Early Diagnosis of Risks and Management of Cardiometabolic Diseases: A Case Study
The case study presented underscores the importance of early identification of metabolic risks, effective management, and lifestyle modifications in preventing clinical complications associated with cardiometabolic diseases (CMDs). The individual in the study, a South Asian immigrant, experienced the development of essential hypertension in his mid-50s, leading to left ventricular hypertrophy (LVH) and mild diastolic dysfunction. However, through proactive measures such as early diagnosis of metabolic risks, robust management of cardiovascular disease (CVD), adherence to a heart-healthy diet, and lifestyle changes, he was able to avoid major clinical complications of diabetes and maintain overall well-being until the age of 87. The key takeaways from this case study align with broader public health initiatives aimed at addressing the global epidemic of metabolic diseases. The multifaceted and intricate nature of this problem requires a comprehensive approach that considers various factors contributing to the rising prevalence of these diseases. Primary prevention strategies, which focus on identifying and mitigating risk factors for CMDs before the onset of vascular disease, play a crucial role in curbing the epidemic. The success observed in this case study, highlights the potential impact of proactive management and lifestyle interventions, in preventing and mitigating the progression of cardiometabolic diseases. It emphasizes the need for increased awareness, early screening, and ongoing monitoring of individuals at risk. Additionally, promoting heart-healthy diets and encouraging lifestyle modifications, such as regular physical activity and stress reduction, are essential components of a holistic approach to cardiometabolic health. Despite the positive outcomes demonstrated in this case, the article acknowledges that the global response to preventing both communicable and non-communicable diseases has been tepid, with varying levels of enthusiasm for developing primary prevention strategies across different nations. Addressing this challenge requires coordinated efforts at the individual, community, and policy levels to promote a culture of preventive healthcare. In conclusion, the findings of this case study contribute to the growing body of evidence supporting the efficacy of early diagnosis of metabolic risks, effective management, and lifestyle modifications in preventing clinical complications associated with cardiometabolic diseases. The lessons learned from individual cases can inform broader public health initiatives and underscore the importance of a proactive and comprehensive approach to address the escalating prevalence of metabolic diseases globally.
Introduction
Cardiometabolic diseases such as, hypertension, excess weight, obesity, type-2 diabetes, and vascular diseases have increased in incidence and prevalence worldwide [1, 2, 3, 4, 5, 6, 7, 8]. Known sequalae of events that contribute significantly to the promotion of these conditions leading to acute arterial events include, oxidative stress, inflammation of the blood vessels, obesity, type-2 diabetes, vascular dysfunction, arterial stiffness, subclinical atherosclerosis, growth of atherosclerotic plaques in the major arteries, stenosis of the arteries, activation of platelet and coagulation pathways [9]. Meticulous research conducted by the Framingham Heart Study group, established risk factors for the development of coronary artery disease [10]. The INTERHEART study found that nine easily measurable modifiable risk factors could explain more than 90 percent, the risk of heart attack globally, in all geographical regions and major ethnic groups [11]. They concluded that management of modifiable risk factors will have the potential to prevent most premature myocardial infarctions. Khera and associates from Harvard University, demonstrated that among participants, even with high genetic risk, a favorable lifestyle was associated with a nearly 50% lower relative risk of coronary artery disease [12]. According to a report from the researchers of the Imperial College London, Cardiovascular mortality has declined, and diabetes mortality has increased in high-income countries [13]. Between 1980 and 2009, age- standardized cardiometabolic mortality declined in all 26 industrialized countries. According to these researchers, across 26 countries, lowering risk factor trends may have accounted for 49% (men) and 40% (women) cardiometabolic mortality decline. Despite this knowledge, no country has reduced, reversed or prevented the increase in the incidence of vascular diseases.
The recent Harris Poll conducted on behalf of the American Heart Association, reveals a concerning statistic: only 49% of adults in the United States correctly recognize heart disease as the leading cause of death in the nation. Unfortunately, death rates from heart disease have been on the rise in recent years. An estimated 17.9 million people died from CVDs in 2019, representing 32% of all global deaths. Of these deaths, 85% were due to heart attack and stroke. Experts attribute this lack of awareness to a slow progression, denial, and misplaced skepticism about the disease. In a press conference, Dr. Joseph Wu, the president of the American Heart Association, director of the Stanford Cardiovascular Institute, and Professor of Medicine and Radiology, expressed his dismay at the survey results, emphasizing the significant impact of heart disease that many people fail to grasp (https://medicine.stanford.edu/ news/current-news/standard-news/wu-insights.html). He described the findings as discouraging and somewhat frightening. At the individual level, early diagnosis and effective management are crucial for reducing and preventing metabolic diseases that contribute to the development of acute vascular events such as, heart attacks and strokes. Dr. Wu highlighted the key role of early detection and improved management to address this public health challenge.
The South Asian phenotype presents a unique set of characteristics, including high triglycerides, low-density lipoprotein cholesterol, increased visceral fat, a high propensity for diabetes, and low levels of physical activity. According to Kandula, et al. a Professor of Medicine at UC San Francisco, more than 60% of cardiovascular disease (CVD) patients worldwide, belong to the South Asian descent category [14]. The purpose of presenting this case study is to share observations on this distinctive case (South Asian Phenotype), propose a roadmap for enhancing early diagnosis using both approved devices as well as those in developmental stage, and monitor the impact of treatment, risk management, and lifestyle changes on the progression of cardiometabolic risks. The goal is to contribute to a better understanding of the risks, development of a proactive approach, and to address the prevalence of heart disease, especially among individuals with specific risk factors like the South Asian phenotype.
Case Study
The person (GR) is of South Asian origin, who was born in India (08/23/1937), and migrated to the USA for higher studies in 1965. According to experts, 25% of heart attacks occur under age 40 for people of South Asian origin, and 50% occur under age 50. According to Stanford University Scientists, South Asians develop coronary artery disease up to 10 years earlier than the general population. (https://stanfordhealthcare.org/medical-clinics/stanford- south-asian-translational-heart-initiative/conditions.html). The subject in question, developed early signs of heart dysfunction at the age of 57. During his entire life, his health care was provided by three primary doctors,- 1937-65 (India) 1972-2012 (Minneapolis, Minnesota) 2012 to present Washington DC. The patient is a renowned researcher in the areas of cardiometabolic diseases, as such was willing to undergo approved diagnostic tests as well as those that were in the developmental stages.
Diagnosis of Hypertension and Left Ventricular Hypertrophy
In 1994, during a sightseeing tour in India, subject noticed shortness of breath, while climbing a small hill (300 meters high). Primary physician in Minneapolis (Dr. Azam Ansari) performed ECG tests and determined that probably left ventricular hypertrophy was the cause for observed shortness of breath during uphill climbing. It is worth noting here, that both the patient and primary physician were experts in the area of heart health. Primary physician had board certification in multiple medical specialties (Internal Medicine, Pulmonary Medicine, Gastroenterology and Cardiovascular Medicine). Uncontrolled hypertension is the most common cause of left ventricular hypertrophy (LVH). The blood pressure of the patient was 160/80. It is generally recommended that people over 40, should get frequent checkups for increased blood pressure. Thiazide diuretics and angiotensin-converting enzyme (ACE) inhibitors are the most common combination of antihypertensive medications recommended for such cases [15]. In addition to the routine blood pressure monitoring during clinic visits, both conventional sphygmomanometer as well as ambulatory blood pressure (BP) were used to monitor BP before administering various types of medications, as well as for adjusting the dosage of antihypertensives (Figure 1). Initially a combination of a thiazide diuretic and angiotensin- converting inhibitor was used to arrest and normalize LVH. Once this goal was achieved the use of Enalapril (Vasotec 5 Mg) once daily was recommended.
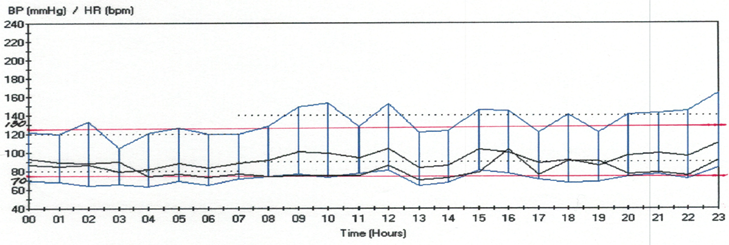
In 2005, ambulatory blood pressure (ABP) was monitored again, for five days (24 hrs.) With a frequency of 30 minutes. Mean low and high values for systolic, diastolic and heart rate are summarized (Figure 1). Of these five days, data for three days included post changing of the dosage of antihypertensive drug (50 Mgs of Atenolol). The quality of 24-hour ambulatory blood pressure monitoring was excellent. No abnormal symptoms were reported. Better systolic blood pressure control was achieved after adding Atenolol a first generation b-blocker. Better control of mean arterial pressure was observed. No significant fluctuations or peaks in blood pressure were observed during the day or at night.
In 2005, in addition to ABP monitoring a complete transthoracic cardiac ultrasound study was ordered to follow the progress or regression of left ventricular hypertrophy, ventricular function and valvular dysfunction. Left atrium was found enlarged at 46 mm. A mild concentric left ventricular hypertrophy was observed. Estimate of cardiac ejection fraction was 75%, which is almost normal for the age. Experts concluded that compared to the previous echocardiographic study done at the University of Minnesota Hospitals in 1996, there seems to be definite evidence for mild left ventricular hypertrophy, mild mitral and aortic regurgitations, left atrial enlargement and diastolic dysfunction. Despite these findings, no stenosis or altered flow dynamics was observed.
Diagnosis of Type-2 Diabetes
Patient visited the Game Park in Tanzania, Africa, during March-April of 1998. During this visit he suffered a spider bite on his neck. It caused necrosis of the skin but healed in a few days. Few weeks after these travels he developed a low-grade fever of unknown origin (FUO) and suffered considerable loss of weight from 153 lbs. to 130. He was administered a wide spectrum antibiotic Levaquin. At the same time, it was noticed that blood sugar also increased to 170 Mgs., per deciliter (dl), hemoglobin A1c (HbA1c) was 7.5%. In addition to the antibiotic, he was administered Glucophage (750Mgs/ day). The low-grade fever persisted for over a year and no definitive diagnosis as to the underlying cause was obtained in spite of thorough diagnostic tests at the Hospitals affiliated with University of Minnesota. Family physicians report stated, “A 61-year-old male admitted for mini laparotomy to diagnose underlying problems of recurrent low-grade fever, weight loss and mild normochromic/normocytic anemia. Earlier he had travelled to Africa and India and had malaria prophylaxis, as well as yellow fever vaccinations. Extensive work out for infective endocarditis, bone marrow pathology, hepatitis B, C and HIV, Cancer antigens, blood culture for bacilli and fungi did not provide any clarifications as to what the underlying cause for this condition is”.
Blood chemistry indicated increased inflammatory markers such as hs-C-reactive protein (hsCRP), and sedimentation ratio, low hemoglobin and hematocrit, and high platelet count. Pathology report indicated mild lymphadenopathy (cluster of enlarged lymph nodes; 1.5 cm) of uncertain etiology, probably of inflammatory origin with mild blunting of the villi and non-caseating granulomas. Despite the advances in our understanding of the immune system, the pathogenesis underlying non-caseating granulomas in chronic inflammatory disease is still poorly understood [16]. The Primary physician at the U of M hospitals recommended a course of Bactrim (Trimethoprim sulfamethoxazole). Since blood chemistry did not improve after a course of antibiotic, patient was advised to continue the use of antibiotic for six months. It took over a year to normalize the blood chemistry. Since the theme of this article is “Cardiometabolic Diseases” we will not describe any more about the origin of “FUO” or its management, suffice it to say, that after years of antibiotic therapy the condition subsided with observed malabsorption of lipids and some nutrients. Other than the FUO, he did have partial intestinal obstructions a couple of times, which resolved without any surgical interventions.
Vascular Dysfunction
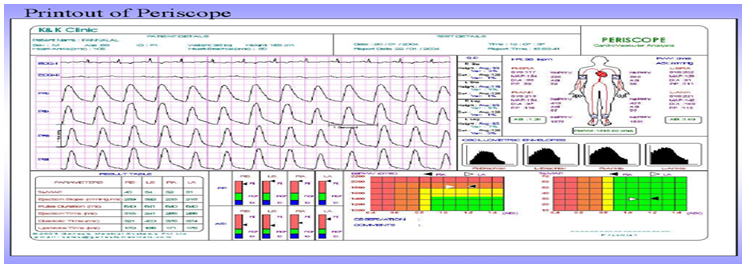
Vascular dysfunction can occur in individuals with hypertension as well as diabetes. Furthermore, impaired insulin action in disorders like diabetes and hypertension, may also play a role in causing endothelial dysfunction within these conditions. Therefore, both hypertension and diabetes can lead to vascular dysfunction, highlighting the importance of managing these conditions effectively to maintain vascular health. Increased vascular oxidative stress in diabetes and hypertension promotes posttranslational oxidative modification of proteins, causing cellular damage and vascular dysfunction. There is increasing evidence that essential hypertension, excess weight, obesity and diabetes are associated with a variety of metabolic abnormalities, including insulin resistance, dyslipidemia, and endothelial dysfunction [17]. This patient had both primary hypertension, LVH and type-2 diabetes. There seems to be a close association between left ventricular diastolic dysfunction and aortic stiffness. Therefore, diagnostic studies were suggested to monitor stiffness of the carotid and femoral arteries as well as for the presence of sub-clinical atherosclerosis. The pulse wave analysis was used for computing stiffness of the arteries using “Periscope” a newly developed device in India, which uses brachial blood pressure and Carotid Femoral pulse wave (PW) to find out Aortic root pressure. Data from a typical analysis is presented for illustration purposes (Figure 2).
Genesis Medical Systems of Hyderabad, India (www. genesismedicals.com), have developed a device, which is a combination of various POC devices on a single platform, which can be used to detect Arterial Stiffness and Ankle-
Brachial Index (Periscope), Autonomic nervous system functions (CanWin; VarioWin), peripheral nervous system (ThesioWin), Pulmonary system (SpiroWin) etc. Pulse wave velocity (PWV) is measured by devices that use either probes or cuffs to noninvasively track the speed of blood flow in meters per second [18]. One measurement is taken at carotid artery and one at femoral artery and the difference is calculated by appropriate algorithms.
Recommendation to measure PWV is included in the recent hypertension guidelines. PWV was determined by PeriScope in an 8-channel real-time PC-based simultaneous acquisition system and analysis system. Patients (GR) blood pressure was 140/80, right brachial PWV was 1265, left brachial PWV was 1260 and pulse pressure was 50 mmHg, age adjusted normal values (Figure 3).

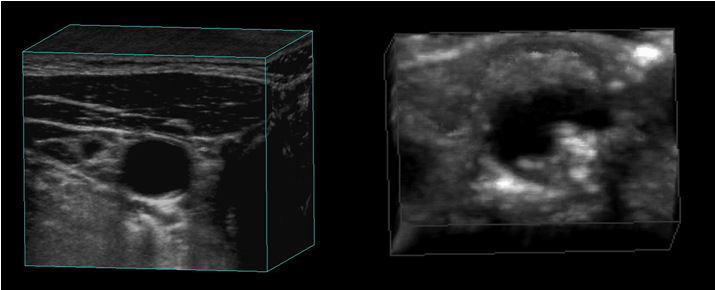
Professor Aaron Fenster and Professor J David Spence at the Robarts Research Institute, Guelph, Ontario, Canada, have developed a cost-effective non-invasive method for direct measurements of carotid atherosclerotic plaques. They have invented and developed a 3-D carotid ultrasound imaging technology (Figure 3), which provides sensitive atherosclerosis measurement tools and appropriate proprietary analytical software to monitor carotid plaque progression and regression by measuring the plaque volume [19]. In 2005, patient visited Robarts Research Institute, in Ontario, Canada and got a carotid scan done by the experts. A 3-D scan of his carotid artery (A-GR) is shown in Figure 4. Compared to a scan of a patient with advanced atherosclerotic plaque (B), his carotid artery was relatively free of any visible plaques. In a bilateral carotid ultrasound doppler study in 2010, minimal homogenous plaque formation was recorded without any flow disturbances.
In 2007, blood chemistry was as follows; Cholesterol 140, Triglycerides 137, LDL Cholesterol 76, VLDL cholesterol 27, Cholesterol HDL ratio 3.7, Fasting glucose 164, HbA1c 7.0, Blood Pressure 140/70. Medications included Metformin ER 500 Mg two tablets/twice daily, Enalapril 10Mg twice daily, Carvedilol 6.5 Mg twice daily, cyanocobalamin 1ml once a month. From 2007 to 2012 the blood glucose levels fluctuated and HbA1c varied from a low of 5.6 to 7.0 depending upon the antiglycemic medications. Patient even participated in a clinical study of twice daily injectable. “Byetta”. Three
different Glucagon Like Peptide (GLP1) agonists were available, exenatide (Byetta ) twice daily, liraglutide (Victoza) once a day, exenatide once a weak (Bydureon) at that time. Victoza seems to lower A1c more than the other two. Once a week exenatide causes less nausea than twice daily. Because of nausea caused by the drug, patient discontinued the use of exenatide and went back to the use of a combination of antiglycemics.
In 2012, post retirement, patient permanently moved to Maryland and the medical records were transferred to the present family physician (Dr. Collin Cullen) in Washington DC. Although he continued the use of Metformin ER and blood pressure medications, Enalapril and Carvedilol, additional antiglycemics were added as and when needed.
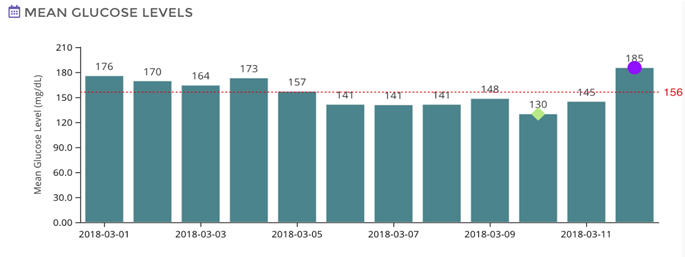
Current medications include Metformin ER 500Mg two tablets twice daily, Lisinopril 20Mg Twice daily, Carvedilol 6.25 Mg twice daily, Glipizide 10Mg twice daily, Jardiance 10 Mg once daily, Rybelsus 7Mg once daily, Atorvastatin 10 Mg once daily, Cyanocobalamin 1000mcg twice a month. Vitamin D 1000 IU daily. In 2018 continuous glucose monitor (CGM) was used to monitor interstitial glucose by the use of Abbott FreeStyleLibre. Data are presented in Figure 5 and Figure 6. A typical glucose profile over a 12-day period is shown in Figure 5. It shows a low of 117 to a high of 205 (daily average 159). In the figure 6, mean daily averages of (96 readings per day) glucose are shown for the twelve days . It shows a low of 130 and a high 185 with an average 156 over the twelve-day period with an estimated HbA1c of 7.2%.
![Figure 5: Mean Daily Glucose values for a period of twelve days (Personal Data) [Data presented shows the daily average of the glucose (159), high (205) and low (117) values] [Courtesy: Dr Santsoh Olety, Karnataka Institute for Endocrinology and Research (KIER)].](/fulltextimages/12198/fig_5.png)
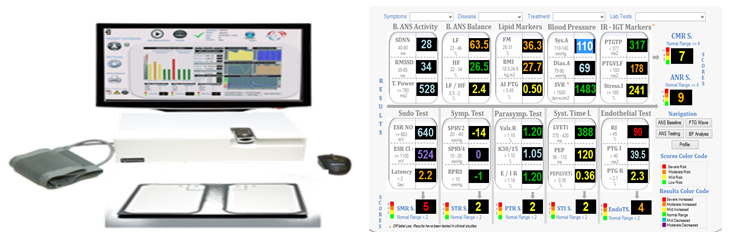
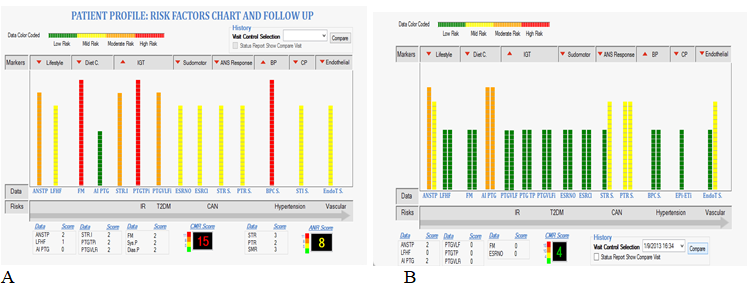
Albert Maarek, Pratiksha Gandhi and Gundu Rao have shown in their earlier work, that TM -Oxi system could be used for early detection of cardiometabolic disorders as well as monitoring the effect of medical treatment on the progression or regression of observed risks [20, 21, 22, 23]. The diagnostic platform used at the IPC Heartcare, Mumbai, India, is a combination of many devices and uses photoplethysmography, spectrophotometry, oscillometry, and galvanic skin response technologies and displays data rapidly. Using proprietary software developed at LD technologies (https://ldteck.com), Miami, Florida, scores for various functional and diagnostic tests are obtained, digitized and displayed color coded (green, yellow, orange and red with increasing risk scores), and printed out graphically as well as digitally (Figures 7 & 8). LD Technologies have developed CAN-PAD for nervous system assessment, VASO-PAD for vascular assessment and LEDA-PAD for podiatry. Figure 8 shows a typical patient risk factor profile in graphic format before (A) and after treatment. (B). Post treatment there is drastic reduction in the cardiometabolic risk (CMR). Patient (GR) has undergone this test many a times to make sure his cardiometabolic risks were within normal limits. No major risks were detected using these non-invasive diagnostic tools.
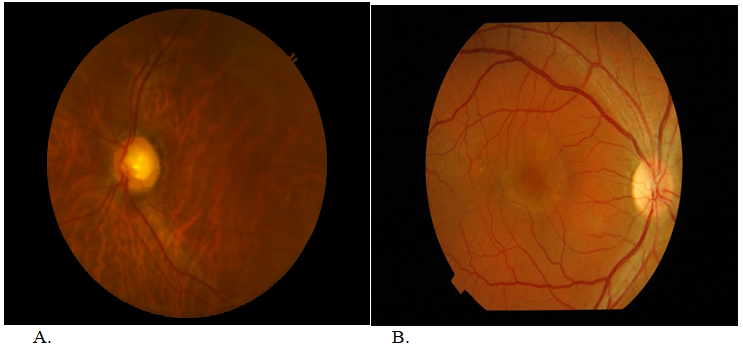
Diabetes induced clinical complications are mainly due to compromised vascular function and include nephropathy, retinopathy, neuropathy and peripheral artery disease in addition to vascular diseases of the heart and brain. Images commonly taken as part of the eye care seems to provide valuable information about patient’s systemic heath [24]. Patient visits ophthalmologists every six months and routine examinations have not revealed any signs of diabetic retinopathy (Figure 9A-GR and Figure 9B-a diabetic smoker).
We used FLIR-E85 series thermal imaging camera, to obtain thermal scans of body surfaces (data presented for hands only) for monitoring thermal variations which are indicators of disturbed blood flow of regional vascular beds. In a routine thermal imaging process, we shoot the video at 30 frames per second for one minute and capture 1800 frames of data. The data thus collected is computed and processed further, using a proprietary software, to obtain patterns of thermal variation, and graded for risk with 1-10, one being no risk and the risk increases with increasing numbers, indicating higher risk [25]. The diabetic, low-risk, individual (A) is an 83 old male (GR), residing in the USA for over half a century, with ten-year prediabetic condition, and 20 years of maturity onset diabetes, undergoing medical treatment which includes following medications,-
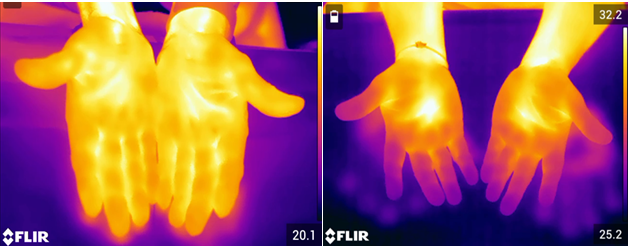
Metformin (2 gm), Glipizide (10mg), Januvia (100mg), Carvedilol (6.25mg), Lisinopril (20mg), and Atorvastatin (10 mg). As is visible in the images (Figure 10), left hand is having an asymmetric temperature pattern for the moderate- risk individual (B). Also, both hands are having colder fingers compared to the low-risk individual (A) indicating signs of peripheral neuropathy. Earlier studies have recommended using skin temperature as guide to monitor neuropathic feet, as well as for rehabilitations [26]. Other methods include using ‘telemedicine mats’ (Podimetrics RTM system, Somerville MA)

to obtain “thermograms”. [27]. According to the UK guidelines of detection and management of peripheral artery diseases, the primary physician should facilitate a ‘definitive’ early clinical diagnosis and guide appropriate urgent or non-urgent referrals, in order to improve the patients prognosis for saving limbs [28]. Patient was referred to a podiatric facility in Potomac, Maryland for consultation. The podiatrician did not conduct any diagnostic tests, instead prescribed an ointment containing lidocaine 3%, Verapamil 15% Diclofenac sodium for application as needed to numb the pain in the toes and sole of the foot.
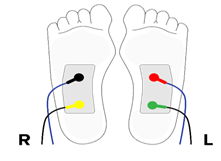
Using a new peripheral artery disease (PAD) detection device under development in Bengaluru, India, studies were done if there were early signs of PAD. The device consisted to two sensors placed on the posterior side of the leg as shown in Figure 11. One sensor provided the initial stimulus, and the other sensor monitored the change in the blood flow velocity over a period of time. The response was monitored continuously for two minutes intervals and graphed for further computations. Initial stimulus recorded greater than 400 arbitrary units Figure 12A whereas subsequent stimulus elicited comparatively less response. Similarly, blood flow dynamics also showed gradually reduced response from a high of 1800 to a low of 1300 Figure 12B, suggesting microvascualr dysfunction.
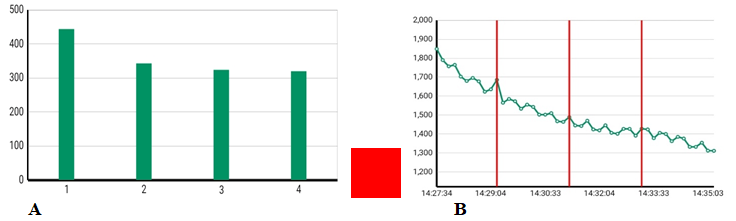
The stimulus induced flow patterns were analyzed by proprietary software and fed back to a source of colored lights,-green, orange or red indicating the relative progress of PAD. In this study, the red dot indicates the presence of PAD. Atherosclerotic occlusive disease involving the leg induces ambulatory function. When symptoms become severe, the clinical manifestation is termed chronic limb threatening ischemia (CLTI) and is characterized by limb pain at rest, nonhealing skin ulcers, or gangrene [29]. The tools available for early diagnosis are relatively few, minimally invasive interventions (use of arterial stents) are evolving rapidly, however, diagnosis capabilities and management of microvascular diseases of the lower limb vessels with CLTI are lacking and need further improvement.
In 2024, at the age of 87, patient underwent following tests to follow the progress of the atherosclerotic arterial disease of the blood vessels, as well as heart health, and vascular function or dysfunction, 1) non-invasive lower limb vascular assessment, 2) bilateral lower limb arterial doppler study, bilateral peroneal and posterior tibial nerve conduction study, 3) carotid artery calcium score, 4) bilateral carotid (neck) Doppler studies, and 5) echo cardiography of the heart. Bilateral iliac, common femoral, popliteal arteries showed diffuse wall thickening, calcification with mild narrowing of lumen. Despite these lesions, blood flow studies showed normal velocity waveforms. Left femoral artery showed wall irregularity and calcified plaques causing 20-30% luminal stenosis. Bilateral anterior tibial and dorsalis pedis arteries showed biphasic waveform, diffused wall thickening, calcification with mild narrowing of the lumen. In the motor nerve, bilateral common peroneal nerve studies showed mildly prolonged latency with mildly reduced compound muscle action potential (CMAP) amplitude and reduced motor conduction velocity. Bilateral posterior tibial nerve studies showed mildly prolonged latency with reduced motor conduction velocity and normal CMAP amplitude. These studies indicate electrophysiological evidence of bilateral lower limb mild sensorimotor axonal with secondary demyelinating neuropathy.
Risk assessment of coronary artery calcium (CAC) score showed significant calcification of the coronary arteries. Number of calcifications in right coronary artery was 3 [Agatston Score (AS) 1007], left main coronary artery 0, Left anterior descending artery 2 (AS 54), left circumflex artery 2 (AS 2748). According to the American College of Cardiology, CAC(AS) score of 100-400 relative risk of 4.3; CAC score of 400-999-relative risk of 7.2, and CAC score > 1000 relative risk of 10.8 [30]. Carotid doppler studies on the other hand, showed multiple eccentric plaques in internal carotid artery (ICA), external carotid artery (ECA), and right carotid bulb. Largest plaques measured 5.6x2.2 mm at right carotid bulb causing no limiting stenosis. Multiple eccentric calcified plaques were seen in left ICA, ECA and left carotid bulb, largest plaque measured 3.6x1.4 mm at left carotid bulb causing no flow limiting stenosis. Thickened intima media was noted on both sides (1.4 mm on right side 1.2 mm on left side). Conclusion of the observation was that spectral wave forms including flow pattern and velocities in the above- mentioned vessels appeared normal with no evidence of significant stenosis of vessels.
2-D Echo and doppler findings of the heart revealed sclerotic aortic valve, trivial mitral valve, and tricuspid valve regurgitation. Left ventricle, mild concentric LVH. Normal LV systolic function. Grade 1 left ventricular diastolic dysfunction. Left atrium normal. Right ventricle and right atrium normal in size, normal right ventricular function. No LV/LA masses, vegetation or thrombus. Main pulmonary artery and aorta are normal. No pericardial thickening or effusion. Ejection fraction 60%. Ejection fraction in a healthy heart is 50% to 70%. However, it is worth noting that ejection fraction can vary with age. An ejection factor of 55 to 65 is considered normal regardless of age, but studies have shown that there can be age-related changes in ventricular volumes and ejection fraction. With advanced age a slight but significant decrease in end systolic volume (ESV), end diastolic volume (EDV) and ejection fraction (EF) has been observed. These findings underline the importance of using age adapted values as standard of reference when evaluating such studies [31]. His blood chemistry was as follows; Cholesterol 99, HDL cholesterol 43, LDL cholesterol 33, Chol/HDL-C 2.3, Triglycerides 133, HbA1c 7.5.
Discussion
Studies done in many countries on South Asian immigrants have demonstrated increased risk for coronary artery disease in this population compared to that of the local ethnic groups [32, 33, 34, 35]. According to American Heart Association News dated My 24, 2018, South Asians living in the U.S., are more likely to die from heart disease, than the general population. But this risk has been largely hidden by a lack of data, researchers say [8]. It is interesting to note, that despite genetic factors, it is possible to prevent premature mortality of this population by appropriate interventions. Khera and associates from Harvard University based on their extensive research concluded that, across four studies involving 55,685 participants, lifestyle factors were independently associated with susceptibility to coronary artery disease [12]. The subject for this case study is a South Asian immigrant, with increased risk for developing cardiovascular disease at an earlier age. He arrived at the young age of 27, with a desire to get advance training in grain science technology. He was healthy, weighed 125 lbs., with a BMI of less than 21. Due to unavoidable circumstances, had to remain in this country and reorient his research field to health sciences (Vascular Biology).
Over the years he gained weight (154 lbs.) and developed hypertension at the age of 57. It is not clear, as to how long the increased systolic pressure was unregulated, as he discovered the presence of this risk when he felt shortness of breath during a climbing expedition. Initially, a combination of a thiazide diuretic and angiotensin-converting inhibitor was used, to arrest and normalize the blood pressure. Later, various medications including first generation b-blockers were tried, and the effect of dosage and medication was followed using ambulatory blood pressure monitoring. For the past two decades, the blood pressure has been in control with a combination of Lisinopril (20Mg) and Carvedilol (6.25Mg). Uncontrolled hypertension led to the precipitation of left ventricular hypertrophy (LVH) and diastolic dysfunction. Although blood pressure has been under control all these years, it seems the mild diastolic dysfunction remains to this day, indicating that risk factor management improves function, but hardly alters or reverses structural damage to the vessels of the heart. It is worth noting, that uncontrolled hypertension even during a short time, can induce LVH, but reversing structural damage to the heart takes a long time. According to experts, maximum reversal of LVH is a time-consuming slow process and the essential goal of antihypertensive therapy should be, not only a reduction in LVH but also a normalization of LV mass, left ventricular size, and diastolic dysfunction [36]. Most recent (2024) echo cardiography of this patient shows, grade-1 diastolic dysfunction (after three decades), no LV/LA masses, and an ejection fraction of 60%. Grade-1diasotlic dysfunction is a slightly impaired diastole and is quite common in persons older than age 60.
At the age of 61 the subject developed impaired glucose tolerance, which resulted in the diagnosis of maturity onset type-2 diabetes. He was put on anti-glycemic drugs, and the blood glucose and glycosylated hemoglobin levels were monitored regularly. The HbA1c levels have been fluctuating between 6.0 to 7.5 depending upon the combination of anti- diabetic medications used. Primary medication has been Metformin ER (500Mg. two tablets twice daily). Later on, glipizide and Januvia were added. At present in addition to Metformin, he is on Glipizide (10Mg once daily). Januvia has been replaced with Jardiance (10Mg, once daily) and Rybelsus (7mg once daily) has been added. Addition of GLP (RA)-1 did reduce the weight considerably (140 lbs.) and lowered HbA1c as expected. Considering his advanced (87) age, no further attempts have been made to bring down the HbA1c further. Although no major clinical complication related to diabetes, such as retinopathy, nephropathy, neuropathy has been noticed, regular six months checkups are recommended to monitor the progress of the vascular disease. In addition, he is undergoing annual screening of bilateral carotid artery (neck) color flow Doppler and 2-D echo cardiography of the heart, to track the advancement of vessel wall disease and monitor his heart health.
Regular follow-up of the functioning of the carotid arteries of the neck and heart shows gradual changes of the vessel wall as well as development of subclinical atherosclerosis. Intimal thickness as well as calcification is evident. Atherosclerotic plaques have been detected in the various regional vascular beds. Narrowing of lumen of the vessels have been recorded. Despite these lesions in the vessel walls, there seems to be no flow disturbances are stenosis. According to the experts, all of the lesions diagnosed are age related. High coronary calcium score (>1000 AS) of right coronary artery and circumflex artery is of concern. However, it has been noted that in mid-to long -term follow up, statin therapy increases the CAC score as documented by a serial non-contrast CT, suggesting that the plaque stabilizing effect of statins may be reflected in a higher CAC score. Patient has been taking statins over a decade and his cholesterol and LDL have come down considerably (Chol 140, LDL 76 in 2007 Vs Chol 99, LDL 33 in 2024). Statin therapy seem to modestly accelerate calcification of plaques leading to more stable, lower-risk compositions and sometimes an acceleration of Agatston CAC score progression [37, 38, 39]. Experts are of the opinion, that CAC (As) score >1000 warrants intensifying lipid lowering therapy to secondary prevention levels and introducing other preventive medicines-GLP1Ras, if diabetes present or adding icosapent ethyl [(VASCEPA)-Eicosapentaenoic acid, EPA]. Patient is already on GLP1Ras, icoaspent ethyl may be added.
In reviewing this case, what we have noticed is the disconnect between the management of known risk for metabolic diseases, versus lack of attention for prevention of possible clinical complications associated with metabolic diseases such as diabetes. As an example, in this study the patient who is diabetic has noticed some changes related to diabetic neuropathy. Has noticed tingling of the toes, heat in the sole of the foot, minor pain in the sole of the resting foot. The diagnostic tests that were available were limited to macro vasculature. No definite test was available for looking at the microvascular flow changes in the sole of the feet. Recently, Gandhi and associates have used pulse wave methods to measure the ankle and toe brachial indices as new markers for early detection of lower extremity peripheral artery disease, similar to some of our earlier studies on diabetes [40, 41]. Toe systolic pressure < 60mmHg indicates significant ischemia and <30mmHg indicates critical limb threatening ischemia. We have discussed in our earlier studies, the need for better flow sensor-based devices for monitoring flow velocity in microvasculature of the peripheral vasculature [42]. We are discussing possibilities of developing a flexible flow-sensor based device with Cardiac Design Laboratories (CDL), Bengaluru, India, who have developed a sophisticated monitor for continuous monitoring of cardiac rhythms.
In a typical pulse wave, triphasic signal indicates the vessels are healthy, a reduction in reverse flow and loss of third phase is considered normal part of aging; a monophasic signal indicates presence of disease in arteries (Figure 13). There are flexible flow sensors as well as,
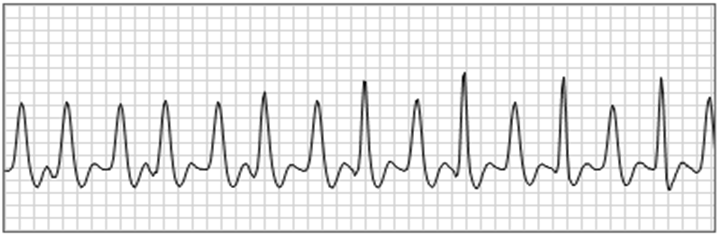
Photo-plethysmography (PPG) sensors, available to measure changes in blood volume at a given site on the body surface. A typical PPG sensor emits light at the tissue site with one or more LEDs. Di photodiode measures the intensity of the non-absorbed light reflected from the tissue. The green LED with short wavelengths are better for certain applications. Such sensors could be used to develop devices that can monitor flow changes of micro vasculature as well as peripheral arteries. Albert Maarek and associates have developed sensors and technologies that can monitor symptoms such as pins-and needles, pricks, tingling and numbness (Figure 14). Foot doctors suggest that the patient should go to foot experts, if there is a change in temperature of 4 degrees F in any part of the sole. However sensitive temperature monitors are not yet available. We feel strongly that there is an immediate need for development of devices to monitor flow dynamics and disturbance in microvasculature of regional vascular beds.
The pathophysiology of atherosclerosis is intricate and forms the basis for promotion of vascular diseases [43]. Earlier, we outlined a series of events that contribute to the advancement of atherosclerosis. Hypertension is one of the leading risk factor that promotes vascular as well as cardiac diseases. Hypertension affects 48% of adults in the US and nearly a billion people worldwide. It is worth noting, that hepatic angiotensin mRNA ‘silencing’, “siRNA” injection once every 6 months, improves adherence and lowers blood pressure in patients with hypertension [44]. Research has demonstrated that reducing LDL-cholesterol with statins decreases the risk of cardiovascular events, supporting the cholesterol hypothesis regarding the origin of atherosclerotic lesions on vessel walls [45]. Additionally, clinical studies have emphasized the role of inflammation in atherosclerosis progression and the occurrence of acute vascular events, independent of lipid-lowering interventions [46]. There is great need for the development effective anti-inflammatory agents. Despite early detection and effective management, this case study highlights the progression of subclinical atherosclerosis as an inherent part of aging. Advanced vascular atherosclerotic lesions represent persistent inflammatory conditions that lead to vulnerable plaque development. Aging is recognized as a significant risk factor for atherosclerosis progression [47]. The implications of this case study resonate globally, particularly with the increasing aging population, prompting a “call for action” for public health organizations and healthcare providers to address the evolving challenges posed by aging-related alterations in metabolism and their contribution to atherosclerotic lesion development in the vasculature [48, 49, 50].
Conclusions
The case study highlights the increased risk of cardiovascular diseases in South Asian immigrants, emphasizing the importance of early intervention and preventive measures. Genetic factors, coupled with lifestyle changes, contribute to a higher susceptibility to conditions like coronary artery disease. The subject’s journey from developing hypertension at the age of 57 to the present controlled state with a combination of Lisinopril and Carvedilol underscores the importance of continuous monitoring and adjustment of antihypertensive medications. Recent findings that a silencing RNA (zilebesiran) injection once every six months produces sustained blood pressure lowering is encouraging (The KARDIA-1 Studies). Despite controlled blood pressure, mild diastolic dysfunction persists, indicating the need for a holistic approach to structural heart damage prevention. The subject’s progression from impaired glucose tolerance to maturity onset type-2 diabetes highlights the challenges of glycemic control. The fluctuating HbA1c levels and the introduction of various anti-diabetic medications underscore the complexity of managing diabetes in an aging population.
The case reveals the development of subclinical atherosclerosis, with detectable changes in carotid arteries and regional vascular beds. The concern over a high coronary calcium score prompts the consideration of intensified lipid- lowering therapy and additional preventive measures. The case draws attention to the lack of attention given to the management of potential microvascular complications in diabetes. Symptoms related to diabetic neuropathy, such as tingling and pain, suggest a need for advanced diagnostic tools to monitor microvascular flow changes. Current diagnostic tests primarily focus on macrovasculature, leaving a gap in identifying early signs of microvascular disturbances of limb extremities. The study emphasizes the urgent need for the development of advanced devices capable of monitoring microvascular flow dynamics and disturbances in regional vascular beds. These devices could aid in the early detection of complications associated with metabolic diseases, enabling timely intervention and preventive measures.
In conclusion, the case study underscores the importance of a comprehensive and personalized approach to managing metabolic diseases, considering both macrovascular and microvascular complications. The development of advanced monitoring devices is crucial for early detection and proactive management, especially in an aging population with a heightened risk of cardiovascular and metabolic conditions.
Acknowledgements
Author expresses his sincere thanks to the following agencies for funding his research for over half a century. Council of Scientific and Industrial Research (CSIR), India 1960-65. Toxicology Training Fellowship (NIH), Department of Pharmacology, University of Minnesota 1971-72. National Science Foundation (NSF), USA 1982-Tarvel grants to visit India for exploration of research collaboration. International Society on Thrombosis and Hemostasis (ISTH) Reach the World Award 1990-93. TOKTEN Fellowship Sponsored jointly by United National Development Program and CSIR, India. 1990-93. National Institutes of Health (NIH) RO1 HL 30127-01A1 1984-86. NIH-NHLBI/STTR 1R41HL081979-01 and 1R41HL079854-01(2005-2007).
References
-
Rao GHR (2023) Editorial: Insights in Diabetes: molecular mechanisms 2022. Front Endocrinol (Lausanne) 14: 1242759.
-
Rao GHR (2018) Cardiometabolic Diseases: A Global Perspective. J Cardiol & Cardiovasc Ther 12(2): ID555834.
-
Nguyen TN, Chow CK (2021) Global and national high blood pressure burden and control. Lancet 398(10304): 932-933.
-
Chong B, Jayabaskaran J, Kong G, Chan YH, Chin YH, et al. (2023) Trends and predictions of malnutrition and obesity in 204 countries and territories: an analysis of the Global Burden of Disease Study. Lancet 57: 1011850.
-
GBD 2021 Diabetes Collaborators (2023) Global, regional, and national burden of diabetes from 1990- 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study Lancet 402(10397): 203-234.
-
Menash GA, Fuster V, Murray CJL, Roth GA (2023) Global Burden of Cardiovascular Disease and Risks, 1990-2022. J The Amer Coll Cardiol 82(25): 2023-2351.
-
Das A, Ambale-Venkatesh B, Lima JAC, Freedman JE, Spahillari A, et al. (2017) Cardiometabolic Disease in South Asians: A global health concern in an expanding population. Nutr Metab Cardiovasc Dis 27(1): 32-40.
-
Volgman AS, Palaniappan LS, Aggarwal NT, Gupta M, Khandelwal A, et al. (2018) Atherosclerotic Cardiovascular Disease in South Asians in the United States: Epidemiology, Risk Factors, and Treatments: A Scientific Statement From the American Heart Association. Circulation 138(1): e1-e34.
-
Rao V, Shankar RT, Rao GHR (2023) Acute Vascular Events: Cellular and Molecular Mechanisms. Int J BioMed 13(3): 9-16.
-
Mahmood SS, Levy D, Vasan RS, Wang T (2014) The Framingham Study and the Epidemiology of Cardiovascular Disease: A Historical Perspective. Lancet 383(9921): 999-1008.
-
Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, et al. (2004) Effect of potentially modifiable risk factors associated with myocardial infraction in 52 countries (the INTEHEART study): case-control study. Lancet 364(9438): 937-952.
-
Khera AV, Emdin CA, Drake I, Natarajan P, Bick AG, et al. (2016) Genetic risk, adherence to a healthy lifestyle, and coronary artery disease. N Engl J Med 375: 2349-2358.
-
Di Cesare M, Bennett JE, Best N, Stevens GA, Danaei G, et al. (2013) The contributions of risk factor trends to cardiometabolic mortality in 26 industrialized countries. Int J Epidemiol 42(3): 838-848.
-
Kandula NR, Kanaya AM, Liu K, Lee JY, Herrington D, et al. (2014) Association of 10-year and lifetime predicted cardiovascular disease risk with subclinical atherosclerosis in South Asians living in America (MASALA) study. J Am Heart Assoc 3: e001117.
-
Kinfe DG, Berhe G, Gidey K, Demoz GT (2020) Blood pressure control, left ventricular hypertrophy and treatment practices among hypertensive patients in Ethiopia. Int G Med 13: 903-916.
-
Timmermans WMC, van Laar M, van Hagen PH, van Zelm MC (2016) Immunopathologies of granulomas in chronic inflammatory diseases. Clin Trans Immunology 5(12): e118.
-
Marwan H, Mario L, Sowers J (1998) Diabetic vascular disease and hypertension. Curr Opinion in Cardiol 13(5a): 298-303.
-
Sridhar Y, Naidu MUR, Usharani P, Raju YSN (2007) Non- invasive evaluation of arterial stiffness in patients with increased risk of cardiovascular morbidity: A cross- sectional study. Ind J Pharmacol 39(6): 294-298.
-
Landry A, Spence JD, Fenster A (2004) Measurement of Carotid Plaque Volume by 3-Dimensional Ultrasound. Stroke 35(4): 864-869.
-
Gandhi PG, Rao GHR (2014) The spectral analysis of photoplethysmography to evaluate an independent cardiovascular risk factor. Int J Gen Med 7: 539-547.
-
Rao GHR, Gandhi PG (2014) Need for a noninvasive diagnosis platform for early detection and management of cardiovascular disorders. View Point. J Clin & Prevent Cardiol 3(3): 93-98.
-
Gandhi PG, Rao GHR (2015) Detection of neuropathy using a sudomotor test in type-2 diabetes. Degener Neurol Neuromuscul Dis 5(5): 1-7.
-
Maarek A, Gandhi PG, Rao GHR (2015) Identifying autonomic neuropathy and endothelial dysfunction in type-11 diabetes patients. Neurology Res 2(2): 63-78.
-
Zekavat SM, Jorshery SD, Rauscher FG, Horn K, Sekimitsu S, et al. (2024) Phenome-and genome-wide analyses of retinal optical coherence tomography images identify links between ocular and systemic health. Sci Transl Med 16(731): eadg4517.
-
Choda G, Rao GHR (2020) Thermal Imaging for the diagnosis of early vascular dysfunctions: A case report. J Clin Cardiol and Diagnostics 3(1): 1-7.
-
Sun PC, Jao SE, Cheng C (2005) Assessing foot temperature using infrared thermography. Foot Ankle Int 26(10): 847-853.
-
Gordon IL, Rothenberg GM, Lepow BD, Petersen BJ, Linders DR, et al (2020) Accuracy of a foot temperature monitoring mat for predicting diabetic foot ulcers in patients with recent wounds or partial foot amputation. Daib Res and Clin Pract 161: 108074.
-
Guidelines for the Assessment, Diagnosis and Management of Peripheral Arterial Disease.
-
Beckman JA (2024) Coming age of device therapy in peripheral artery disease. M Engl J Med Editorial 390(1): 78-79.
-
Neves PO, Andrae J, Monaco H (2017) Coronary Artery Calcium Score: Current status. Radiol Bras 50(3): 182- 189.
-
Fiechter M, Fuchs TA, Gebhard C, Stehli J, Klaeser B, et al. (2013) Age-related structural and functional ventricular values in cardiac function assessed by magnetic resonance. BMC Med Imaging 13: 6.
-
Rao GHR, White JG (1993) Coronary Artery Disease: An overview of risk factors. Ind Heart J 45(3): 143-153.
-
Rao GHR, Kakkar VJ (2001) Coronary Artery Disease in South Asians: Epidemiology, Risk Factors, Prevention. Jaypee Medical Publishers, New Delhi, India.
-
Rao GHR, Thanikachalam S (2005) Coronary Artery Disease: Risk Factors, Pathophysiology and Prevention. Jaypee Medical Publishers, New Delhi, India.
-
Rao GHR (2020) Clinical Handbook of Coronary Artery Disease. Jaypee Medical Publishers. New Delhi, India.
-
Franz IW, Tonnesmann U, Muller JF (1998) Time course of complete normalization of left ventricular hypertrophy during a long-term antihypertensive therapy with angiotensin converting inhibitors. Am J Hypertense 11(6): 631-639.
-
Puri R, Nicholls SJ, Shao M, Kataoka Y, Uno K, et al. (2015) Impact of statins on serial coronary calcification during atheroma progression and regression. J Am Coll Cardiol 65(13): 1273-1282.
-
Nakazato R, Gransar H, Berman DS, Cheng VY, Lin FY, et al. (2012) Statins use and coronary artery plaque composition: results from the International Multicentre CONFIRM Registry. Atherosclerosis 225(1): 148-153.
-
Wannarong T, Parraga G, Buchman D, et al (2013) Progression of carotid plaque volume predicts cardiovascular events. Stroke 44(7): 1859-1865.
-
Gandhi PG, Kamble P (2023) New approach to measuring the ankle toe brachial indices as new markers for early detection of lower extremity peripheral artery disease. J Prevent Med 13(3): 73-86.
-
Uzomba O, Rao GHR (2018) Management of diabetes and Cardiometabolic risks using a novel diagnostic platform. Interven in Obesity & Diab 2(3): IOD.000539.
-
Rao GHR (2016) Flow Velocity, fluid dynamics and vascular pathophysiology. Ann Heart 1(1): 1-18.
-
Xu Y, Zeng Xi, Tu W (2024) Editorial: Pathophysiology, treatment and rehabilitation of atherosclerosis-related diseases in geriatric population. Front Med 11: 1358769.
-
Schiffrin EL (2024) RNA injection every 6 months to improve adherence and lower blood pressure in patients with hypertension. JAMA Editorial 331(9): 733-735.
-
Linton MF, Yancey PG, Davies SS, Jerome WG, Linton EF, et al. (2019) The role of lipids and lipoproteins in Atherosclerosis. In: Feingold KR, Anwalt B, et al. (Eds.), South Dartmouth (MA): MDText.com, Inc.
-
Libby P (2021) Inflammation in Atherosclerosis-No longer a theory. Clin Chem 67(1): 131-142.
-
Zhang L, Connelly JJ, Peppel K, Brian L, Shah SH, et al. (2010) Aging-related atherosclerosis is exacerbated by arterial expression of tumor necrosis factor receptor-1: evidence from mouse modes and human association studies. Hum Mol Genet 19(14): 2754-2766.
-
Rao GHR (2018) Prevention or reversal of cardiometabolic diseases. J Clin Prevent Cardiol 7(1): 22-28.
-
Rao GHR (2018) Predictive and preventive healthcare: Integration of emerging technologies. Point of view. J Clin Res in Diab & Endocrinol 1(1): 1-8.
-
Agrawal A, Rao GHR (2023) Novel approaches for early diagnosis and prevention of cardiometabolic diseases. J Clin & Prevent Cardiol 12(1): 23-36.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study