Simultaneous Progression and Regression of Coronary Artery Disease in a Patient from North India
Background: Lipids have a central role in the pathogenesis of atheroma formation. Statins are known to favorably alter the morphology of plaque and decrease the atheroma volume. Case: We present a case of 45 year old male who had spontaneous regression of coronary artery disease in Left anterior descending (LAD) with progression of coronary artery disease in left circumflex (LCX) and right coronary artery (RCA) over a period of 7 years. Conclusion: Disease regression could be attributable to statins while mechanism for simultaneous progression in other two vessels is still unclear.
Case Presentation
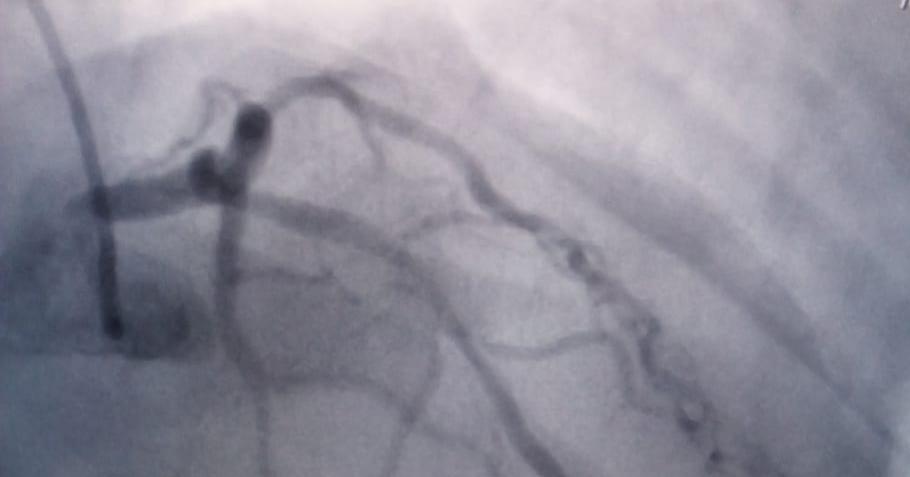
Patient continued the treatment with good compliance and was on regular follow up in outpatient department. However he was admitted again as a case of Acute Coronary Syndrome in 2016. His Echo showed regional wall motion abnormality, mild MR, trace pericardial effusion and ejection fraction of 40%. He underwent coronary angiography which revealed left main normal, LAD 20% residual stenosis (Figure 2), LCX proximal & mid 90% tandem lesions, RCA proximal plaquing followed by mid to distal diffuse 95% lesion with thrombus & spontaneous spiral dissection (Figure 3), Ramus ostial plaquing.
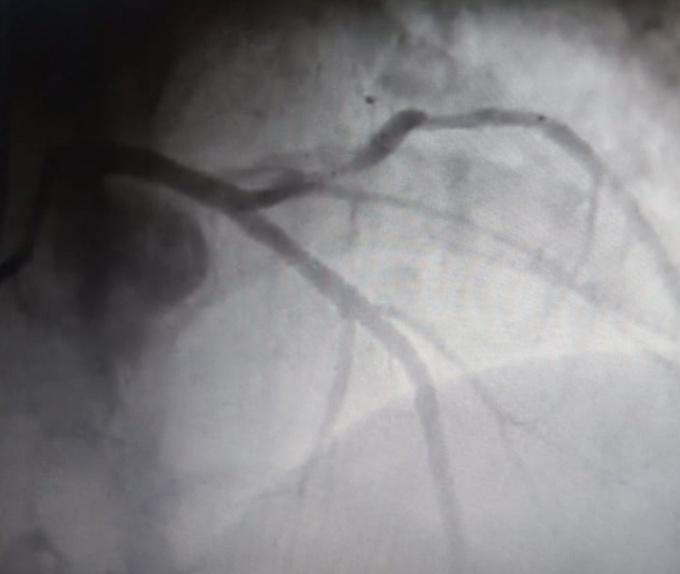
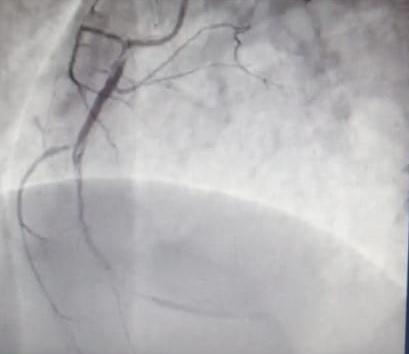
CAG was consistent with regression of CAD in LAD & progression of CAD in RCA & LCx. Subsequently he underwent PCI and stenting to RCA (3 stents) and LCx (1 stent) using everolimus eluting stents with good end results.
Discussion
Plaque reversal occurs by removal of lipids and necrotic material, endothelial repair, or halt of vascular smooth muscle cell proliferation. Serial CTA evaluation of coronary plaques allows for the assessment of interval change in the plaque morphology. Statin treatment results in decrease in the plaque and necrotic core volume [1]. Statin treatment induces favorable plaque morphologic changes with an increase in fibrous cap thickness, and decreases in both percentage plaque and lipid volume indexes [2]. In a meta-analysis of eight trials, 919 patients (461 patients in the statin group and 458 in the placebo group) were studied with intravascular ultrasound (IVUS). There was no significant difference between the two groups in terms of their plaque characteristics at baseline. However, there was a statistically significant mean difference in coronary atheroma volume between the statin therapy and the placebo arms, which was −3.573 (P < 0.01). This suggests that statins have the potential to induce plaque reversal [3]. One small study analyzed the effects of rosuvastatin combined with ramipril on atheroma volume and its mechanism in patients with intermediate CAD. In this study, 21 patients received rosuvastatin (20mg daily) and 19 patients received rosuvastatin along with ramipril (20mg and 10mg, respectively) for 9 to 12 months. There was decrease in the TAV in both groups, with reduction in the CRP levels in the combination treatment group [4]. Hibi, et al. studied effects of statin treatment on plaque regression in patients with polyvascular disease versus those with CAD alone. They studied 252 patients (at 33 centers) with a history of an ACS, who underwent percutaneous intervention to localize the lesion followed by treatment with atorvastatin (20mg per day) or pitavastatin (4mg per day). Both groups showed regression of plaques, as assessed by IVUS at baseline and at 8–12 months follow-up [5]. In a prospective randomized comparative study using rosuvastatin 20 mg (n = 65) and atorvastatin 40mg (n =
63), IVUS was used at baseline and at 11-month follow- up, to show effective plaque regression. TAV and percent atheroma volume (PAV) was measured. Plaque was decreased in 99 of 128 patients (77%); (85% in the rosuvastatin group vs 70% in the atorvastatin group). Both groups showed change in TAV: −4.4 ± 7.3 mm3 for the rosuvastatin group and –3.68 ± 6.8 mm3 for the atorvastatin group (P = 0.5). The difference in PAV between the two groups was not statistically significant (P = 0.14). These results demonstrate that both statins are effective in reducing plaque burden [6]. Kovarnik, et al. randomized 89 patients to receive either atorvastatin 80mg plus ezetimibe 10mg or standard treatment per the patients’ general practitioner for 12 months. The authors found a decrease in the coronary artery PAV (−0.4%) in the group on combination treatment versus an increase (+1.4%) in the other group (P = 0.014), as measured by IVUS. There was also an increased frequency of combined atherosclerosis regression (increased lumen volume plus decreased PAV) in patients taking both medications (40.5%) compared with the group on monotherapy (14.9%) (P = 0.007) [7]. The literature available suggests that statins play an important role in plaque regression .However in our case it was surprising to have disease regressed in one vessel while it progressed in the other two vessels. The exact mechanism is still debatable.
Conclusion
Major reductions in coronary events are associated with aggressive medical therapy. Statin therapy is associated with beneficial histological changes in plaque morphology as demonstrated by IVUS. The cellular and molecular mechanisms responsible for plaque regression in humans are less understood. Our case represents a unique combination of simultaneous regression of disease in LAD with progression in LCX and RCA, despite giving statin therapy. More studies are needed to clearly elucidate this issue.
References
-
Inoue K, Motoyama S, Sarai M, Sato T, Harigaya H, et al. (2010) Serial coronary CT angiography-verified changes in plaque characteristics as an end point. JACC Cardiovasc Imaging 3(7): 691-698.
-
Hattori K, Ozaki Y, Ismail TF, Okumura M, Naruse H, et al. (2012) Impact of statin therapy on plaque characteristics as assessed by serial OCT, grayscale and integrated backscatter-IVUS. JACC Cardiovasc Imaging 5(2): 169-177.
-
Bedi U, Singh M, Singh P, Molnar J, Khosla S, et al. (2011) Effects of statins on progression of coronary artery disease as measured by intravascular ultrasound. J Clin Hypertens (Greenwich) 13(7): 492- 496.
-
Han SH, Chung WJ, Kang WC, Lee K, Park YM, et al. (2012) Rosuvastatin combined with ramipril significantly reduced atheroma volume by anti- inflammatory mechanism: Comparative analysis with rosuvastatin alone by intravascular ultrasound. Int J Cardiol 158(2): 217-224.
-
Hibi K, Kimura T, Kimura K, Morimoto T, Hiro T, et al. (2011) Clinically evident polyvascular disease and regression of coronary atherosclerosis after intensive statin therapy in patients with acute coronary syndrome: serial intravascular ultrasound from the Japanese assessment of pitavastatin and atorvastatin in acute coronary syndrome (JAPAN-ACS) trial. Atherosclerosis 219(2): 743-749.
-
Hong YJ, Jeong MH, Hachinohe D, Ahmed K, Choi YH, et al. (2011) Comparison of Effects of rosuvastatin and atorvastatin on plaque regression in Korean patients with untreated intermediate coronary stenosis. Circ J 75(2): 398-406.
-
Kovarnik T, Mintz GS, Skalicka H, Kral A, Horak J, et al. (2012) Virtual histology evaluation of atherosclerosis regression during atorvastatin and ezetimibe administration: HEAVEN study. Circ J 76(1): 176-183.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study