Surgery for Primary Cardiac Tumors in Mexican Children: Preliminary report
Background: Primary cardiac tumors are a rare disease with an incidence in childhood of 0.27%. 90% of these tumors are benign but by their location and size can be malignant because of the clinical behavior. The most common types are rhabdomyoma, fibroma and myxoma. The Clinical symptoms consist of arrhythmias, heart murmur, and heart failure. Curative treatment is surgical resection. Our main goal is to describe the clinical results in Mexican pediatric patients in whom a primary cardiac tumor was removed. Highlighting the importance of the initial clinical assessment, As well the usefulness of echocardiography in the morphologic diagnosis of primary cardiac tumors in pediatric patients. Material and methods: We included 11 patients with primary cardiac tumor, with indications for surgical treatment due to obstruction and arrhythmias. Results: We found 5 patients with rhabdomyoma, fibroma in 3 patients and 3 patients with myxoma as well. The mortality was 9 % (1 patient), and morbidity was found in 27% (3 patients) secondary to pneumonia. Conclusions: Early diagnosis of primary cardiac tumor allows us a curative surgical treatment of this pathology. The emphasis in the initial clinical assessment and the echocardiography performed by an expert cardiologist and echo cardiographer allow us an accurate cardio anatomic orientation and location of the tumor at the time of echocardiography. According the results presented in this study the frequency of occurrence of this disease is higher on Mexican children population than the reported in the literature and surgical resection have curative results in over 90% of cases.
Introduction
Primary heart tumors have an incidence in the general population ranging from 0.005 to 0.05%. In pediatric patients, the incidence is 0.27% [1, 2]. The most frequent tumor in childhood is rhabdomyomas (45%), followed by fibroids (25%). Its clinical presentation is variable, but in most cases is asymptomatic. In the neonate they may condition the appearance of arrhythmias or hydrops fetalis; in the group of infants they can present low cardiac output data or sudden death. In later stages the main clinical manifestations are arrhythmias and murmurs. 90% of primary cardiac tumors are benign in children. But according to its size, location and number can be of malignant clinical behavior by blockage of blood flow or causing lethal arrhythmias [3]. The most common types of primary heart tumors are rhabdomyoma, fibroma and myxoma.
Rhabdomyoma
It is the most common histologic form in fetal and pediatric stage. It was first described by Von Recklinghausen associated with neurofibromatosis. It is characterized for been circumscribed, lobular, whitish or greyish, usually multiple in up to 90% of cases and is usually found in the thickness of the heart muscle and can affect any point, prevailing in the ventricles and of them, the left ventricle [4]. Rhabdomyomas are associated with tuberous sclerosis by up to 81%. Lymburner found an incidence of 0.05% in 8,500 autopsies. In several series of autopsies, the reported incidence is from 0.027 to 0.08% in pediatric patients and the prevalence of 1: 10,000 [1].
Fibroma
The first heart fibroma was described in 1855, with the first successful resection in 1962, 90% of these tumors occur at school age in children under 12 years. The most common anatomical site is the free wall or septum from left ventricle, less frequently they arise from the right ventricle or atrium. Up to 10% of patients with cardiac fibroma die suddenly. Because these tumors do not show spontaneous regression and because after surgical resection usually have no recurrence, the treatment of choice is surgical and is considered curative [2, 3].
Myxoma
A benign tumor of primitive mesenchymal cells, which in 90% of cases are in the atria, 4 times more frequent on the left side and with predominance in the septum. They occupy 50% of benign cardiac tumors in adults [4, 5]. These are rare disorder but up to 7% of cases are familial. Clinically it manifests with dyspnea, palpitations, strokes, chest pain, syncope, fever and peripheral arterial embolism [6]. They are presented with pericardial effusion, heart failure, arrhythmias, peripheral embolization, syncope and cerebral embolism in 12% of cases [7].
It is associated with Carney complex including cardiac myxomas, endocrine disease and pigmented skin lesions [8, 9]. The election treatment is surgical resection, the recurrence is usually 1-3% and in patients with Carney complex is up to 25%. In general, for all heart tumors the diagnostic method of choice is Doppler echocardiography, in cases of difficult diagnosis and high clinical suspicion are useful Magnetic resonance imaging (MRI) and Angio Computed Tomography (CT) with three-dimensional (3D) reconstruction [10].
Primary cardiac tumors are a rare disease in all ages but even more in the pediatric age, the improving of non- invasive diagnostic tests has increased the possibilities of earlier diagnostic accuracy as well as a better and definitive opportunity of treatment in this group of age. At the HRAEB (Regional Hospital of High Specialty of Bajio, Leon city, Mexico), surgical resection of primary cardiac tumors in pediatric patients is 2.1% of all procedures performed over the last five years in the service of Pediatric Cardiovascular Surgery. In this article we present the results of resection of 3 different histological types of primary heart tumors in 11 pediatric patients.
Objective
Our main goal is to describe the results in Mexican pediatric patients to whom were removed a primary cardiac tumor in the Regional Hospital of High Specialty of the Bajio (HRAEB) Mexico. Highlighting the importance of the initial clinical assessment as well as the usefulness of echocardiography for the appropriate anatomical diagnosis of primary cardiac tumors in pediatric patients, without the availability of more diagnostics aids such as Angio CT or MRI.
Material and Methods
This is a descriptive, retrospective study with a series of cases of children with primary cardiac tumors diagnosed by initial clinical assessment and echocardiography. Measures of central tendency, such as average age, weight, intrahospital stay days and frequency measurements as morbidity and mortality were performed (Excel 2018). From a total of 528 heart surgeries in pediatric patients, carried out from June 2008 to December 2012, we found and reviewed the medical records of 11 children diagnosed with primary cardiac tumor, to who was performed surgical resection of the tumor as an initial option treatment. Clinical data, demographic and diagnostic studies values were evaluated as well.
Results
Demographic characteristics: The average age was 4.8 years (age from 3 weeks to 13 years), weight was 16.6 kg (2.8 to 35 kg), 6 of 11 patients (55%) were females and 5 (45%) men. Diagnosis of all patients was made by clinical assessment and bidimensional echocardiography. The average follow-up was 21 months; this was done in 100% of patients through outpatient, with sequential echocardiograms. Mortality was 9% (1 patient) in the immediate postoperative, secondary to acute pulmonary edema due to left ventricular dysfunction (interventricular septum tumor and free wall of the left ventricle). All patients entered the operating room with a preoperative diagnosis of tumor type, location and size. Histopathologic corroboration of all surgical specimens was obtained. In all patients (100%) the tumor was completely removed.
Tumor Types were
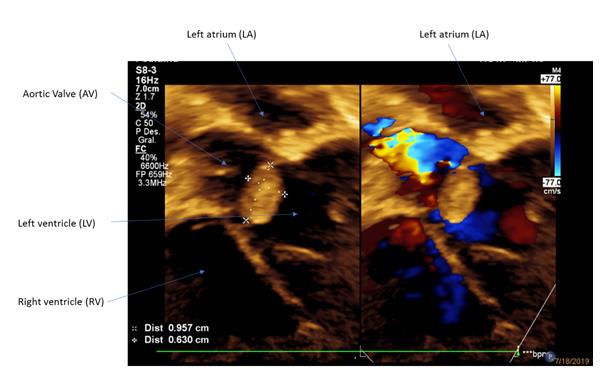
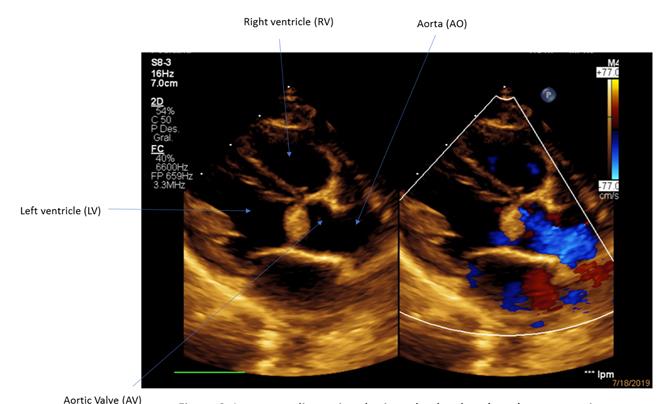
Rhabdomyoma: It was detected in 5 patients; in prenatal period 2 patients and in the neonatal period in 3, all of them with obstruction of the left ventricular outflow, intermittent presentation of ventricular tachycardia and evidence of congestive heart failure. The 5 patients were auscultated with ejection murmur in mesocardium at the precordial area. All of the patients were operated in the neonatal period. The 5 patients were also diagnosed with tuberous sclerosis, all alive at the time of this report. Fibroma: It was identified in 3 patients, 1 in preschool age and 2 at school-age, 1 of the patients with tumor in left ventricular septum, 1 patient with tumor on the right interventricular septum in proximity to the moderator band and 1 in the free wall of the left ventricle (deceased because of acute pulmonary edema). The predominant clinical picture consisted of arrhythmias (ventricular tachycardia) and breathed into mesocardium of the precordial area. In the 2 living patients the surgical resection was curative, finding them asymptomatic at the time of this report. There were no associated pathologies in any of the 3 patients. Myxomas: it was detected in 3 patients, all of them at school age and female. Clinical symptoms characterized by general malaise, presence of heart failure and mitral systolic murmur in the precordial area, arrhythmias presented were supraventricular tachycardias. The location of the tumor was in the left atrial septum in all 3 cases. In 1 patient association was found with Carney complex, 2 cases were sporadic presentation. In all the 3 cases the tumor resection was curative. At the time of the report no symptoms were found in the cardiovascular system.
Surgical and Perioperative Data
The surgery was performed on average 35 days after the clinical diagnosis, and all of them had cardiopulmonary bypass support. Average time: 110 minutes of cardiopulmonary bypass, aortic clamping of 47 minutes, hospital stay of 14 days, endotracheal intubation of 4 days stays and seven days in the Intensive care unit (ICU). Regarding the surgical technique, in all cases bicaval cannulation was performed, in patients with atrial myxoma the septum was repaired with autologous pericardium patch, in 1 patient with fibroma a repair of a warned interventricular communication was needed with a Dacron patch, in patients with rhabdomyoma no residual defects occurred. The evaluation by echocardiography in the immediate, mediate and late postoperative reported ventricular function and normal ejection fraction in all the patients who survived. No residual shunts were reported.
Mortality was 9% (1 patient) due to left ventricular dysfunction secondary to a wide resection of the tumor that involved both the free wall and left interventricular septum, the patient died in the immediate postoperative. Morbidity was 27% (3 patients) consisted of pneumonia caused by Staphylococcus aureus, Moraxella catarrhalis and Klebsiella pneumoniae respectively.
Discussion
In this paper the results of surgical resection of primary cardiac tumors in childhood are presented, including the three most common histological types by age and sex like Rhabdomyoma in the neonatal period, fibroma in preschool and school age, and myxomas in school patients. The clinical behavior of tumors corresponded to that reported in the literature [11, 12], the main clinical manifestations were heart failure, arrhythmias, impaired functional class (prevalence of dyspnea) and auscultation blow in the precordial area. By anatomic site, also it corresponded to the reports in the literature [11, 13], predominantly those in the left cavities in the case of rhabdomyomas, fibromas in the ventricles, and in the case of myxomas at the left atrial. (Figures 1& 2) In 100% of our patients the clinical and anatomical diagnosis corresponded to macroscopic pathologic findings and the type of tumor. Pathologies associated like tuberous sclerosis corresponded in 100% of patients with rhabdomyoma. Fibroid patients had no associated pathologies [13, 14, 15]. Among patients with myxoma one of them was associated with Carney complex (disorder characterized by multiple pigmented skin lesions, endocrine tumors, schwannomas, Myxomas of different locations, including heart and skin as well as some other cancers). It has autosomal dominant behavior, in 70% of cases are inherited, and the remaining 30% present as a de novo mutation. Usually have bad long-term prognosis [11].
complemented by with echocardiogram, previously with a clinical guidance, which we carry out the diagnosis with certainty in 100% of patients, so we do not require any additional study as magnetic resonance angiography or angiotomography.
In the perioperative management the most important aspects were the stabilization strategy of pH to physiological values and hemodiafiltration modified to reduce as much as possible the capillary leakage to the 3rd space, which is particularly important in patients with congestive heart failure.
Conclusion
Early clinical diagnosis of primary cardiac tumors allows curative surgical treatment of them. The emphasis on the initial clinical assessment allows a precise anatomical orientation and a differential tumor type diagnosis at the time of the echocardiographic study. When there is a high clinical suspicion of the pathology and the diagnosis by echocardiography is not determined, angioresonance and / or angiotomography with three- dimensional reconstruction are useful. Prenatal diagnosis in patients with rhabdomyoma is mainly performed during routine obstetric ultrasound and may be referred to by finding fetal cardiac tumor, arrhythmias or hydrops [12]. According to the results presented in this paper, surgical resection has curative results in more than 90% of cases. It is necessary a multidisciplinary team that includes the pediatric cardiologist, hemodynamic, cardio- pediatric surgeon and echocardiographer, all of them should be considered in both clinical and surgical evaluation, as well as in monitoring these types of patients for a better prognosis and quality of life.
References
-
Cigarroa Lopez JA, Garcia Jimenez Y, Yanez Gutierrez L, Jimenez Arteaga S, Martinez Sanchez A, et al. (2005) Rabdomioma cardiaco tratado quirurgicamente con exito y revision de la literatura. Arch Cardiol Mex 75(S3): 113-117.
-
Grinda JM, Chachques JC, Jouan J, Latremouille C, Deloche A, et al. (2001) Left ventricular reconstruction after resection of a large fibroma. Ann Thorac Surg 71(4): 1354-1356.
-
Stratemann S, Dzurik Y, Fish F, Parra D (2008) Left Ventricular Cardiac Fibroma in a Child Presenting with Ventricular Tachycardia. Pediatr Cardiol 29(1): 223-226.
-
Tazelaar HD, Locke TJ, McGregor CG (1992) Pathology of Surgycally excised primary Cardiac Tumors. Mayo Clin Proc 67(10): 957-965.
-
Reynen K (1995) Cardiac Myxomas. N Engl J Med 333(24): 1610-1617.
-
Ipek G, Erentug V, Bozbuga N, Polat A, Guler M, et al. (2005) Surgical Management of Cardiac Myxoma. J Card Surg 20: 300-304.
-
Lee VH, Connolly HM, Brown RD (2007) Central nervous manifestation of Myxoma. Arch Neurol
-
64(8): 1115-1120.
-
Amir O, Merdler A, Shiran A (2001) Bilateral Atrial Myxomas associated with hyperpigmented skin lesions. N Engl J Med 344(12): 938-939.
-
Basson CT, Aretz HT (2002) Case records of the Massachusetts General Hospital, weekly Gonzalez PJ clinicopathological exercises. A 27 year old woman with two intracardiac masses and history of endocrinopathy. N Engl J Med 346(15): 1152-1158.
-
Erdmenger J, Vazquez C, Ortega J (2005) Valor de la ecocardiografia en el diagnostico contemporaneo de tumores cardiacos primarios en pediatria. Arch Cardiol Mex 75(2): 154-158.
-
Briassoulis G, Quezado M, Lee CC, Keil M, Stratakis CA (2012) Myxoma of the ear lobe in a 23-month-old girl with Carney complex. J Cutan Pathol 39(1): 68-71.
-
Lacey SR, Donofrio MT (2007) Fetal Cardiac Tumors: Prenatal Diagnosis and Outcome. Pediatr Cardiol 28(1): 61-67.
-
Leja MJ, Dipan J, Perryman L, Reardon MJ (2011) Resection of left Ventricular Fibroma with Subacute Papillary Muscle Rupture. Tex Heart Inst J 38(3): 279- 281.
-
Narendra RD, Suvro SS, Krishnan U (2008) Resection of ventricular rhabdomyomas in infants presenting with cardiac failure. Cardiol Young 18(6): 635-637.
-
Tasoglu I, Tutun U, Lafci G, Hijaazi, Yener U, et al. (2009) Primary Cardiac Myxomas: Clinical Experience and Surgical Results in 67 Patients. J Card Surg 24(3): 256-259.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study