Evaluation of Syncope: Who Needs an Implantable Loop Recorder?
Syncope is a frequently encountered condition and accounts for up to 3% of emergency department consultations and 6% of hospital admissions. Although clinical history and examination combined with laboratory testing are adequate in obtaining a diagnosis in many patients, there are some who experience infrequent episodes that are elusive in nature and the cause difficult to detect. This is because correlation between syncopal events and any alteration of physiological signals (ECG, blood pressure) is the “gold standard†for the diagnostic work-up. In these individuals, prolonged ambulatory monitoring with implantable electrocardiographic recorders can be of great benefit. Implantable loop recorder (ILR) is a relatively recent investigational tool in undiagnosed syncope that permits prolonged monitoring without external electrodes. It is ideally suited to patients with infrequent recurrent syncope thought to be due to an arrhythmic cause. The newly available REVEAL LINQTM is a miniature ILR device which could be literally injected under the skin without a surgical incision. The mean diagnostic yield of ILR reported in the literature is about 50–60%.
Introduction
Syncope is defined as a transient loss of consciousness due to global cerebral hypo perfusion and is characterized by rapid onset, short duration, and spontaneous complete recovery. It is a frequently encountered clinical conundrum with an estimated lifetime prevalence of up to 35% [1]. It accounts for up to 3% of emergency department consultations and 6% of hospital admissions [2, 3, 4].
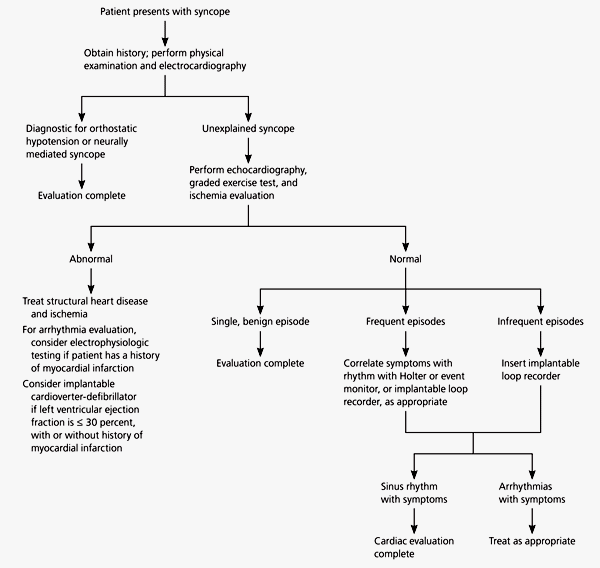
The causes of syncope could be broadly classified as those due to disorder of autonomic function, obstruction to blood flow or arrhythmia (Table1). Although clinical history and examination combined with laboratory testing are adequate in obtaining a diagnosis in many patients, there are nonetheless some who experience infrequent cardiac arrhythmias that are elusive in nature and difficult to detect. This is because correlation between syncopal events and any alteration of physiological signals (ECG, blood pressure) is the “gold standard” for
- the diagnostic work-up. In these individuals, prolonged ambulatory monitoring with implantable electrocardiographic recorders can be of great benefit.
- 1. Disorder of autonomic function
- Neurally-mediated syncope (vasovagal syncope, carotid sinus hypersensitivity, situational syncope)
- Chronic orthostatic intolerance (ie, postural orthostatic tachycardia syndrome [POTS])
- Orthostatic hypotension (secondary to volume depletion, systemic illness, use of a vasoactive drug or pure autonomic failure/multiple system atrophy)
- 2. Obstruction to blood flow (eg, aortic stenosis, aortic dissection, pulmonary embolism, pericardial tamponade, pulmonary hypertension, etc)
- 3. Arrhythmia (bradyarrhythmia or tachyarrhythmia)
Table 1: Causes of syncope.
Recurrent syncope thought to be due to an arrhythmic cause. Similar to the external loop recorder, it is designed to correlate physiology with recorded cardiac rhythms, but implanted and therefore devoid of surface electrodes and accompanying compliance issues. The ILR also monitors much longer time periods than an external loop recorder and current devices have an estimated battery life of about 36 months. These devices have a solid-state loop memory that stores retrospective ECG recordings, when activated either by the patient or a bystander, usually after a syncopal episode, or automatically activated in the case of occurrence of predefined arrhythmias [6]. A pair of built-in sensing leads located on the shell of the device allows for recording of a single lead bipolar electrocardiogram, which can be downloaded via radiofrequency with a special programmer. The device is usually implanted into the subcutaneous in the left pectoral area under local anesthesia. Advantages of ILRs include continuous loop high-fidelity ECG recording. Disadvantages include the need for a minor surgical procedure, the fact that sometimes it can be difficult to differentiate between supraventricular or ventricular arrhythmias, the presence of under- or over-sensing that may fill the memory, and the cost of the implantable device. The newly available REVEAL LINQTM is a miniature ILR device which could be literally injected under the skin without a surgical incision (Figures 2 & 3). The mean diagnostic yield of ILR reported in the literature is about 50–60% [7] and depends on the duration of monitoring.


Indication of ILR in Syncope Evaluation
Class I. ILR is indicated:
- In an early phase of evaluation of patients with recurrent syncope of uncertain origin who have: –absence of high-risk criteria that require immediate hospitalization or intensive evaluation [Table 2], and –a likely recurrence within battery longevity of the device (Level of evidence A)
- In high-risk patients in whom a comprehensive evaluation did not demonstrate a cause of syncope or lead to specific treatment (Level of evidence B). Class II A. ILR may be indicated: To assess the contribution of bradycardia before embarking on cardiac pacing in patients with suspected or certain neurally mediated syncope presenting with frequent or traumatic syncopal episodes (Level of evidence B) [8].
Class II B. ILR May Be Indicated
In patients with T-LOC of uncertain syncopal origin in order to definitely exclude an arrhythmic mechanism (Level of evidence C). Patients with high-risk criteria who are at high risk of sudden cardiac arrest and require prompt hospitalization or intensive evaluation are given in (Table 2).
If such high-risk criteria are present, ILR implantation should be postponed until a comprehensive evaluation has failed to find the cause of syncope [9].
High risk criteria which require intensive evaluation or prompt hospitalisation:
Severe structural or coronary artery disease (Previous MI , recent acute coronary syndrome, low ejection fraction) Clinical or ECG features suggesting syncope due to arrhythmia:
1. Syncope in supine position or during exertion
2. Palpitation at the time of syncope 3. Family history of sudden cardiac arrest
4. Non-sustained ventricular tachycardia 5. Bifascicular block or other conduction abnormalities with QRS duration ≥ 120 ms 6. Severe sinus bradycardia (<50 / min) or sinoatrial block in absence of physical training or negatively chronotropic medications 7. Pre-exited QRS complex 8. Prolonged or short QT interval 9. RBBB with ST elevation in leads V1-V3 (Brugada pattern) 10. Negative T waves in right precordial leads, epsilon waves, ventricular late potentials suggestive of arryhthmogenic
- right ventricular dysplasia
- Co-morbidities:
- 1. Severe anaemia
- 2. Dyselectrolytemia
Table 2: High risk criteria for patients with history of syncope.
into homogeneous patterns in order to define an acceptable standard, useful for future studies and clinical practice (Figure 4).
Type 1, Asystole. RR pause ≥ 3 s (a) Type 1A, Sinus arrest:
–Progressive sinus bradycardia or initial sinus tachycardia followed by progressive sinus bradycardia until sinus arrest (b) Type 1B, Sinus bradycardia plus AV block: –Progressive sinus bradycardia followed by AV block (and ventricular pause/s) with concomitant decrease in sinus rate –Sudden onset AV block (and ventricular pause/s) with concomitant decrease in sinus rate (c) Type 1C, AV block: –Sudden onset AV block (and ventricular pause/s) with concomitant increase in sinus rate Type 2, Bradycardia. Decrease of heart rate >30% or <40 bpm for >10 s (a) Type 2A. Decrease of heart rate >30% (b) Type 2B. Heart rate <40 bpm for >10 s Type 3, No or slight rhythm variations. Variations of heart rate <30% and heart rate >40 bpm (a) Type 3A. No variation or >10% variation in heart rate (b) Type 3B. Increase in heart rate >10% but <30% and <120 bpm; or, decrease >10% but <30% and >40 bpm Type 4, Tachycardia. Increase of heart rate >30% and heart rate >120 bpm.
(a) Type 4 A. Progressive sinus tachycardia (b) Type 4 B. Atrial fibrillation (c) Type 4 C. Supraventricular tachycardia (except sinus) (d) Type 4 D. Ventricular tachycardia Figure 4: The ISSUE classification of ECG-documented spontaneous syncope.
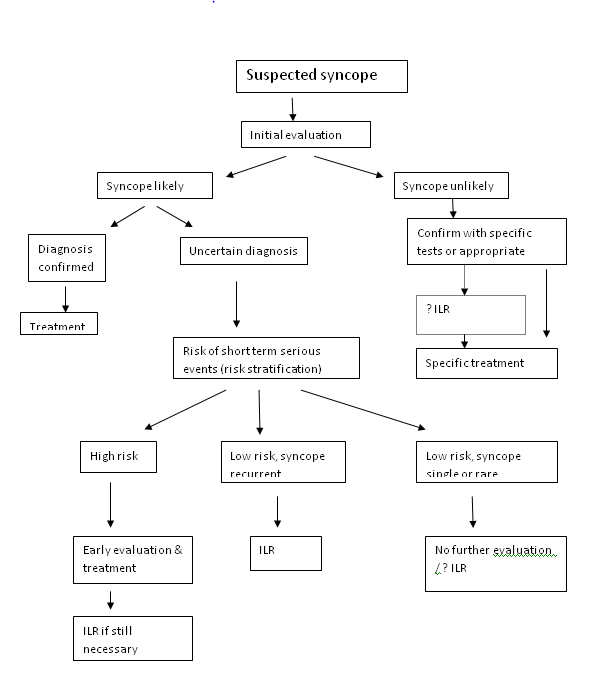
Type 1 (asystole) was the most frequent finding that was observed in 63% of patients; type 2 (bradycardia) was observed in 5% of patients; type 3 (no or slight rhythm variations was observed in 18% of patients); and type 4 (tachycardia) was observed in 14% of patients. In types 1A, 1B, and 2, the findings of progressive sinus bradycardia, most often followed by ventricular asystole due to sinus arrest, or progressive tachycardia followed by progressive bradycardia and, eventually, ventricular asystole due to sinus arrest, suggest that the syncope is probably neutrally mediated. In type 1C, the finding of prolonged asystolic pauses due to sudden-onset paroxysmal AV block with concomitant increase in sinus rate suggests another mechanism, namely intrinsic disease of the His –Purkinje system as observed in Stokes –Adam attacks. In types 4B, 4C, and 4D, a primary cardiac arrhythmia is typically responsible for syncope. In the other types, in which no arrhythmia is detected, the exact nature of syncope remains uncertain because of the lack of contemporary recording of blood pressure; however, the finding of progressive heart rate increase and/or decrease at the time of syncope suggests a (primary or secondary) activation of the cardiovascular system and a possible hypertensive mechanism [10]. The ISSUE investigators (International Study on Syncope of Unknown Etiology) have landmark trials on the utility of the ILR in syncope. The first trial examined the use of ILR in three different groups of patients suffering from syncope who had undergone conventional testing. In the first trial, 111 patients with unexplained syncope underwent HUTT followed by ILR implantation (regardless of the HUTT results) [11]. Syncope recurred in 34% of patients in both HUTT-positive and HUTT- negative patients, with marked bradycardia and asystole being the most common recorded arrhythmia (46% of the HUTT positive and 62% of the HUTT-negative patients). The heart rate responses seen during HUTT did not seem to predict the ILR recorded responses, with a much higher rate of asystole than was noted during HUTT. In the second ISSUE study, ILRs were placed in 52 patients with syncope and bundle branch block who had unremarkable electrophysiological studies [12]. Syncope recurred in 22 of the 52 patients, with 17 patients exhibiting bradycardia due to complete heart block. The third part of the ISSUE study looked at 35 patients with syncope and structural heart disease who had negative electrophysiological testing [13]. The underlying heart disease was principally ischemic heart disease or hypertrophic cardiomyopathy with only moderate left ventricular dysfunction. Syncope recurred in 19 of the 35 patients (54%), with bradycardia observed in four, supraventricular tachycardia in five, and ventricular tachycardia in only 1 patient. There were no cases of sudden cardiac death that occurred during the 16±11 months of follow-up. The results of the study supported the use of ILR monitoring in syncope patients with moderate left ventricular dysfunction secondary to heart disease when electrophysiological testing is negative. The ISSUE-2 trial, 21 a prospective, multicentre, observational study that aimed to assess the efficacy of specific therapies based on ILR results in patients with suspected recurrent neutrally mediated syncope [14]. Patients were enrolled if they had experienced more than three clinically severe syncopal episodes in the previous 2 years (in the absence of significant electrocardiographic or cardiac abnormalities). Patients suffering from orthostatic hypotension and carotid sinus hypersensitivity were excluded. Following ILR implantation, patients were followed until the first documented syncopal event (phase 1). Then characteristics of the ILR recording of this episode determined the subsequent therapy that was pursued during phase 2 of the study. Out of 392 patients, the recurring rate in the first year of the phase 1 study was 33%. One hundred 5three patients had an ILR- documented syncopal event and were entered into phase 2 of the trial. Of these, 53 patients received specific therapy: 46 received permanent pacemakers because of documented asystole (median duration 11.5 s), 6 underwent therapy for tachyarrhythmias (catheter ablation in 4 patients, implantable cardioverter- defibrillator placement in 1, and antiarrhythmic drug therapy in another). The remaining 50 patients did not receive any specific therapy. The recurrence rate after 1 year in the ILR guided therapy group was 10% (a syncope burden of 0.7±0.2 episodes per patient per year) compared with 41% (burden 0.8±1.57 episodes per patient per year) patients who did not receive specific therapy. This represents an 80% relative risk reduction (p50.002) as well as a 92% reduction in syncope burden (p=0.002) in the guided therapy group. The recurrence rate in the patients who received a pacemaker was 5% (burden 0.05±0.15 episodes per patient year. Severe trauma secondary to the syncopal events was received in 2% of patients and mild traumas in 4% of patients. Thus, the study demonstrated that early use of an ILR in the evaluation of recurrent unexplained syncope, with application of therapy based on ILR results, allowed for a safe and effective means of diagnosis and management The current status of ILR in evaluation of syncope is given in (Figure 5).
References
-
Ganzeboom KS, Mairuhu G, Reitsma JB, Linzer M, Wieling W, et al. (2006) Lifetime cumulative incidence of syncope in the general population: a study of 549 Dutch subjects aged 35-60 years. J Cardiovasc Electrophysiol 17(11): 1172-1176.
-
Brignole M, Menozzi C, Moya A, Garcia-Civera R, Mont L, et al. (2001) Mechanism of syncope in patients with bundle branch block and negative electrophysiological test. Circulation 104(17): 2045- 2050.
-
Farwell D, Sulke N (2002) How do we diagnose syncope? J Cardiovasc Electrophysiol 13(1): S9-13.
-
Soteriades ES, Evans JC, Larson MG, Chen MH, Chen L, et al. (2002) Incidence and prognosis of syncope. N Engl J Med 347(12): 878-885.
-
Strickberger SA, Benson DW, Biaggioni I, Callans DJ, Cohen MI, et al. (2006) AHA/ACCF scientific statement on the evaluation of syncope: from the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; and the American College of Cardiology Foundation In Collaboration With the Heart Rhythm Society. Circulation 113(2): 316-327.
-
Krahn AD, Klein GJ, Yee R, Norris C (1997) Maturation of the sensed electrogram amplitude over time in a new subcutaneous implantable loop recorder. Pacing Clin Electrophysiol 20(6): 1686-1690.
-
Iglesias JF, Graf D, Pascale P, Pruvot E (2009) The implantable loop recorder: a critical review. Kardiovaskuläre Medizin 12(3): 85-93.
-
Brignole M, Vardas P, Hoffman E, Huikuri H, Moya A, et al. (2009) Indications for the use of diagnostic implantable and external ECG loop recorders. Europace 11(5): 671-687.
-
Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, et al. (2009) Guidelines for the diagnosis and management of syncope. Eur Heart J 30(21): 2631- 2671.
-
Brignole M, Moya A, Menozzi C, Garcia-Civera R, Sutton R (2005) Proposed electrocardiographic classification of spontaneous syncope documented by an Implantable Loop Recorder. Europace 7(1): 14-18.
-
Moya A, Brignole M, Menozzi C, Garcia-Civera R, Tognarini S, et al. (2001) Mechanism of syncope in patients with isolated syncope and in patients with tilt-positive syncope. Circulation 104(11): 1261-1267.
-
Brignole M, Menozzi C, Moya A, Garcia-Civera R, Mont L, et al. (2001) Mechanism of syncope in patients with bundle branch block and negative electrophysiological test. Circulation 104(17): 2045- 2050.
-
Menozzi C, Brignole M, Garcia-Civera R, Moya A, Botto G, et al. (2002) Mechanism of syncope in patients with heart disease and negative electrophysiological test. Circulation 105(23): 2741-2745.
-
Brignole M, Sutton R, Menozzi C, Garcia-Civera R, Moya A, et al. (2006) Early application of an implantable loop recorder allows effective specific therapy in patients with recurrent suspected neutrally mediated syncope. Eur Heart J 27(9): 1085- 1092.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study