood flow between the left atrium and left ventricle, mitral valve replacement is performed instead of repair, which preserves native valve tissue. Replace the diseased valve with an artificial one. This surgery is frequently considered for severe mitral stenosis or regurgitation, where the valve structure is irreparably destroyed or calcified. Replacement may be needed if a patient’s valve pathology is too complicated or has failed many times. The only way to correct this and restart the heart is to replace the valve. The highly successful mitral valve replacement operation can enhance survival and clinical outcomes for patients with severe mitral valve dysfunction. The patient’s age, health, and lifestyle are among the many factors that determine mechanical or biological replacement valves [10].
Types of Mitral Valve Replacement
Mitral valve replacement involves two primary types of prosthetic valves: mechanical valves and biological (tissue) valves. Each type has its advantages and disadvantages, which are considered based on the patient’s individual needs. Mechanical Valves: Mechanical valves are made of carbon or metal to last. Due to their durability, these valves are ideal for younger patients or those seeking a long-term solution. Artificial valves increase blood clot risk. Mechanical valve patients must take warfarin permanently to lessen risk. This lifetime anticoagulant medicine raises bleeding risk and can cause problems with minor accidents or surgery. Patients are already busy enough without worrying about blood clotting (INR values) that must be monitored regularly. Biological Valves (Tissue Valves): Animal tissue, usually pig or cow, is used to make tissue valves. These valves work like the mitral valve, so you won’t need anticoagulants forever. Since clots are less frequent after tissue valve surgery, patients rarely need blood-thinning medicines. Because of this, biological valves may assist elderly or anticoagulant- intolerant patients. Biological valves last 10–15 years, less than mechanical valves. Over time, valve tissue degeneration can cause it to stop working and require a second surgery. Because of this, younger people may need multiple biological valve replacement surgeries. In older or shorter-lived patients, tissue valves are more durable and benefit them more.
Indications for Replacement
When substantial damage or calcification makes mitral valve repair impossible, the patient is usually advised to replace it. Severe mitral regurgitation or stenosis, especially with heart failure or pulmonary hypertension, warrants replacement. Patients with rheumatic heart disease may not be ideal candidates for repair due to damage complexity. This is because the valve commonly scars and calcifies. If a patient’s valve repairs have failed, replacement may be the only alternative [11]. This surgery is also suitable for patients with birth defects, bacterial endocarditis-damaged mitral valves, or cardiac attacks and ischemic mitral regurgitation.
Advantages of Mitral Valve Replacement
Mitral valve replacement benefits severe and complicated valve disease. Restoration is impractical for valves with considerable annulus or leaflet damage, therefore replacement is more reliable and long-lasting.
Due to their longevity and lifetime potential, mechanical valves are ideal for younger patients or those who cannot undergo repeated surgery. Due to their endurance, mechanical valves reduce the requirement for subsequent valve surgeries.
If valves are heavily calcified or malfunction after previous repairs, replacement is a long-term solution, especially if restoration is unlikely to succeed. Restoring valve function reduces heart failure symptoms like fatigue, edoema, and shortness of breath.
Disadvantages of Mitral Valve Replacement
Their main drawback is that mechanical valves require anticoagulation. Although these valves are durable, they increase bleeding risk since anticoagulants are needed to avoid blood clots. Patients must be careful since even minor injuries or treatments can create major problems.
Biological valves’ short lifespan is their main drawback. If the valve fails, patients, especially younger ones, may need repeated procedures to replace it. Later surgeries, especially in elderly patients, may be more difficult and hazardous.
Endocarditis is more likely with mechanical or biological valve replacement than with native valves. Valve thrombosis and failure from normal wear and tear are more risky with mechanical prosthetic valves [12].
Comparison of Mitral Valve Repair and Replacement
Repairing or replacing the mitral valve depends on age, health, valve sickness, and surgeon expertise. Both procedures have pros and cons, and some mitral valve diseases respond better to one than the other. This comparison will consider surgical difficulty, length, complication rates, patient fit, and treatment trends (Table 1).
| Success Rate | Risks | Longevity | Anticoagulation Need | Suitable Patient Population | |
|---|---|---|---|---|---|
| Mitral Valve Repair | 90-95% | Lower risk of thromboembolism and infection | Durable with low reoperation rates | No | Younger patients, patients with degenerative valve disease |
| Mitral Valve Replacement (Mechanical) | 95% | Risk of anticoagulation-related bleeding and thromboembolism | Lifelong durability | Yes (lifelong) | Younger patients needing long-lasting valves |
| Mitral Valve Replacement (Biological) | 85-90% | Potential degeneration requiring reoperation | 10-15 years (typically) | No | Older patients, patients unable to take anticoagulants |
Table 1: Comparison of Mitral Valve Repair and Replacement.
Surgical Complexity and Risk
Repairing a mitral valve usually takes more technical expertise than replacing it. The surgeon may bend, tighten, or reinforce valve components like chordae or leaflets to restore valve architecture and function. Due to their precision, repair surgeries require skilled surgeons. However, expert valve repair yields better long-term results with fewer issues. Mitral valve replacement is often simpler surgically, especially in severe valve disease or calcification. A valve replacement surgery replaces the damaged valve with a mechanical or biological prosthetic valve. Replacing a valve is easier than mending it, but it has long-term risks include prosthetic valve deterioration in biological valves and lifelong anticoagulation in mechanical valves. Despite being more difficult, repairing something is usually safer than replacing it. Replacing a faulty valve can cause anticoagulant-related bleeding in mechanical valves or re-operation in biological valves, although it may be required.
Durability and Longevity
Mechanical mitral valves are known for their 20-year endurance. This makes them an excellent choice for younger individuals who may need many surgeries. It requires lifelong anticoagulation, which can cause bleeding or thrombosis if not controlled properly. Biological (tissue) valves are superior for older or blood thinner-intolerant patients because they do not require anticoagulants. However, biological valves degenerate after 10–15 years, therefore younger patients may need a second valve replacement. Mitral valve replacement often eliminates the requirement for lifelong anticoagulant therapy [13]. Preserving the restored valve’s native anatomy ensures its natural operation, reducing prosthetic device risks. Because thrombosis and reoperation are less likely, many surgeons repair rather than reoperate.
Complication Rates
Mitral valve repair reduces the incidence of infections and thromboembolisms compared to valve replacement. The native valve is intact; thus patients do not need anticoagulation unless they have atrial fibrillation, reducing bleeding risk. Long-lasting mechanical valve replacement raises the risk of thromboembolic events since anticoagulation medicine must be used forever. Mechanical valve patients are more likely to develop life-threatening valve thrombosis and haemorrhage. Despite a lower risk of thrombosis without anticoagulation, biological valves are more likely to degenerate and require reoperation. Patients with significantly damaged mitral valves can replace them, although it has a larger risk of problems than repair. The patient’s situation and mitral valve condition are key factors in choosing between these surgeries.
Patient Suitability and Outcomes
The patient’s age, health, and valve sickness determine whether mitral valve repair or replacement is best. Valve repair is better for younger and less severe valve disease patients because it avoids artificial valves and lifelong anticoagulation. Repair is beneficial for degenerative mitral valve disease patients because it restores normal valve function while preserving valve structure. For older or complex mitral valve disease patients, mitral valve replacement may be best [3].
The elderly may be better candidates for a biological valve, which removes the need for anticoagulation, reduces bleeding, and reduces deterioration. Repair usually has fewer difficulties and higher survival rates than replacement, especially in experienced institutions. Studies show that restoring the mitral valve increases long-term survival, quality of life, and problems.
Current Trends in Treatment Choices
Repairing the mitral valve instead of replacing it has grown in popularity, especially at skilled surgery centres. Because repair yields better results and fewer complications than other treatments, most mitral regurgitation patients, especially those with degenerative valve disease, should choose it first. Mitral valve replacement is still possible for those with irreversible severe valve disease. When repair is impossible, such as in badly calcified valves or rheumatic heart disease, valve replacement is preferred. Studies show that mending the mitral valve instead of replacing it increases long-term life and minimises complications. Repairs reduce the need for a second treatment, unlike biological valve replacements, which degrade over time.
Finally, mitral valve disease treatment requires valve repair and replacement. If the valve is irreparable, replacement is required. Repair is usually better since it lasts longer, has fewer difficulties, and yields better outcomes. Best approach depends on surgical team skill, patient condition, and valve pathology. Even though recent advances support repair, difficult or severe sickness patients still need replacement.
Conclusion
Mitral valve disease management requires repair and replacement. Both approaches have pros and cons. The surgeon’s experience, patient preferences, and valve condition will determine the best option. Mitral valve repair is preferred for mitral regurgitation because surgery preserves the original valve, maintains cardiac function, and has better long-term outcomes with fewer problems. Repair decreases thrombosis, infection, and anticoagulation, thus many patients, especially younger ones, choose it over anticoagulation. Mitral valve replacement is indicated when calcification, rheumatic illness, or valve injury prevent restoration. Mechanical valves are long-lasting but require lifetime anticoagulation, biological valves flow more naturally but degenerate over time, and replacement solves problems. Current data shows that mitral valve repair is more common than replacement in specialised centres, especially for degenerative diseases. Studies show that repair, not replacement, improves long-term survival, quality of life, and problems. The patient’s condition and center’s experience frequently impact operation selection. Repair is more common at high-volume institutions with skilled surgeons due to better results. Replacement is still the best operation for severely ill patients when repair is impossible or unlikely. For difficult valve illness or older patients who cannot re- operate, biological valve replacement is favoured despite its short lifespan. Because it doesn’t need anticoagulation. To conclude, mitral valve replacement is still necessary for patients with more severe conditions, even though repair may be optimal for some due to its long-term benefits and lower complication rates. Treatment should take into account the surgeon’s ability, the patient’s condition, and the valve damage’s severity. Minimally invasive and transcatheter mitral valve surgery may lead to less invasive and longer- lasting treatments.
References
-
Acker MA, Parides MK, Perrault LP, Moskowitz AJ, Gelijns AC, et al. (2014) Mitral-valve repair versus replacement for severe ischemic mitral regurgitation. New England Journal of Medicine 370(1): 23-32.
-
Madesis A, Tsakiridis K, Zarogoulidis P, Katsikogiannis N, Machairiotis N, et al. (2014) Review of mitral valve insufficiency: repair or replacement. Journal of thoracic disease 6(S1): S39.
-
Pozzoli A, De Bonis M, Alfieri O (2016) Mitral valve repair. F1000Research pp: 5.
-
Chikwe J, Toyoda N, Anyanwu AC, Itagaki S, Egorova NN, et al. (2017) Relation of mitral valve surgery volume to repair rate, durability, and survival. Journal of the American College of Cardiology 69(19): 2397-2406.
-
Seese LM, Sultan I, Gleason TG, Wang Y, Thoma F, et al. (2020) Outcomes of mitral valve repair versus replacement in the elderly. The Annals of Thoracic Surgery 109(4): 1202-1209.
-
Veerappan M, Cheekoty P, Sazzad F, Kofidis T (2020) Mitral valve re-repair vs replacement following failed initial repair: a systematic review and meta-analysis. Journal of Cardiothoracic Surgery 15: 1-9.
-
Zhou S, Egorova N, Moskowitz G, Giustino G, Ailawadi G, et al. (2021) Trends in MitraClip, mitral valve repair, and mitral valve replacement from 2000 to 2016. The Journal of thoracic and cardiovascular surgery 162(2): 551-562.
-
Fan Q, Li X, Cao G, Yu P, Zhang F (2021) Outcome of mitral valve repair or replacement for non-ischemic mitral regurgitation: a systematic review and meta- analysis. Journal of Cardiothoracic Surgery 16: 1-10.
-
Brescia AA, Watt TM, Murray SL, Rosenbloom LM, Kleeman KC, et al. (2022) Rheumatic mitral valve repair or replacement in the valve-in-valve era. The Journal of thoracic and cardiovascular surgery 163(2): 591-602.
-
Di Tommaso E, Rapetto F, Guida GA, Zakkar M, Bruno VD (2021) Benefits of mitral valve repair over replacement in the elderly: a systematic review and meta‐ analysis. Journal of Cardiac Surgery 36(7): 2524-2530.
-
Badhwar V, Chikwe J, Gillinov AM, Vemulapalli S, O’Gara PT, et al. (2023) Risk of surgical mitral valve repair for primary mitral regurgitation. Journal of the American College of Cardiology 81(7): 636-648.
-
He K, Song J, Luo H, Su H, Liang W, et al. (2022) Valve replacement or repair in native mitral valve infective endocarditis—Which is better? A meta‐analysis and systematic review. Journal of Cardiac Surgery 37(4): 1004-1015.
-
Ludwig S, Kalbacher D, Ali WB, Weimann J, Adam M, et al. (2023) Transcatheter mitral valve replacement or repair for secondary mitral regurgitation: a propensity score‐ matched analysis. European journal of heart failure 25(3): 399-410.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study
- The Hidden Impact of COVID-19 Lockdowns: A Study in Non COVID Venous Thromboembolism Cases-our Experience