Study of Prognostic Role of High Sensitivity C - Reactive Protein and Serum Fibrinogen Levels in Unstable Angina Patients in Eastern India
Introduction: Patients with unstable angina are heterogeneous in terms of risk of cardiac death and nonfatal ischemic events. Assessment of the prognosis in these individuals guides the management protocol. C - reactive protein (CRP) and serum fibrinogen are established prognostic markers in UA. Aim: This study assessed the prognostic role of high sensitivity CRP (hs CRP) and serum fibrinogen levels in unstable angina patients in eastern India with no other high risk factors. Material and methods: It was a prospective single centre observational study which included patients admitted with diagnosis of unstable angina in medical ICU from August 1, 2009 to June 1, 2011. Cases with concomitant inflammatory or neoplastic condition, valvular heart disease, left ventricular (LV) failure, ST elevation/ new or presumably new ST depression and T wave inversion in ECG, elevated cardiac biomarkers (CPK MB/ Troponin T), LV dysfunction (LVEF60 years, known case of coronary artery disease, heart failure, diabetes, hypertension, dyslipidemia and chronic kidney disease were excluded from the study. Patients were observed for 72 hours in medical ICU. Serum fibrinogen and high sensitivity C - reactive protein (hs CRP) levels were estimated at the time of admission, and at the end of 48 hours and 72 hours. Primary endpoints were death, myocardial infarction, heart failure and secondary endpoints were hemodynamically unstable ventricular arrhythmias, and refractory angina or recurrent angina. Patients who met the study endpoints were grouped as unfavourable group and others as favourable group. Results: Of 1034 patients with unstable angina, 927 met the exclusion criteria and 7 were lost on follow up. On follow up, 30 (30%) patients were in unfavourable group and 70(70%) were in favourable group. Primary endpoints were met in 9% patients, death- 1(1%), myocardial infarction- 3 (3%), heart failure- 5 (5%). Secondary endpoints were met in 21% patients, ventricular arrhythmias- 4 (4%), refractory angina- 17 (17%). Patients in recurrent angina 10 (10%). Patients in unfavourable group had significantly high hs CRP (4.47±1.22 mg/L vs 1.98±0.37 mg/L, p3mg/L and serum fibrinogen level >600mg/dl. Conclusion: High sensitivity C - reactive protein and serum fibrinogen levels at admission were independent prognostic markers of adverse hospital outcome in unstable angina patients. These markers can be useful in risk stratification of patients with unstable angina and early referral to cardiac care centre for destination curative therapy.
Introduction
Patients with unstable angina are heterogeneous in terms of risk of cardiac death and nonfatal ischemic events. Assessment of the prognosis in these individuals guide the initial evaluation and treatment in terms of selection of the site of care (coronary care unit, monitored step-down unit, or outpatient setting), selection of therapy, including platelet glycoprotein (GP) IIb/IIIa inhibitors and invasive management strategy. Risk scores like TIMI, GRACE, PURSUIT regroup markers of the acute thrombotic process and other markers of high risk to identify high-risk patients with UA [1, 2, 3, 4, 5, 6, 7]. Inflammation characterizes all phases of atherosclerosis and can play a major role in plaque instability [8]. Inflammatory markers like C - reactive protein (CRP) and serum fibrinogen are established prognostic markers in UA [9, 10, 11]. We undertook this study to assess the prognostic role of high sensitivity CRP (hs CRP) and serum fibrinogen levels in unstable angina patients in eastern India with no other high risk factors (diabetes, hypertension, age >60 years, dyslipidemia, chronic kidney disease, ECG changes, elevated biomarkers, known case of coronary artery disease, heart failure).
Methods
It was a prospective single centre observational study which included patients admitted in medical ICU from August 1, 2009 to June 1, 2011 with the diagnosis of unstable angina after meticulous screening in the emergency department (ED). We included patients aged 30 to 60 years who presented to the ED with symptoms suggestive of unstable angina. Unstable angina was defined as angina pectoris (or equivalent type of ischemic discomfort) with at least one of three features: (1) occurring at rest (or minimal exertion) and usually lasting >20 minutes (if not interrupted by the administration of a nitrate or an analgesic); (2) being severe and usually described as frank pain; or (3) occurring with a crescendo pattern (i.e., pain that awakens the patient from sleep or that is more severe, prolonged, or frequent than previously) [12]. Other data of interest included sociodemographic information, electrocardiographic (ECG) findings, serial creatine kinase MB (CK-MB)/ troponin T and echocardiography. Cases with concomitant inflammatory or neoplastic condition, valvular heart disease, left ventricular (LV) failure, ST elevation/ new or presumably new ST depression and T wave inversion in ECG, elevated cardiac biomarkers (CPK MB/ Troponin T), LV dysfunction (LVEF<50%), suspected pulmonary thromboembolism, age>60 years, known case of coronary artery disease, heart failure, diabetes, hypertension, dyslipidemia and chronic kidney disease were excluded from the study.
Study Protocol
All patients were evaluated with a detailed history and clinical examination. Other data of interest included socio demographic information, electrocardiographic (ECG) findings, serial creatine kinase MB (CK-MB)/ troponin T, renal function test and echocardiography. All patients who satisfied the study criteria were observed for 72 hours in medical ICU and managed according to ACC/
AHA guidelines (2007) for unstable angina. Serum fibrinogen and high sensitivity C-Reactive Protein (hs CRP) levels were estimated at the time of admission and again at the end of 48 hours and 72 hours. Level of inflammatory markers were classified as low (hs CRP <1mg/L and serum fibrinogen ≤500 mg/dl), intermediate (hsCRP 1 to 3 mg/L or serum fibrinogen 501-600 mg/dl ) and high (hsCRP >3 mg/L or serum fibrinogen >600 mg/dl) high (>600 mg/dl). Primary endpoints were death, myocardial infarction, heart failure and secondary endpoints were hemodynamically unstable ventricular arrhythmias, refractory angina or recurrent angina. Patients who met the primary or secondary study endpoints were grouped as unfavourable group and others as favourable group.
Laboratory Analysis
hsCRP: The hsCRP was measured quantitatively by turbid metric test using kits. Latex particles coated with specific anti-human CRP were agglutinated when mixed with samples containing CRP. The agglutination caused an absorbance change depending upon the CRP content in the sample. The absorbance change was quantified using calibrators of known CRP concentration (calibration curve). The linearity of the method was up to 10 mg/L. All the samples having values >10 mg/L were diluted further and reanalyzed. The intra assay coefficient of variation was < 5% and inter-assay coefficient was<10%. Serum fibrinogen: Fibrinogen level was analyzed quantitatively by rate nephelometry with a Beckman Array protein system (Beckman Instruments). The assay was performed according to recommendations of the manufacturer except that goat anti-human fibrinogen (Atlantic Antibodies) was used. The assay was calibrated against a human plasma standard (Behring).
Statistical Analysis
Statistical analysis was done using SPSS 20 software. Continuous variables were expressed as mean ± SD, and categorical variables were presented as absolute number and proportion (%).Data were analyzed using the 2-tailed test to identify differences between groups and analysis of variance (ANOVA) for repeated measures. Nominal data was analyzed by the chi square test. We considered 95% confidence intervals (CIs) that excluded unity, or, equivalently, p < 0.05, as statistically significant. ANOVA was used to compare serum fibrinogen and high sensitivity C-Reactive Protein amongst themselves to ascertain whether their levels were rising or returning to baseline. ANOVA was also used to compare the levels of serum fibrinogen and high sensitivity C - reactive protein with the prognosis of unstable angina.
Results
Of 2765 patients who presented with chest pain in the ED, 1034 had unstable angina. 927 patients met the exclusion criteria and were excluded from the study (Figure 1). 7 patients were lost on follow up and excluded. Data of remaining 100 patients was analyzed. Mean age of the study group was 53 ± 6 years and 51% patients were female. On follow up 30 (30%) patients were in unfavourable group and 70% in favourable group. Primary endpoints were met in 9% patients, death- 1(1%), myocardial infarction- 3 (3%), heart failure- 5 (5%). Secondary endpoints were met in 21% patients, ventricular arrhythmias- 4 (4%), refractory angina or recurrent angina 17 (17%).
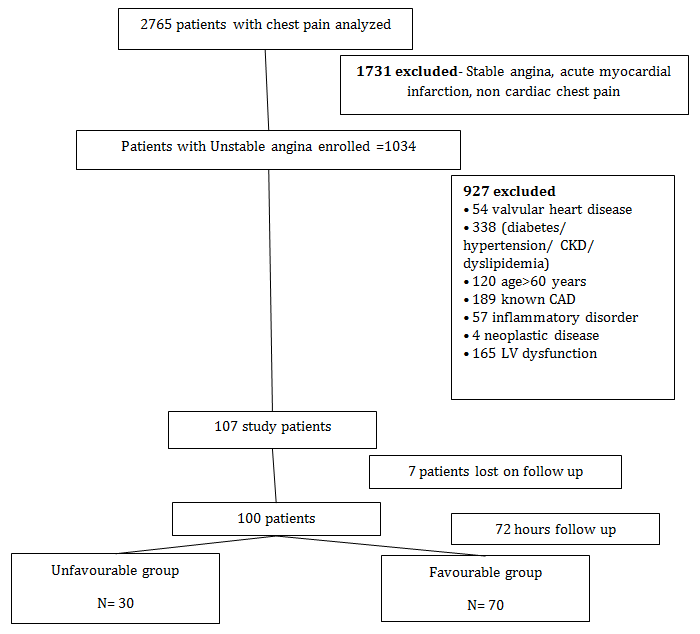
Figure 1: Flow of patients in the study. Patients with low level of inflammatory markers (hsCRP levels <1 mg/L and serum fibrinogen ≤500mg/dl) at the time of admission had favourable outcome while those with high level of inflammatory markers (hsCRP >3 mg/ L or serum fibrinogen > 600mg/dl) had unfavourable outcome. 83.78% of patients with intermediate level of inflammatory markers (hs CRP 1 to 3 mg/L or serum fibrinogen level >600 mg/dl) at admission had favourable outcome while 16.22% had unfavourable outcome (Table 1). 16.67% of patients with hs CRP between 1 to3mg/L and 40% with serum fibrinogen between 501 to 600 mg/dl had unfavourable outcome. Those with unfavourable outcome, showed increasing trend of hsCRP and serum fibrinogen, so that by the end of 72 hours they had hsCRP level >3mg/L and serum fibrinogen level >600mg/dl (Table 2). Patients in unfavourable group had significantly high hs CRP (4.47±1.22 mg/L vs 1.98±0.37 mg/L, p<0.0001) and serum fibrinogen (600.93 ±49.94 mg/ dl vs 404.1 ±94.01mg/dl, p<0.0001) levels at the time of admission (Table 3).
| Inflammatory markers | At admissio | n | Favourable group (%) | Unfavourable group (%) | p value | ||||||||
| Low (hs CRP<1mg/L and fibrinogen ≤500mg/dl) | 38 | 38 (100) | 0 | <0.0001 | |||||||||
| Intermediate (hs CRP 1to 3 mg/L or fibrinogen 501 to 600 mg/dl) | 37 | 31(83.78) | 6(16.22) | <0.0001 | |||||||||
| High (hs CRP >3 mg/L or fibrinogen >600 mg/dl | 25 | 01 (04) | 24(96) | <0.0001 |
Table 1: Comparison of outcome in patients of unstable angina according to low, intermediate and high levels of inflammatory mark
| At admission | At 48 hours | At 72 hours | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Favourable group (%) | Unfavourable group (%) | p value | Favourable group (%) | Unfavourable group (%) | p value | Favourable group (%) | Unfavourable group (%) | p value | |||||||||||||
| hs CRP (in mg/L) | <1 | 40(57.14) | 0 | <0.0001 | 67(95.71) | 0 | <0.0001 | 70(100) | 0 | <0.0001 | |||||||||||
| 1 to 3 | 30(42.86) | 6(20) | <0.0001 | 3(4.29) | 2(6.67) | 0.0012 | 0 | 0 | 0 | ||||||||||||
| >3 | 0 | 24(80) | <0.0001 | 0 | 28(93.33) | <0.0001 | 0 | 30(100) | <0.0001 | ||||||||||||
| Serum fibrinogen (in mg/dl) | ≤500 | 55(78.57) | 0 | <0.0001 | 70(100) | 0 | <0.0001 | 70(100) | 0 | <0.0001 | |||||||||||
| 501- 600 | 15(21.43) | 10(33.33) | 0.0450 | 0 | 5(16.67) | <0.0001 | 0 | 0 | 0 | ||||||||||||
| >600 | 0 | 20(66.67) | <0.0001 | 0 | 25(83.33) | <0.0001 | 0 | 30(100) | <0.0001 |
Table 2: Distribution of hs-CRP and serum fibrinogen in favourable and unfavourable group of patients at admission, 48 hours and
| Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Favourable group (n=70) | Unfavourable group (n=30) | p value | ||||||||
| hs CRP (in mg/L) | 1.98±0.37 | 4.47±1.22 | <0.0001 | |||||||
| Serum fibrinogen (in mg/dl) | 404.1 ±94.01 | 600.93 ±49.94 | <0.0001 |
Table 3: Comparison of mean value of hs CRP and serum fibrinogen between favourable and unfavourable groups at the time of admiss
Discussion
As epidemic of coronary artery disease continues to hit the globe, hunt for newer diagnostic, therapeutic and prognostic tools also expedites. Despite improved treatment of unstable coronary artery disease during the past decade, there remains a substantial risk of new ischemic events during the first months after the acute episode [11]. Inflammation has a key role in the pathophysiology of entire spectrum of atherosclerotic coronary artery diseases ranging from stable ischemic heart disease to acute coronary syndrome. Increased concentrations of acute phase proteins, such as fibrinogen and C-reactive protein are associated with poor prognosis in unstable coronary artery disease [13, 14]. Unstable coronary artery disease is a heterogeneous syndrome. A
plaque fissure could be visualized by angioscopy in ~65% of the individuals with unstable angina [15, 16]. Increased troponin levels might be a tool for selecting individuals at greater risk (i.e, patients with plaque fissure and subsequent thrombus formation) and hence with a greater susceptibility to increased fibrinogen concentrations [17]. Furthermore, increased plasma viscosity, which is mainly determined by fibrinogen levels, indicates an unfavourable outcome in patients with unstable angina [18]. This negative influence of increased viscosity might be more pronounced in patients with a decreased vessel lumen because of a mural thrombus. CRP leads to decreased expression of nitric oxide by endothelial cells and increase complement activation, thus leading to myocardial and vascular damage. Current study also showed increased in hospital adverse outcome in unstable angina patients with elevated hs CRP and serum fibrinogen levels. These markers predicted poor prognosis without any relation to the other high risk factors. Some of our results are therefore consistent with sub study of the Thrombolysis in Myocardial Infarction (TIMI) IIIB, FRISC, TIMI 11A trial, in which elevated fibrinogen or CRP levels were associated with spontaneous, in-hospital ischemic episodes in the subgroup of patients with unstable angina [4, 11, 19, 20]. In accordance to PROVE IT TIMI 22 trial, high hs CRP was related to adverse cardiac events in the current study but in contrary to it, our study did not assess long term prognostic value of this inflammatory marker [21].
Study Limitation
First, it was a single centre study and only a small number of patients (n=100) were studied. Larger studies are needed to validate the results. Second, Coronary angiography findings, number of vessels involved and type of lesions were not taken into account which have important relation to outcome. Third, Plaque morphology which is very closely related to inflammatory mediators was also not taken into account. Fourth, as other high risk factors were excluded, role of these markers whether additive to other high risk factors cannot be highlighted from this study. Lastly, study was only confined to in hospital adverse events during 72 hours of hospital stay and relation of these markers to short or long term prognosis could not be established by this study.
Conclusion
High sensitivity C - reactive protein and serum fibrinogen levels at admission were independent prognostic markers of in hospital adverse outcome in unstable angina patients. These markers can be useful in risk stratification of unstable angina patients at primary care centre. So these high risk patients can be referred to advanced cardiac care centres for early invasive therapy.
References
-
Antman EM, Cohen M, Bernink PJ, McCabe CH, Horacek T, et al. (2000) The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 284(7): 835-836.
-
Granger CB, Goldberg RJ, Dabbous O, Pieper KS, Eagle KA, et al. (2003) Predictors of hospital mortality in the global registry of acute coronary events. Arch Intern Med 163(19): 2345-2348.
-
Sabatine MS, Morrow DA, de Lemos J, Gibson CM, Murphy SA, et al. (2002) Multimarker approach to risk stratification in non-ST elevation acute coronary syndromes: Simultaneous assessment of troponin I, C-reactive protein, and B-type natriuretic peptide. Circulation 105(15): 1760-174.
-
(1994) Effects of tissue plasminogen activator and a comparison of early invasive and conservative strategies in unstable angina and non-Q wave myocardial infarction: results of the TIMI IIIB Trial. Thrombolysis in Myocardial Ischemia. Circulation 89: 1545-1556.
-
Savonitto S, Ardissino D, Granger CB, Morando G, Prando MD, et al. (1999) Prognostic value of the admission electrocardiogram in acute coronary syndromes. JAMA 281(8): 707-713.
-
Chang WC, Boersma E, Granger CB, Harrington RA, Califf RM, et al. (2004) Dynamic prognostication in non-ST-elevation acute coronary syndromes: insights from GUSTO-IIb and PURSUIT. Am Heart J 148(1): 62- 71.
-
Ho KT, Miller TD, Hodge DO, Bailey KR, Gibbons RJ (2002) Use of a simple clinical score to predict prognosis of patients with normal or mildly abnormal resting electrocardiographic findings undergoing evaluation for coronary artery disease. Mayo Clin Proc 77(6): 515-521.
-
Buffon A, Biasucci LM, Liuzzo G, D'Onofrio G, Crea F, et al. (2002) Widespread coronary inflammation in unstable angina. N Engl J Med 347(1): 5-12.
-
Zairis MN, Papadaki OA, Manousakis SJ, Thoma MA, Beldekos DJ, et al. (2002) C-reactive protein and multiple complex coronary artery plaques in patients with primary unstable angina. Atherosclerosis 164(2): 355-359.
-
Morrow DA, de Lemos JA, Sabatine MS, Wiviott SD, Blazing MA, et al. (2006) Clinical relevance of C- reactive protein during follow-up of patients with acute coronary syndromes in the Aggrastat-to-Zocor Trial. Circulation 114(4): 281-288.
-
FRISC Study Group (1996) Low-molecular-weight heparin during instability in coronary artery disease. Lancet 347(9001): 561-568.
-
Anderson JL, Adams CD, Antman EM, Antman EM, Bridges CR, et al. (2007) ACC/ AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction: Executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 116: 803-877.
-
Berk B, Weintraub W, Alexander W (1990) Elevation of C-reactive protein in 'active' coronary artery disease. Am J Cardiol 65(3): 168-172.
-
Swahn E, von Schenk H, Wallentin L (1989) Plasma fibrinogen in unstable coronary artery disease. Scand J Clin Lab Invest 49(1): 49-54.
-
Silva J, Escobar A, Collins T, Ramee S, White C (1995) Unstable angina: a comparison of angioscopic findings between diabetic and nondiabetic patients. Circulation 92(7): 1731-1736.
-
Feyter P, Ozaki Y, Baptista J, Escaned J, Di Mario C, et al. (1995) Ischemia related lesion characteristics in patients with stable or unstable angina. Circulation 92: 1408-1413.
-
Lindahl B, Venge P, Wallentin L (1996) Relation between troponin T and the risk of subsequent cardiac event in unstable coronary artery disease. Circulation 93: 1651-1657.
-
Neumann FJ, Katus H, Hoberg E, Roebruck P, Braun M, et al. (1991) Increased plasma viscosity and erythrocyte aggregation: indicators of an unfavourable clinical outcome in patients with unstable angina pectoris. Br Heart J 66(6): 425-430.
-
Tracy R, Bovil E, Yanez D, Psaty B, Fried L, et al. (1995) Fibrinogen and factor VIII, but not factor VII, are associated with measures of subclinical cardiovascular disease in the elderly. Arterioscler Thromb Vasc Biol 15(9): 1269-1279.
-
Morrow DA, Rifai N, Antman EM, Weiner DL, McCabe CH, et al. (1998) C-Reactive protein is a potent predictor of mortality independently of and in combination with troponin T in acute coronary syndromes: a TIMI 11A substudy. J Am Coll Cardiol 31(7): 1460-1465.
-
Ridker PM, Morrow DA, Rose LM, Rifai N, Cannon CP, et al. (2005) Relative efficacy of atorvastatin 80 mg and pravastatin 40 mg in achieving the dual goals of low-density lipoprotein cholesterol < 70 mg/dl and C- reactive protein <2 mg/L: an analysis of the PROVE- IT TIMI-22 trial. J Am Coll Cardiol 45(10): 1644-1648.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study