The Added Value of 3D Transesophageal Chocardiography over 2D Transesophageal Echocardiography in the Assessment of Infective Endocarditis
Infective endocarditis is a peculiar disease that still carries a poor prognosis and high mortality despite major advances in both diagnostic and therapeutic procedures. It is not a uniform disease, but presents in a variety of different forms, varying according to the initial clinical manifestations, the underlying cardiac disease (if any), the microorganism involved, the presence or absence of complications, and underlying patient characteristics. The incidence of infective endocarditis ranges from one country to another within 3–10 episodes/100 000 person-years. Three-dimensional (3D) echocardiography has been conceived as one of the most promising methods for the diagnosis of infective endocarditis, and recently has become an integral clinical tool. The aim of this study was to evaluate the added value of 3D transesophageal echocardiography over 2D transesophageal echocardiography in the diagnosis of infective endocarditis.
Introduction
Patients and methods
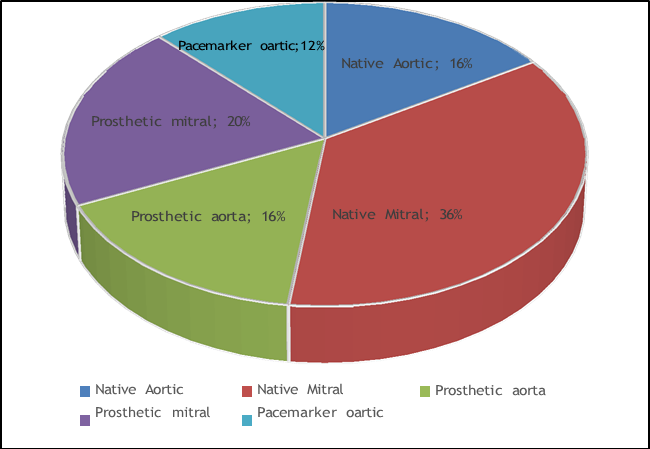
All patients were diagnosed to suffer from definite infective endocarditits based on modified Duke criteria, there were 19 males (76%) and 6 females (24%), while the age of the studied patients ranged from 20-66 with a mean age of 43.12±13.7 years.
The left sided of the heart alone was involved in 23 patients (92%).
15 Patients (60%) had the disease on the left sided native valves, 8 patients (32%) had the disease on the left sided prosthesis. The mitral valve was affected in
16patients (64%), 11 patients (44%) on top of native mitral valves and 5 patients (20%) on top of mitral prosthesis. The aortic valve was involved 7 patients (28%), 4 patients (16%) on top of native aortic valve and 3 patients (12%) on top of aortic prosthesis.
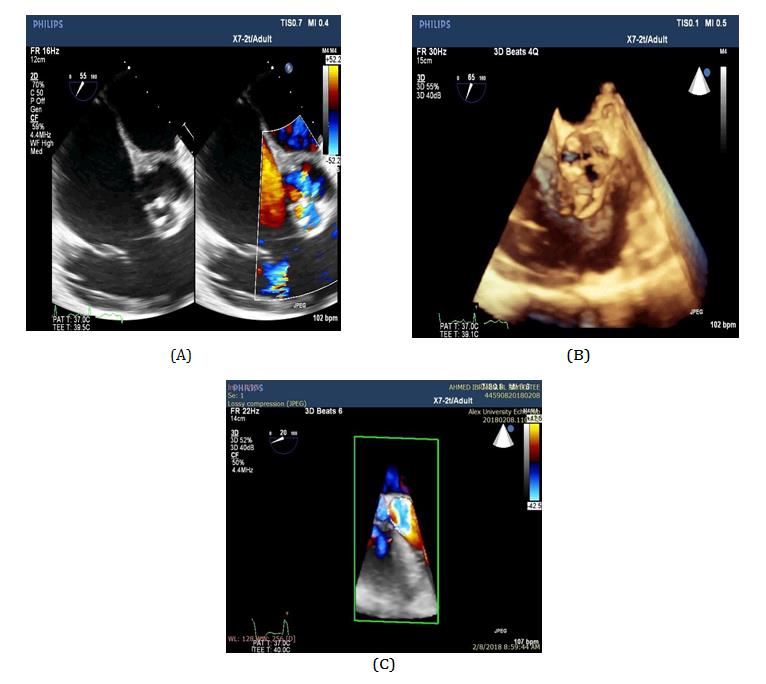
The right side of the heart alone was involved in 2 patients (8%) with intracardiac device related infective endocarditis (Figure 1).
Methods
The modified Dukes diagnostic criteria was used to make the diagnosis of infective endocarditis. These combine the clinical, pathologic, microbiologic and echocardiographic aspects. Complete 2D TEE study was performed for all subjects according to the standard protocol [1] followed by 3D TEE using a matrix probe (X7-2) connected to iE33 system (Philips Medical Systems, Andover, MA, USA). The study was approved by the hospital ethical committee. Using Simultaneous Multiplane Mode, ZOOM” mood and Full Volume—Gated Acquisition mood. Then using a crop box, the 3D data set was then dissected in multiple plane angulations to obtain views from any desired direction. In particular, en face views of the valves were obtained to facilitate the visualization of leaflet perforations and abscess formation. The mitral valve (for example :): was divided into three segments of the anterior mitral leaflet (designated A1, A2, and A3) and three scallops of the posterior mitral leaflet (P1, P2, and P3). A1 and P1, A2 and P2, and A3 and P3 were assigned to the anterolateral, middle, and posteromedial sections of the mitral valve [2, 3], the vegetation area was calculated and specific areas of the valve involved with the vegetative process and noted whether there were any complications of infective endocarditis.
Results
Echocardiogrphic analysis of the native valves pathology
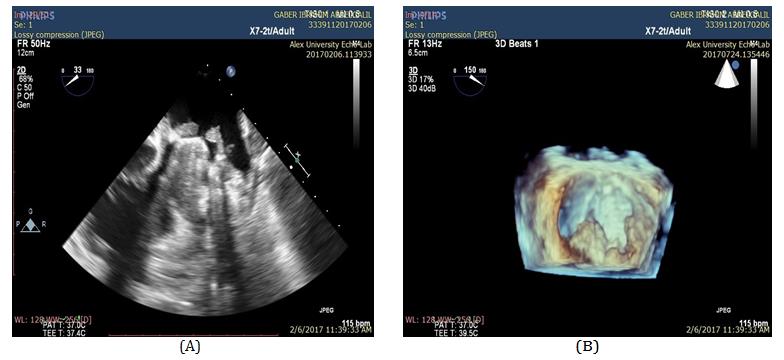
By 2D TEE vegetations of variable sizes were seen attached to 10 mitral valves and 1 aortic valves. 3D TEE confirm the diagnosis of vegetations in the same patients, the 3D en face view using zoom mode helped in delineation of the size, site and number of vegetations. The vegetations size were mildly larger by 3D TEE than 2D TEE, the number of vegetations was similar in both technique but the shape was different (Figure 2).
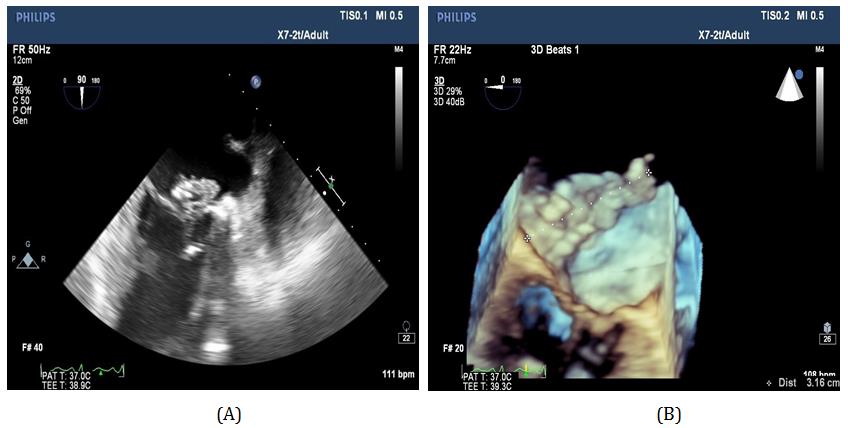
B) 3D TEE of the mitral valve from the left atrial surface showing large vegetation at p1 scallop.
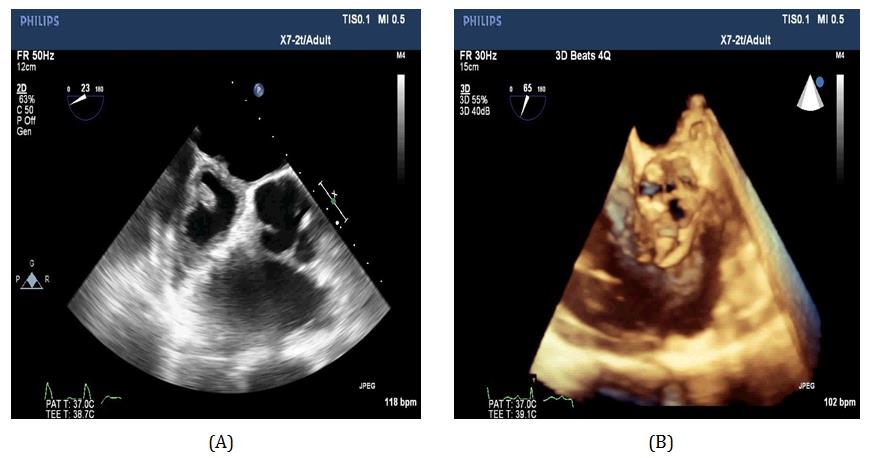
Annular abscesess were detected in 4 patients, 3 patents in the aortic position and one patient in the mitral position, The abscesses were associated with vegetation in one aortic annular abscess and the mitral annular abscess.
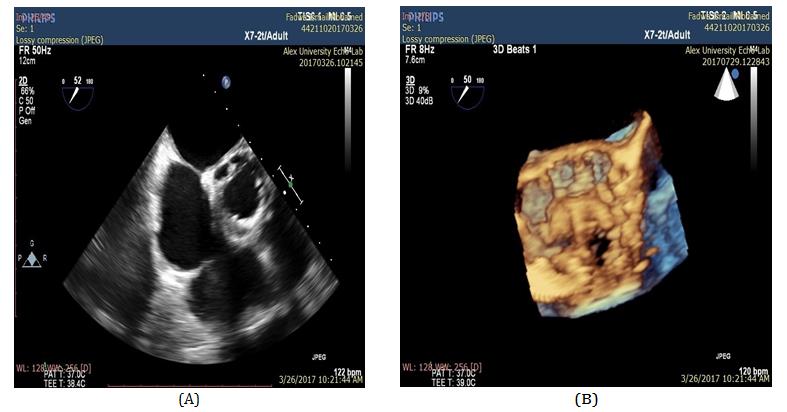
3D TEE confirmed the presence of the abscesses in addition to the assessment of the size, site, extension and wall thickness of the abscess. Through cropping of the full volume 3D images with and without color Doppler the communication orifice of the abscess cavity was well visualized in the en face view (Figure 3).
Valve perforations were present in 8 mitral valves and 3 aortic valves.
3D TEE confirm the presence of perforations with accurate localization of the site of perforations in terms of scallops and cusps affected (Figure 3).
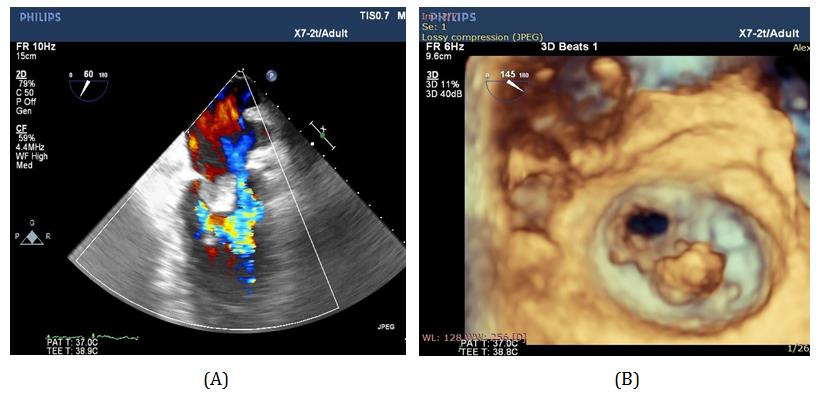
other patient 3D TEE confirmed the prescience of fistula between the aorta -right atrium and aorta –right ventricle that was suspicious by 2D TEE (Figures 4 & 5).
Echocardiographic analysis of the prosthetic valve pathology (Table 1).
| 2D TEE | 3D TEE | 3D TEE value | ||||||
|---|---|---|---|---|---|---|---|---|
| Vegetation : | Confirm the 2D TEE diagnosis in both mitral and aortic position. Complete and adequate analysis of the vegetation number, size, location and attachment. | |||||||
| Identification | ++ | ++ | ||||||
| Number | + | ++ | ||||||
| Size | + | ++ | ||||||
| Location | + | ++ | ||||||
| Attachment | + | ++ | ||||||
| Abscess: | Confirmed the 2D TEE in all cases. Better estimation of the abscess size, site, extension and communication points. Comprehensive description of the abscess wall and cavity by multiple slicing at different levels | |||||||
| Identification | ++ | ++ | ||||||
| Size | ± | ++ | ||||||
| Site | + | ++ | ||||||
| Extension | + | ++ | ||||||
| Communication | ± | ++ | ||||||
| Regurgitation: | ||||||||
| Transvalvular | ++ | ++ | Clear differentiation of transvalvular and paravalvular regurgitation in all cases with more understand of the mechanism of regurgitation. | |||||
| Paravalvular | + | ++ | ||||||
| Mechanism | + | ++ | ||||||
| Severity | + | + | ||||||
| Jet direction | + | + | ||||||
| Perforation: | ||||||||
| Identification | + | ++ | Confirm the presences of perforation with accurate assessment of the perforation site and size. | |||||
| Site | + | ++ | ||||||
| Size | - | ++ | ||||||
| PV Dehiscence: | ||||||||
| Identification | + | ++ | Superior description of the dehisced segment (site ,size ,shape and area of the dehisced segment) as well as their relationship to the paravalvular regurgitation. | |||||
| Site | ± | ++ | ||||||
| Size | - | ++ | ||||||
| Shape | - | ++ | ||||||
| Area | - | ++ |
Table 1: Summarized additional value of 3D TEE in infective endocarditis. - = Not Possible; ± = Can be obtained; + = Suboptimal;
Absent 7 28 7 28
standard 2D TTE 3D TEE Percent of Additional value of 3DTT No. % No. % No. % Vegetation
12 66.6 Correct 6 24 18 72 Incomplete correct 12 48 0 0
| Abscess | ||||||
|---|---|---|---|---|---|---|
| Absent | 17 | 68 | 17 | 68 | 4 | 50 |
| Correct | 4 | 16 | 8 | 32 | ||
| Incomplete correct | 4 | 16 | 0 | 0 | ||
| Fistula | ||||||
| Absent | 22 | 88 | 21 | 84 | 3 | 75 |
| Correct | 1 | 4 | 4 | 16 | ||
| Incomplete correct | 2 | 8 | 0 | 0 | ||
| Perforation | ||||||
| Absent | 14 | 56 | 14 | 56 | 10 | 90 |
| Correct | 1 | 4 | 11 | 44 | ||
| Incomplete correct | 10 | 40 | 0 | 0 | ||
| Dehiscence of prostheic valve | ||||||
| Absent | 4 | 50 | 4 | 50 | 4 | 100 |
| Correct | 0 | 0 | 4 | 50 | ||
| Incomplete correct | 4 | 50 | 0 | 0 |
Table 2: Echocardiography results in relation to 2D TEE and 3D TEE. Correct = Correct Diagnosis with complete data information; I
In 2 patients the vegetations appeared as multiple vegetations by 2D TEE while by 3D TEE it appeared as a single large mass (Figure 6).
3D TEE confirmed the presence of the abscesses in addition to the assessment of the size, site extension and wall thickness of the abscess.
Through cropping of the full volume 3D images using color Doppler revealed the communication orifices of the abscess cavities (Figure 7).
3D TEE was able to assess the severity and direction of paravalvular leakage in all patients. It also differentiated between transvalvular and paravalvular regurgitation. Using zoom mode, the extent of paravalvular regurgitation was identified in all prosthetic valves in enface view.
Compared to 2D TEE, 3D TEE showed details of all of the dehisced segments site, size, shape, and area of dehisced segment (Figure 8).
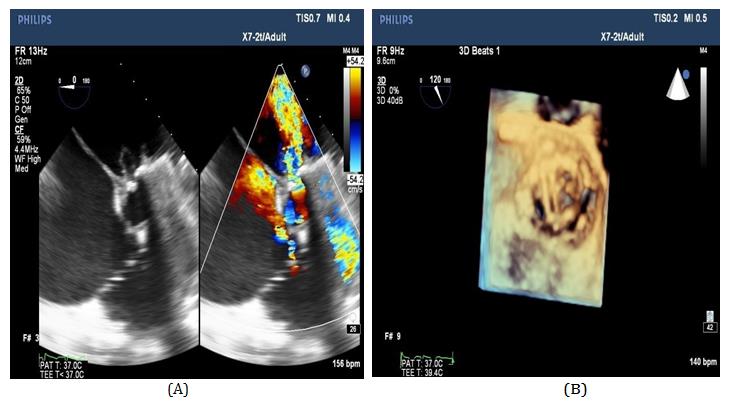
of such fistulae in the two patients with accurate localization of their extension (Figure 9).
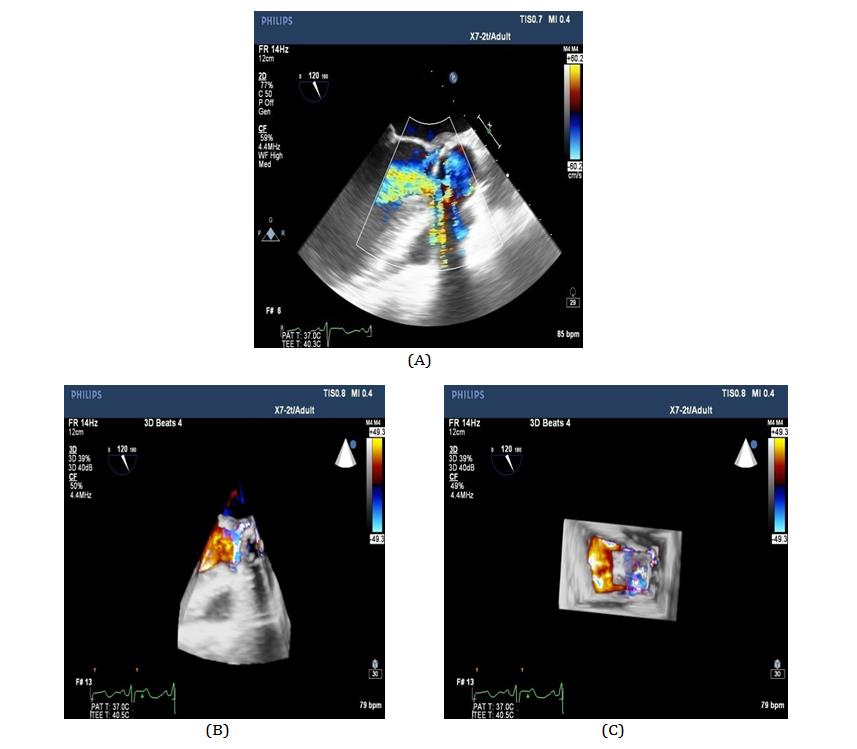
B & C) 3D color full volume demonstrate the fistula between the aorta and left atrium.
Discussion
In this study, we showed the incremental benefit of 3D TEE on top of 2D TEE for the evaluation of valvular vegetations. In this study, we showed that 3D TEE is able to identify and localize vegetations better than 2D TEE.
In our study views obtained by 2D TEE were limited by the anatomic restriction of the imaging probe inside the esophagus. On the contrary, using cropping planes, images could be obtained from any direction using 3D TEE. In addition to facilitating our localization of vegetations, 3D TEE allowed us to visualize the leaflets en face, therefore, greatly enhancing our ability to detect and measure leaflet perforations and allowing us to measure the area of the valve leaflet that was involved in the infective process and the area that was free from destruction.
It was almost impossible to image the entirety of complicated mobile vegetation with 2D echocardiography. In contrast, 3D echocardiography, facilitated visualization of the full extension and motion of the complicated vegetation in one view from any desired angle. As a result, the maximum size of the vegetation was underestimated by 2D TEE as compared to 3D TEE.
Annular abscesses size, site, extension, wall thickness of the abscess could be identified by RT3D TEE. Through cropping of the full-volume 3D images, the orifice of communication of the abscess cavity could be visualized well in en face view.
3D TEE confirm the presence of perforations with accurate localization of the site of perforations in terms of scallops and cusps affected.
3D TEE showed details of all of the dehisced segments of the prosthetic valves, site, size, shape, and area of dehisced segment.
The ability to visualize the valve in its anatomic and realistic perspectives allowed us to perceive the vegetative process as a continuum from vegetation to abscess formation and valve destruction. Another advantage in the use of 3D TEE was its ability to measure the area of vegetations, which was not possible when imaging in 2D.
Since the size of vegetations has been shown in previous studies to be a strong prognostic indicator in patients with infective endocarditis, a more robust and accurate assessment of size using 3D TEE might provide incremental prognostic data to that available from 2D imaging [3].
et al. (2003) Usefulness of transesophageal three‐dimensional echocardiography in the identification of individual segment/scallop prolapse of the mitral valve. Echocardiography 20(2): 203-209.
In the 25 patients who were studied, 3D TEE provided superior images of both the presence and the site of valvular vegetations as compared to2D TEE, and delivered additional information with respect to the area of vegetations, extent of involvement with the infective process, and complications of infective endocarditis that were useful to the cardiac surgeons.
Conclusion
This study provides evidence of the incremental value of 3D transesopageal echocardiography over 2D transesophageal echocardiography in the assessment of infective endocarditis with clear and realistic images resemble true pathology, and the assessment of extent of the involvement of the infective process and complications of infective endocarditis that are useful for cardiac surgeons.
References
-
Hahn RT, Abraham T, Adams MS, Bruce CJ, Glas KE, et al. (2013) Guidelines for Performing a Comprehensive Transesophageal Echocardiographic Examination: Recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr 26(9): 921-364.
-
Manda J, Kesanolla SK, Hsuing MC, Nanda NC, Abo- Salem E, et al. (2008) Comparison of real time two‐ dimensional with live/real time three‐dimensional transesophageal echocardiography in the evaluation of mitral valve prolapse and chordae rupture. Echocardiography 25(10): 1131-1137.
-
Ahmed S, Nanda NC, Miller AP, Nekkanti R, Yousif AM,
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study