Association between Frequency of Major Amputations and the Occlusive Pattern of Peripheral Arterial Disease
Introduction: Peripheral arterial disease (PAD) is the leading cause of amputation worldwide. The location of the affected sector could have a certain predictive value regarding the evolution of these patients. Objective: Estimate the association between the frequency of major amputations and the topography of the PAD. Material and method: Observational, descriptive, analytical, retrospective study that estimates the association between the frequency of amputations and the aortoiliac or femoropopliteal topography of PAD, in patients with said diagnosis, hospitalized in the Arteriology service of the National Institute of Angiology and Vascular Surgery (INACV), during the years 2018 and 2019. Results: In a sample of 220 stories, we found that high blood pressure (HBP) and smoking were the most frequent variables, affecting 71.8% and 60.5% of the sample respectively, 40.5% presented an aortoiliac pattern. , of these 55.1% were amputated and 59.5% were femoropopliteal, 58% of which were amputated, for a total of 125 amputations (56.8%). Supracondylar amputation was generally the most performed and infracondylar amputation was performed more frequently in patients with femoropopliteal topography. A more notable influence of smoking on the aortoiliac sector was evidenced. There was a similar probability of amputation for both sectors studied. Conclusions: the type of occlusive pattern did not show an association with the frequency of amputations, nor the time in which it occurs, or with the associated risk factors.
Introduction
Peripheral arterial disease (PAD) occurs due to narrowing or blockage of arterial blood vessels, resulting in impaired blood flow to tissues. Around 70 to 80% of affected patients are asymptomatic, which can delay or hinder early diagnosis and initiation of early treatment, thus improving the chances of a positive evolution of the disease. Intermittent claudication is the path gnomonic sign of PAD and is characterized by pain triggered by walking, in the feet, calves or eventually in the thigh and buttocks of the affected limb, ceasing after rest. A minority of patients progress to critical ischemia or suffer amputation, being more common in men [1]. this pathology includes a range of non-coronary arterial syndromes that are caused by alterations in the structure and function of the arteries at the level of the non-coronary circulation. There are many pathophysiologic processes that can contribute to the formation of occlusions in the non-coronary arterial circulation; however, atherosclerosis obliterans (AEO) continues to be the main cause that affects the aorta and its different branches. The definition of occlusive arterial disease of the lower limbs then refers to any occlusive lesion or stenosis, whether or not it generates a reduction in blood flow to the extremities [2, 3, 4].
Aging is one of the biggest changes in the age pyramid of the human population in recent years. In Brazil, for example, every year, more than 650 thousand people become part of the elderly population. With the aging process of the human population, there is also an increase in the prevalence of chronic diseases such as: diabetes mellitus (DM), high blood pressure (HTN), which in turn constitutes risk factors for PAD.
In addition to aging, other factors influence the increase in chronic diseases such as smoking, alcoholism, unbalanced diet and a sedentary lifestyle. It is estimated that after age 40, the risk of PAD increases two to three times every 10 years [5].
PAD is becoming more common in modern society due, in part, to increased life expectancy. This pathology affected 202 million people worldwide in 2010. The growing interest in early diagnosis has occurred because it is related to atherosclerotic disease in other territories, such as coronary, cerebral, carotid, and increases the risk of cardiovascular events (death, acute myocardial infarction, stroke), of the order of 4 to 6% per year, in patients with the disease. Cardiovascular diseases continue to be the main cause of morbidity and mortality in developed and emerging countries, Brazil being no exception. An example of this is that, in 2006, they represented 29.4% of deaths in that country, while neoplasms were 15.1%. Because it is a chronic disease, the resources required for its treatment are high. In the North American population, the estimated cost per year was $5,955 per patient with a tendency to continue increasing [6].
It is estimated that in the North American population the prevalence of PAD is 4.3%, so by the year 2000, 5 million people were affected and the numbers continue to rise. People in low- and middle-income countries have a moderately low rate of this disease compared to high-income countries. In The Global Burden of Disease study, it is reported that more than 30% of deaths and disabilities were attributed to PAD between 2005 and 2015 and that approximately 1 in 10 people over 70 years of age suffer from it [7]. In Cuba, approximately 1,000 amputations are performed each year, with a prevalence in diabetic patients of 15% and according to reports from the World Health Organization (WHO), amputees represent between 0.25 and 1.25% of the world population [8, 9].
Without a doubt, patients requiring AMI represent a group of seriously ill individuals. They impose a great impact on the health system, especially when more than 150,000 AMI procedures are performed annually around the world [10]. It is vital for the community and for the development of the scientific and health sector to adequately know the behavior of their diseases, more even when it comes to diseases with serious outcomes and high costs for the health system; these are largely preventable, as is the case of chronic peripheral arterial disease. This disease represents a great problem for public health, due to its close relationship with cardiovascular diseases, which in turn represent the leading cause of death in the world, added also to the high costs for its management as it is generally diagnosed in phases. Late stages of the disease. Failure to identify it in a timely manner can lead to decreased quality of life in patients in relation to claudicate-type pain and even the loss of a limb. To the author’s knowledge, many studies show high rates of amputations related to peripheral arterial disease; but its association with different locations has not yet been studied and precisely this motivated our research.
Methodological Design
Type of Study
An observational, descriptive, analytical, retrospective study was carried out, with the objective of ruling out the association between the frequency of amputations and the aortoiliac or femoropopliteal topography of PAD, in patients with said diagnosis, hospitalized in the Arteriology service of the INACV, during the years 2018 and 2019.
Universe or population and sample: Universe: All patients with PAD due to AEO of the aortoiliac or femoropopliteal sectors hospitalized in the Arteriology service of the INACV, during the years 2018 and 2019. Sample: A sample of 220 patients who met the proposed inclusion criteria was selected.
Inclusion Criteria: Patients with a history of PAD due to AEO in Fontaine stages 3 and 4, over 18 years of age, of both sexes. Exclusion Criteria: Patients with incomplete medical records (who do not have the necessary data to carry out this study.
Dependent Variables
Main Output Variable: Frequency of major amputations for each location: Result of the ratio obtained between the number of amputees and the total number of patients for each location. Secondary output variables: Time in which the amputation occurs for each level: Time elapsed for each level of amputation from the moment of diagnosis until the execution of the exerética procedure. Keep in mind that the date of diagnosis will be taken as the date that coincides with the day of the first admission for this pathology, in the medical history. It will be measured in days, months and years. Amputation level for each location: Major amputations according to de Jesús-Silva SG, et al. [11] are generally defined as those performed above the level of the ankle, whether transtibial, transfemoral, knee disarticulations or hip disarticulations. Spoden 12 conceptualizes amputation as the removal of a limb or part of it and establishes the following levels of lower limb amputations: Hemipelvectomy (cut in line with the pelvis, complete removal of the limb). Hip disarticulation. Transfemoral. Knee disarticulation. Transtibial (infracondylar). Ankle disarticulation.
In our work, only major transfemoral (supracondylar) and transtibial (infracondylar) amputations were taken into account as they are the ones most frequently performed due to AI or FP condition secondary to AEO. Distal patterns and minor amputations generally respond to other causes of PAD (which are not the objective of our research), mainly diabetic macroangiopathy and associated risk factors: Clinical- epidemiological factors considered to be associated with lower limb amputation due to PAD [11, 12]. The variables explained below were included here: Age: According to the date of birth recorded in the medical history and will be expressed in years. Sex: According to the patient’s gender: Male and Female. Smoking: According to the WHO, it is a chronic addictive disease associated with tobacco consumption that evolves with relapses. Is considered: Smoker: Person who has smoked at least one cigarette in the last 6 months. Ex-smoker: Person who, having been a smoker has remained abstinent for at least the last 6 months. Non-smoker: A person who has never smoked or has smoked less than 100 cigarettes during their entire life. Personal pathological history: According to pathologies recorded in the medical history: Diabetes mellitus, HBP, dyslipidemia, chronic renal failure, and obesity, others related to the development of PAD.
Independent Variables
Explanation and/or Confusion: Fontaine stage: Only Fontaine stages III and IV were taken into account because they are the terminal phases of the disease that translate into an eminent risk of limb loss. Stage III: It is the pain that appears in the lower extremities of patients in advanced stages of peripheral arterial disease (Fontaine’s y and IV) that tends to manifest during rest. Stage IV: 2 variants of ischemic lesions may occur: Ischemic ulcer: Loss of continuity solution Ischemic gangrene: Mummification of tissue due to tissue death. Occlusive steno pattern: It was determined clinically (by examining the pulses) Aortoiliac Femoropopliteal.
Statistical Analysis
The information was processed on a Dell brand laptop. Microsoft Word and Excel were used to create text, tables and graphics. Data processing was carried out with the Statistical Package for the Social Sciences: IBM SPSS Statistics) version 21.0. The results were presented through summary measures for qualitative variables, such as (absolute and relative frequencies) and quantitative variables such as the mean, standard deviation. To establish the degree of statistical association between the qualitative variables, the Chi square test was used, with a significance level of p < 0.05. The results were presented in tables and graphs for better understanding.
Ethical Considerations
The study was governed by the principles established in the Helsinki codes and the standards of the Council of International Organizations of Medical Sciences (CIOMS), meeting the ethical requirements of value, scientific validity, respect and responsibility [13, 14]. All standards of professional medical ethics were respected in carrying out the study. The data used was collected from the clinical history without any variation and with total confidentiality regarding the identity of the patients and the database of the information obtained; it was protected in compliance with computer security protocols. Authorization to review the patients’ medical records was requested in writing from the center’s management. The work was carried out after being approved by the Research Ethics Committee (CEI) and the Scientific Council of the INACV.
Results
To fulfill the objectives proposed in the study, we included 220 patients. Related to their general characteristics, as shown in Table 1, the variables predominated were HBP (n= 158; 71.8%), smoking (n=133; 60.5%), patients with ischemic lesions (n= 173; 74.1). %), as well as femoropopliteal patterns (n= 131; 59.5%). 56.8% of patients undergo amputation.
| ♯ | Variables | Mean ± SD (N0) | % | IC 95% |
|---|---|---|---|---|
| 1 | Age | 66,3 ± 11,2 | - | - |
| 2 | Female sex | 92 | 41,8 | 35,1 - 48,1 |
| 3 | HTA | 158 | 71,8 | 65,7 - 77,9 |
| 4 | IC | 60 | 27,3 | 21,2 - 33,2 |
| 5 | CVD | 8 | 3,6 | 1,1 - 6,1 |
| 6 | Obesity | 15 | 6,8 | 3,4 - 10,2 |
| 7 | Smoking Habit | |||
| Smoking habit | 133 | 60,5 | 53,9 - 67,1 | |
| Non Smoker | 39 | 17,7 | 12,6 - 22,8 | |
| Former Smoker | 48 | 21,8 | 16,2 - 27,4 | |
| 8 | EO Pattern | |||
| Aortoiliac | 89 | 40,5 | 33,9 - 47,1 | |
| Femoropopliteal | 131 | 59,5 | 52,9 - 66,1 | |
| 9 | Fontaine Stadium | |||
| 3rd grade | 57 | 25,9 | 20,0 - 31,8 | |
| 4th grade | 163 | 74,1 | 68,2 - 80,0 | |
| 10 | Amputees | 125 | 56,8 | 49,7-63,0 |
Table 1: General characteristics of the included patients.
Legend: CI: Confidence interval HTA: Arterial Hypertension Mean ± SD: Mean standard deviation. IC: Ischemic heart disease. CVD: Cerebrovascular disease. EO: Steno-occlusive. AI: Aortoiliac FP: Femoropoplitea. Table 1: General characteristics of the included patients.
Table 2 shows the factors associated with limb amputations in the AI sector. Of the 89 patients included in this location, 49 (n=49; 55.1%) were amputated. The variables that showed a tendency to be a predictor of amputation were: ischemic heart disease, cerebrovascular disease, obesity and Fontaine stage 4. Despite this, none were statistically significant.
| ♯ | Variables | Total (89) | Non-amputees (40) | Major Amputation (49) | P<0,05 |
|---|---|---|---|---|---|
| 1 | Age (Mean±SD) | 65,0 ± 10,6 | 63,6 ± 11,2 | 66,1 ± 10,0 | - |
| Variables | N (%) | N (%) | N (%) | ||
| 2 | Female sex | 35 (39,3) | 14 (35,0) | 21 (42,9) | - |
| 3 | HTA | 63 (70,8) | 26 (65,0) | 37(75,5) | - |
| 4 | IC | 25 (28,1) | 8(20,0) | 17 (34,7) | - |
| 5 | CVD | 4 (4,5) | 1 (2,5) | 3(6,1) | - |
| 6 | Obesity | 8 (9,0) | 2(5,0) | 6 (12,2) | - |
| 7 | Smoking Habit | ||||
| Non smoker | 7 (7,9) | 2 (5,0) | 5 (10,2) | - | |
| Smoker + Former Smoker | 82 (92,1) | 38 (95,0) | 44 (89,8) | - | |
| Fumador | 60 (67,4) | 26 (65,0) | 34(69,4) | - | |
| Former Smoker | 22 (24,7) | 12 (30,0) | 10 (20,4) | - | |
| 8 | Fontaine | ||||
| 3rd grade | 29 (32,6) | 18 (45,0) | 11(22,4) | * | |
| 4th grade | 60 (67,4) | 22 (55,0) | 38(77,6) | - | |
| S No | Variables | Total (131) | No Amputation (55) | Major Amputation (76) | P<0,05 |
| 1 | Age (Mean±SD) | 67,1 ± 11,5 | 69,5 ± 10,2 | 65,4 ± 12,2 | - |
| N (%) | N (%) | N (%) | |||
| 2 | Female sex | 57 (43,5) | 27 (49,1) | 30 (39,5) | - |
| 3 | HTA | 95 (72,5) | 46 (83,6) | 49 (64,5) | * |
| 4 | IC | 35 (26,7) | 15 (27,3) | 20 (26,3) | - |
| 5 | CVD | 4 (3,1) | 2(3,6) | 2 (2,6) | - |
| 6 | Obesity | 7 (5,3) | 3 (5,5) | 4 (5,3) | - |
| 7 | Smoking habit | ||||
| Non smoker | 32 (24,4) | 15 (27,3) | 17 (22,4) | - | |
| Smoker + Former smoker | 99 (75,6) | 40 (72,7) | 59 (77,6) | - | |
| Smoker | 73 (55,7) | 29 (52,7) | 44 (57,9) | - | |
| Former smoker | 26 (19,8) | 11 (20,0) | 15 (19,7) | - | |
| 8 | Fontaine | ||||
| Grade 3 | 28 (21,3) | 10 (18,2) | 18 (23,7) | - | |
| Grade 4 | 103 (78,6) | 45 (81,8) | 58 (76,3) | - |
Table 2: Factors associated with limb amputations with AI injury.
Table 3 shows the factors associated with limb amputations in the FP sector. Of the 131 patients included in this location, 76 (n=76; 58%) were amputated. No variables were found as possible predictors of amputation in this location.
Table 4 shows the factors associated with the steno- occlusive pattern. There were no significant differences in the frequency of amputations in patients in each sector. Infracondylar amputations were performed more in patients with femoropopliteal involvement, while supracondylar amputations were performed in a similar proportion for both sectors. A more notable influence of smoking on the aortoiliac sector was evident compared to the femoropopliteal sector.
| S No | Variables | Aortoiliac (89) | Femoropoplíteo (131) | P<0,05 |
|---|---|---|---|---|
| 1 | Age (Mean±SD) | 65,0 ± 10,6 | 67,1 ± 11,5 | - |
| N (%) | N (%) | - | ||
| 2 | Female sex | 35 (39,3) | 57 (43,5) | - |
| 3 | HTA | 63 (70,8) | 95 (72,5) | - |
| 4 | IC | 25 (28,1) | 35 (26,7) | - |
| 5 | CVD | 4 (4,5) | 4 (3,1) | - |
| 6 | Obesity | 8 (9,0) | 7 (5,3) | - |
| 7 | Smoking Habit | |||
| Non smoker | 7 (7,9) | 32 (24,4) | * | |
| Smoker + Former smoker | 82 (92,1) | 99 (75,6) | - | |
| Smoker | 60 (67,4) | 73 (55,7) | - | |
| Former smoker | 22 (24,7) | 26 (19,8) | - | |
| 8 | Fontaine | |||
| Grade 3 | 29 (32,6) | 28 (21,4) | - | |
| Grade 4 | 60 (67,4) | 103 (78,6) | - | |
| 9 | Amp. Greater | |||
| Total | 49 (55,1) | 76 (58,0) | - | |
| Supra | 43 (48,3) | 56 (42,7) | - | |
| Infra | 6 (6,7) | 20 (15,3) | * |
Table 3: Factors Associated with Steno-occlusive Level.
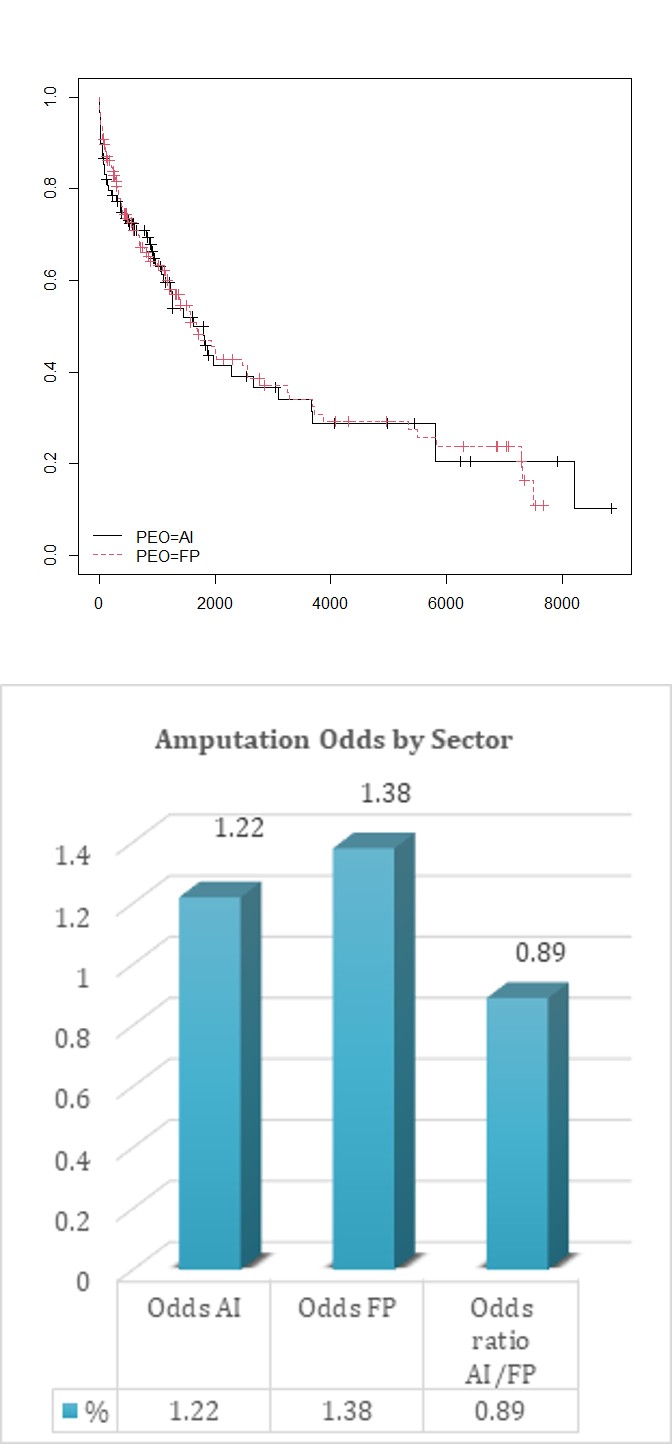
Graph 1: Relationship between the time in which the amputation occurs and the steno-occlusive sector.
Steno-occlusive. Vertical Axis: Probability of amputation Horizontal Axis: Time in days Graph 1 outlines the probability of amputation according to time for each sector. This is composed of two curves that represent the AI and FP sectors. At time zero, that is, at the beginning of the study, the curves are well up and to the left, and this is 100% and means that all of them are without amputation. As time passes, patients are amputated and the curves are lowering. By lowering both together, it shows that the location factor was not important over time for the occurrence of amputations.
Graph 2: Odds: Probability of amputation, in a certain sector. Odds ratio AI/FP: Probability of amputation of the aortoiliac sector with respect to the femoropopliteal sector. Graph 2: For the AI sector, for every 100 people who do not amputate, 122 are amputated, as for the femoropopliteal, 138 are amputated for every 100 who do not do so. The Odds ratio, having a value close to 1, indicates the existence of a similar probability of amputation for each sector.
Discussion of Results
There is a direct relationship between PAD and major amputations, as Aboyans V, et al. [15] and Criqui MH, et al. [16] proposed in their respective studies. The coexistence of risk factors predisposing to vascular disease such as smoking, high blood pressure (HTN), ischemic heart disease (IHD), hyperlipidemia, genetic factors, among others, causes people who suffer from PAD to have a high rate of amputations given that they do not adequately and stably control the risk factors that produce it. Barrios V, et al. [17] in a Consensus of experts carried out in Spain-Barcelona in 2020; agree that smoking and high blood pressure continue to be highly relevant risk factors for the occurrence of PAD, which coincides with what was found in our work.
Frank U, et al. [18] demonstrated in their study that 25- 70% of patients with PAD had atherosclerotic heart disease, with a higher risk of presenting multivessel disease, 14-19% had carotid stenosis greater than 70%, among 10 -23% had renal artery stenosis and increased risk of death. Our research supports what was confirmed by this author regarding the presentation of ischemic heart disease in the AI sector, by demonstrating a predominance of this pathology among amputees in this location, despite not being statistically significant. We did not study the rest of the variables that this author studied. Criqui MH, et al. [19] during the Council on Epidemiology and Prevention of Atherosclerosis of the American Heart Association demonstrated the incidence of cardiovascular disease such as acute myocardial infarction in patients with PAD of up to 14.9% of patients with said pathology, however, In our work we found a greater presence of ischemic heart disease in the patients studied, probably because other clinical modalities of this disease were included.
In Mexico, some risk factors linked to peripheral arterial disease in non-diabetic patients include high blood pressure, smoking and dyslipidemia, a behavior similar to reports in the medical literature and to our work. 4 Another investigation on the general prevalence of peripheral arterial disease carried out by Sikes JM, et al. [20] concluded that it is more prevalent in men than in women, especially in the younger population, since at very advanced ages practically no differences are achieved. Between both groups. Furthermore, the prevalence in men was higher in the more severe degrees of involvement (critical ischemia). It was estimated that the prevalence of intermittent claudication in the 60-65 year old group was 35%. However, in the population 10 years older than 70-75 years, the prevalence increased to reach 70%. Similar results were obtained in our study where men with PAD prevail, both amputees and non-amputees, with fewer differences between sexes in amputees in the AI sector, as well as there is an increase in the percentage of presentation of this ailment for those over 60 years of age. In fact, both in a general sense and by sectors, in our research, the average age of patients always exceeds the sixth decade of life. These results are similar to those obtained by Garcia M, et al. [21] who showed a mean age of 72 ± 13 years, with 79% corresponding to the male sex. Alonso BMJ, et al. [22] who in a prospective study where 45 patients with peripheral arterial disease were included, found a mean age of 68 years and a male/female ratio of 3:1. The same author determined in patients with PAD studied with Doppler ultrasound, 30% diabetic, 37% dyslipidemic, 58% hypertensive and 27% heart disease. We Garcia M, et al. [21], Alonso BMJ, et al. [22] obtained similar results regarding heart disease in the 2 sectors studied and in a general sense.
Ruiz BE, et al. [23] reported that PAD was associated with other pathologies such as arterial hypertension, ischemic heart disease, cerebrovascular ischemia, dyslipidemia and diabetes, as the most important risk factor, according to the dispensarization of non-communicable diseases. Coinciding with our research. De la Puente DLTC, et al. [24] determined the prevalence of classic cardiovascular risk factors in patients with chronic ischemia of the lower extremities upon arrival at a Vascular Surgery Unit. Demonstrating the prevalence of active smoking and high blood pressure with 45% and 59.4% respectively. Higher percentages of HTA were those obtained by this author. Regarding smoking behavior, it is consistent with the results of this report. Kim C, et al. [25] conducted a systematic review of observational studies published between 2008 and 2019. Search terms included “peripheral arterial disease,” “risk factors,” and “amputation-free survival.” This review found that variables such as advanced age, male sex, African-American race, low body mass index, nutritional risk and frailty, comorbidities (CVD, kidney disease, DM, COPD, ischemic heart disease, dementia, wide pulse pressure) , the severity of PAD and its topography, as well as other treatment-related factors, were identified as risk factors affecting amputation-free survival. These results partially coincide with ours in terms of common variables studied, even though the body mass index that Kim associates as a predictor of amputation when it is low, unlike our research where obesity constituted a tendency to predict exeretic surgery in the AI sector.
Venegas RE, et al. [26] in a study to determine the risk factors associated with peripheral arterial disease in patients diagnosed by the ankle-brachial index, the mean age of the population was 58.43 ± 16.69, HBP, DM and dyslipidemia were predictor variables of having an ABI < 0.9. BMI ≥ 25 kg/m2 and sedentary lifestyle, although they were associated in the univariate analysis, did not constitute predictor variables. Coincidentally with our research, age over 60 years and HTN were predominant variables while obesity represented a predictive trend of amputation in the AI sector. Other associated comorbidities such as DM were not included in our research, due to the characteristic profile of patients admitted to the INACV Arteriology service, where hospitalizations of patients with this diagnosis are rare. The age behavior coincidentally coincides with Pichín [27], Martinez, et al. [28] obtained a predominance of male patients while in the study by Nishimura, et al. [29] the female sex was more frequent. In descending order of frequency, HTN was obtained in this study as the most frequent personal pathological history, followed by smoking, DM, dyslipidemia, CKD and a sedentary lifestyle. In the reviewed articles [26, 27, 30, 31, 32] similar frequency data were obtained, unlike Martínez, et al. [28] who obtained 100% smokers in their study. A high prevalence of these diseases is described in the literature; more currently, given the poor dietary habits and lifestyle of the population, all of them are described to a greater or lesser extent related to PAD.
Chen, et al. [32] obtained a positive relationship between overweight and obese patients, with respect to the presence of PAD, coinciding with the present research when studying the behavior of this variable in the AI sector. However, Wassel, et al. [33] did not obtain this relationship. According to the present results, patients suffering from arterial hypertension have a higher risk of developing peripheral arterial disease as a complication. Chen, et al. [32] found a positive relationship between HBP and PAD, coinciding with the results of the present investigation, despite not demonstrating the predictive quality for amputation of this variable in our study, especially in the femoropopliteal sector where it is demonstrated. a statistically significant difference in favor of non-amputees. Smoking, according to Chen, had no statistical relationship with low ABI, contrary to what was obtained by other authors Wassel CL, et al. [33], Yamaki M, et al. [34], Lu Y, et al. [35]. Álvarez, et al. [36] in their study determine the frequency found for smoking (47.3%). This author suggests that smoking constitutes a powerful risk factor for PAD, four times greater in smokers than in non- smokers. In our research, a higher percentage of smokers is obtained, which can be justified by the wide spread of this harmful habit in the Cuban population. It should be noted that in this work a possible association between smoking and PAD was found that was most marked in the IA sector, as in many works on the subject where this independent risk factor is the most associated with this disease [37, 38]. However, an association between this variable and the frequency of amputations could not be demonstrated.
E Castrillón in a study published in 2018 carried out in Southern Colombia, evaluated 158 records of patients between 30 and 95 years old with peripheral arterial disease undergoing lower limb angioplasty. The age of greatest presentation was more than 65 years, coinciding with our study where the average age of presentation of PAD was 61 years. It is also coincidental that HBP is the most commonly presented risk factor among those studied and the femoropopliteal sector is the most affected. The medical literature states that peripheral vascular disease constitutes a high risk of major lower limb amputation in patients without the possibility of revascularization. Exeretic surgery in turn leads to a potentially disabling process, considered worldwide as a significant public health problem. Of all amputations, lower limb amputations are the most common [39]. We agree with the results found in the study carried out by García VR, et al. [40] which included 145 amputee patients, regarding the variables sex (male predominance), HBP and smoking habit (most representative variables among those studied), and regarding the greater representativeness of supracondylar amputations.
Shin JY, et al. [41] conclude after reviewing the 101 publications that support their research, that HBP, IHD, CVD and PAD are the predictor variables of higher rates of major amputation. This author obtained similar results, mainly in the AI sector where IC and CVD showed a certain tendency to constitute predictive variables of amputation, while the amputations performed in our study respond to PAD as a cause. Shin also reports that major amputations are related to the variables, advanced age, more severe ischemia, anemia, sepsis and/or stroke, partially coinciding with our research, as it did not study the variables anemia and sepsis, making it impossible for us to issue a judgment about it. Kennedy G, et al. [42] conducted a two-year retrospective prevalence cohort involving 79 patients undergoing major lower limb amputations. Of the 79 patients, 52 were men and 27 were women. The mean age at the time of surgery was 72 years (range 34-99 years). 58% suffered from diabetes mellitus, 35% from heart failure, and 39% from chronic kidney disease (CKD) and 13% from chronic obstructive pulmonary disease (COPD). Unlike our research, within the coincident variables in our studies, there were a greater number of cases with CKD.
The study by Alijarrah, et al. [43] managed to identify the medical records of patients undergoing major lower limb amputation (MLAM) due to ischemic cause and diabetic foot syndrome (DFS). 140 patients underwent AMMI including 110 below-knee (ADR) and 30 above-knee (AAR) amputations. Unlike our Study in which supracondylar amputation predominated. This is justified by the predominance of diabetic patients in this investigation (89.3%). 61.4% were men, the average age of amputee patients was 63 years (62.1 years for ADR) (66.0 years for AAR). There was a high prevalence of arterial hypertension (80.3%). 46% had ischemic heart disease, 31.6% had congestive heart failure, and 27.7% had cerebrovascular disease. Almost a quarter of the patients had chronic kidney disease (CKD). Furthermore, differentiating from our research are the higher percentages of patients with IC, CVD and CKD, which may respond to an underreporting of cases with these pathologies in our environment. We agree regarding the presentation regarding sex and age.
Regalado F, et al. [44] in their study conclude that the mean age of the patients was 65 ± 15 years and 79 patients (62%) were men; 71 patients (56%) had HTN. Smoking was recorded as a prevalent risk factor in 50% of the patients and 12% more who had already given up the habit at the time of the initial evaluation. 32.57% of patients had extensive lesions. It also reported that in 96 patients, 75.60%, the amputations were performed above the knee and that in 31 patients, 24.40%; the amputations were performed below the knee. In this study, there was a predominance of amputee patients over 65 years of age, 51.1%, and a predominance of smoking amputees 63 for 50%; results are similar to ours. Gómez col.31 in their study, obstructions in the femoropopliteal sector predominated and it was necessary to sacrifice the limb due to amputation of the thigh in 35.6%, contrary to our work where 76 patients were amputated, equivalent to 58% but coinciding with regard to the most affected sector. Furthermore, Gómez reported a predominance of patients with ischemic lesions, 67%, of whom 51.5% had to undergo limb amputation, a result similar to ours, unlike the percentage of amputees with ischemic lesions, which is greater than 70%. In both sectors studied in our study.
In the research by Sereday M, et al. [45], the average age of the amputee population was 62.5 ± 13.0 years.
In non-diabetics, the most frequent amputation is reported to be above the knee for 56.47% of patients, followed by infracondylar amputations with 14.7%; Similar behavior was obtained in our study. Mc Cook, et al. [46] carried out an epidemiological investigation in 218 patients who had undergone major amputation, supra or infracondylar of the lower limbs. 61% of the patients were male and 39% were female [46, 47]. Results similar to ours where, regardless of the sector, more men amputate than women.
The study carried out by Martínez NL, et al. [48] reported that supracondylar amputation was the most performed (in 64.1% of their patients). Depending on sex, we found that it is performed more in women (54.7%) (Unlike of our study where more men amputated), there was a predominance of amputees due to vascular causes and lower limb amputations predominated in the age group of 60 years and over with 84.4% of the cases. 60.9% of amputees were hypertensive and 60.9% of amputee patients were smokers.
In a general sense, with respect to the aforementioned aspects, there is similarity between both studies. Contrary to our research and coinciding with that of Martínez NL, et al. [48] the predominance of female amputees over 60 years of age converges with the findings of other authors, such as Shatnawi NJ, et al. [49]. Martínez NL, et al. [48] also found a higher rate of supracondylar amputation in non-Diabetics, HTN and smoking were the risk factors most commonly identified among patients with major amputation, coinciding with our work.
Hernández DAR, et al. [50] in his study on the behavior of non-traumatic lower limb amputations, found a predominance of diabetes mellitus (60%) and arteriosclerosis obliterans (35%) as the first causes of major amputation. Supracondylar amputations predominated (69%). We obtained identical results despite not including diabetic patients. Cabrera ZJL, et al. [51] in their study of 150 patients who had been admitted to the Arteriology and Diabetic Angiopathy services of the National Institute of Angiology and Vascular Surgery over a period of five years, determined a predominance of male patients (n= 44; 61.97%); and regardless of sex, a greater frequency of patients over 60 years of age. 71 of them underwent major amputation. Supracondylar amputations predominated (69.6%). Similar results are recorded in our research. In the study by Touzard EM, et al. [52] on the tendency towards lower limb amputations, there was a predominance of the male sex with a slightly increasing trend, coinciding with our study. Diabetic Angiopathy and obliterative atherosclerosis were the diseases that most frequently caused amputations, thus reporting the Infracondylar level of amputation in a greater proportion, and their trend was downward in relation to the supracondylar level of amputation, the trend of major amputations was It behaved upwards in those under 60 years of age and downwards in the group aged 70 and over. These results could coincide with ours taking into account the increasing trend of supracondylar amputations, especially in the sixth decade of life.
Aortoiliac disease occurs more frequently after the sixth decade of life. It mainly affects male patients with a predisposition to peripheral arterial disease, exposed to risk factors such as smoking, systemic arterial hypertension, dyslipidemia and obesity, results that we also found. 79 Various studies of clinical cases reveal the association of aortoiliac disease with risk factors such as advanced age, hypertension, smoking and obesity, elements with which we agree. 80.81 In the research study carried out by Martínez J, et al. [53] characterizing aortoiliac steno-occlusive disease, the most frequent risk factors were smoking (73.9%) and high blood pressure (74.4%); The average age was 65 years. We Restrepo RMI, et al. [54], Azañero-Haro J [55] obtained similar Results. Hernández SA, et al. [56] report that in their study the most frequent occlusive pattern was the femoropopliteal in 31 patients for 47.7%, they also reported smoking as the only risk factor present in all the patients studied. We obtained similar results in our research.
Leo S, et al. [57] in a study on the results of hybrid procedures to treat PAD over a period of 5 years, in 87 patients revascularized for this pathology, a higher incidence was demonstrated in males, where involvement of the femoropopliteal sector also predominated, coinciding with with our studio. Cabrera, et al. [39] carried out an investigation about femoropopliteal disease in patients with acute thrombotic arterial ischemia of the lower limbs, in a series of 243 patients over a period of 10 years, finding that major amputation is performed in 74.7 % of patients who presented said acute event. This high percentage of exeretic surgery is justified by the high incidence of atherosclerotic involvement at this level, confirmed in the results of our research where the topography most frequently affected by PAD is the femoropopliteal.
Cheng SW, et al. [16] in a prospective vascular registry consisting of 510 Chinese patients with PAD, revealed a male/female ratio of 1.6:1.0 with a mean age of 72 years. The predominant pattern was femoropopliteal occlusive disease (49%). Half of all patients had tissue loss at presentation. Smoking affected 59%, hypertension (55%). Male patients were mostly smokers (80%) with a higher proportion of aortoiliac disease. We observed great similarity in our research.
Medical literature refers to ischemic manifestations of the lower limbs as the most frequent signs of this disease; it is estimated that it is present in approximately 400 to 450 million patients per inhabitant per year, a worrying fact, since they constitute causes for limb amputations. Sousa PP [58] in his analytical study of patients undergoing lower limb revascularization between 2012 and 2014 found grade IV according to the Leriche Fontaine classification as a predictor variable of amputation and mortality. Our results were identical, mainly at the aortoiliac level [59].
According to the Spanish multidisciplinary consensus guide on peripheral arterial disease corresponding to 2012, none of the studies, since the last 40 years, have altered the impression that only 25% of patients will deteriorate significantly, progressing to clinical states. more serious, which is more frequent in the first year of diagnosis (7-9%) compared to 2-3% annually from the first year onwards. 5-10% of patients with PAD will progress to critical ischemia (defined as grades III and IV of the Fontaine classification), of which 1-3% will require amputation, which represents a rate of 30%30. A similar result is shown by Monteiro, et al. [60] who estimated a mean amputation time of ±27 months and Adame CX, et al. [61] when they state that 30% of patients affected by critical ischemia of the lower extremities suffer a major amputation during the first year after diagnosis. We Monteiro, et al. [60] find something similar in our work, visible through graph 1, which shows the survival curves where precisely the time they persist with a vertical descent (±2 years) coincides with the most accelerated rate of amputations and the point from which they begin. to become horizontal, marks the deceleration of the pace of amputation. It is striking that this deceleration point coincides precisely with 2 years, which could be interpreted as a similarity with previous studies where they estimate an average amputation time from diagnosis, between 12 to 27 months.
The time from the onset of the disease to the occurrence of lower limb amputation is highly variable and multifactorial according to reports in the medical literature, fundamentally motivated by the initial subclinical phase of PAD. For this reason, the data currently available regarding limb survival are limited to describing the behavior of reamputation and not the time elapsed from diagnosis to the performance of the first amputation. This justifies the limited information on the topic that tends to become, in my opinion, totally new or never before studied, when it comes to the relationship between the moment of amputation and steno-occlusive sectors. In recent years, a significant increase in patients consulting for peripheral arterial disease has been observed, especially a high prevalence in the elderly population, with deterioration in quality of life, risk of limb amputation and worse overall survival, due to to the slow and progressive obstruction of the arterial lumen, determining ischemia of the limbs. Its relevance is reflected in the large number of studies carried out. Failure to identify the disease in a timely manner can lead to a decrease in the patient’s quality of life, ranging from claudicate-type pain to the loss of a limb. Added to this, without forgetting its close relationship with cardiovascular diseases, it generates an increase in the patient’s cardiovascular morbidity and mortality, becoming one of the markers of cardiovascular risk worldwide. It is necessary, then, to raise awareness among patients and health-providing entities of the recognition, timely management and care of this silent disease to improve the health of patients and prevent catastrophic outcomes [61].
Conclusion
- The type of occlusive pattern did not show an association with the frequency of amputations, the time in which the amputation occurs, or with risk factors associated with mutilations.
- There was a high frequency of amputated patients (56.8%), with similar percentages for both steno- occlusive sectors.
- The percentage value of supracondylar amputations was similar for both sectors; however, in the femoropopliteal sector the Infracondylar level predominated.
References
-
Camparoto ML, López CR, Marafon CB, Silingovschi GL, Ramos IA, et al. (2019) Peripheral Obstructive Arterial Disease: Description of A Series Of Cases for Medical Professionals. SaBios-Revista 14(1): 27-33.
-
Bolaños DI, Alejandra D, Chaves C, Luisa D, Vanegas G, et al. (2019) Enfermedad Arterial Periférica En Miembros Inferiores. Legal medicine magazine of Costa Rica 36(1): 1-7.
-
(2009) Diagnosis and treatment guide chronic arterial occlusive disease of the lower extremities. Colombian Association of Angiology and Vascular Surgery.
-
[2023] Clinical practice guideline GPC diagnosis and treatment of peripheral arterial disease of the lower limbs. Evidence and recommendations.
-
Mota MI, Mota I, Matheus F, Max O, Villar L, et al. (2020) Occurrence of depressive symptoms in elderly patients with peripheral arterial disease. Health Electronic Magazine Collection 32(1): e1262.
-
De Carvalho Mota T, Diego J, Santos M, De B, Cunha Da Silva J, et al. (2023) Peripheral arterial obstructive disease: integrative review.
-
Castrillon-Peña EL, Poveda-Conde LC, Suaza-Vallejo MC, Vanegas-Vidal M, Barrios-Torres JC, et al. (2019) Experience of lower limb angioplasty in peripheral arterial disease in a private clinic in southern Colombia. Surgery Magazine 71(3): 210-215.
-
Sereday M, Damiano M, Lapertosa S, Cagide A, Bragagnolo JC (2009) Amputaciones de Miembros Inferiores en diabéticos y no diabéticos en el ámbito hospitalario. Revista alad com 13(1): 9-15.
-
Shin JY, Roh SG, Lee NH, Yang KM (2017) Influence of epidemiologic and patient behavior-related predictors on amputation rates in diabetic patients: Systematic review and meta-analysis: Systematic review and meta- analysis. Int J Low Extrem Wounds 16(1): 14-22.
-
Aljarrah Q, Allouh MZ, Bakkar S, Aleshawi A, Obeidat H, et al. (2019) Major lower extremity amputation: a contemporary analysis from an academic tertiary referral centre in a developing community. BMC Surg 19(1): 170.
-
Jesús-Silva SG de, Oliveira JP de, Brianezi MHC, Silva MA de M, Krupa AE, et al. (2017) Analysis of risk factors related to major and minor lower limb amputations in a tertiary hospital. J Vasc Bras 16(1): 16-22.
-
Alonso-Pérez M, Estevan J, Domínguez L (2003) Epidemiology, forms of presentation of occlusive arteriosclerotic pathology of the distal femoral-popliteal sector. Rev Elsevier es 55(S1): S5-S19.
-
(2013) World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. 64th WMA General Assembly. Fortaleza, Brazil, Updated Helsinki guidelines for clinical research get mixed reviews. JAMA pp: 1-4.
-
Cuello Fredes MA, Ramos Vergara P, Etcheverry Borges J (2017) Actualización de las pautas CIOMS. ARS Médica 42(3): 1-5.
-
Aboyans V, Ricco JB, Bartelink MLEL, Björck M, Brodmann M, et al. (2018) ESC 2017 Guide on the diagnosis and treatment of peripheral arterial disease, developed in collaboration with the European Society for Vascular Surgery (ESVS). Spanish Journal of Cardiology 71(2): 111.e1-111.e69.
-
Criqui MH, Aboyans V (2015) Epidemiology of peripheral artery disease. Circ Res 116(9): 1509-1526.
-
Barrios V, Beato P, Brotons C, Campuzano R, Merino- Torres JF, et al. (2022) Comprehensive management of risk factors in peripheral vascular disease. Expert consensus. Rev Clin Esp 222(2): 82-90.
-
Frank U, Nikol S, Belch J, Boc V, Brodmann M, Carpentier PH, et al. (2019) ESVM Guidelineonperipheral arterial disease. Vasa 48(102S): 65-79.
-
Criqui MH, Matsushita K, Aboyans V, Hess CN, Hicks CW, et al. (2021) Lower extremity peripheral artery disease: Contemporary epidemiology, management gaps, and future directions: A scientific statement from the American heart association. Circulation 144(9): e171- 191.
-
Sikes JM, Newmark PA (2013) Restoration of anterior regeneration in a planarian with limited regenerative ability. Nature 500(7460): 77-80.
-
Martínez LG, Fernández-Samos GA, García GA, Pelaz GM, Sierra VA (2017) Diseño, validación y aplicación clínica de un cuestionario de conocimiento (ConocEAP) de los pacientes con enfermedad arterial periférica. Angiología 69(1): 4-11.
-
Alonso MJB, Fueyo RG, Cortés GP, Argueso NA, Pastor FS, et al. (2012) ¿Es útil el eco-Doppler portátil en el diagnóstico de enfermedad arterial periférica? Estudio de validación. Angiología 64(5): 193-198.
-
Ruiz EB, Céniga MVD, Loroño MI, Aguilar CC, Laliena LE, et al. (2010) Factores de riesgo cardiovascular en isquemia crónica de extremidades inferiores: importancia de la intervención del cirujano vascular. Angiología 62(1): 3-8.
-
Triana MME, Rodríguez VLE, Arpajón PY, Almeida HL, Martínez GI, et al. (2017) Enfermedades vasculares periféricas y niveles de calidad de vida en el municipio Diez de Octubre. Rev Cuba Angiol Cir Vasc 18(1): 55-70.
-
Kim C, Yang YS, Ryu GW, Choi M (2021) Risk factors associated with amputation-free survival for patients with peripheral arterial disease: a systematic review. Eur J Cardiovasc Nurs 20(4): 295-304.
-
Rodríguez VEC, Denis PDA, Ávila-Cabreja JA, Hernández- García OL, Vitón-Castillo AA (2021) Factores de riesgo asociados a la enfermedad arterial periférica en pacientes diagnosticados mediante índice tobillo brazo. RevCubanaMed 60(1): e1509.
-
Pichín A, Goulet L, Suárez C, Franco MC (2017) Pacientes con cardiopatía isquémica y enfermedad arterial periférica asintomática determinada mediante el índice tobillo-brazo. Medisan 21(1): 1.
-
Díaz MY, de la CFQL, Zamora JLC, Hernández LA (2018) Calidad de vida en pacientes con enfermedad arterial periférica de miembros inferiores en estadios iniciales. Rev Cuba Angiol Cir Vasc 19(1): 17-27.
-
Nishimura H, Miura T, Minimizada M, Ueki Y, Abe N, et al. (2017) Ankle-brachial index for the prognosis of cardiovascular disease in patients with mild renal insufficiency. Intern Med 56(16): 2103-2111.
-
Filho PJS, Teodoro ECM, Pereira ECA, Miranda VCR (2021) Prevalence of peripheral arterial disease and associated factors in people with type 2 diabetes. Fisioter Em Mov 34: e34122.
-
Crespo-Salgado JJ, Delgado-Martín JL, Blanco-Iglesias O, Aldecoa-Landesa S (2015) Basic guidelines for detecting sedentarism and recommendations for physical activity in primary care. Aten Primary 47(3): 175-183.
-
Chen J, Mohler ER, Xie D, Shlipak M, Townsend RR, et al. (2016) Traditional and non-traditional risk factors for incident peripheral arterial disease among patients with chronic kidney disease. Nephrol Dial Transplant 31(7): 1145-1151.
-
Wassel CL, Ellis AM, Suder NC, Barinas-Mitchell E, Rifkin DE, et al. (2017) Femoral artery atherosclerosis is associated with physical function across the spectrum of the ankle-brachial index: The San Diego Population Study. J Am Heart Assoc 6(7): e005777.
-
Yamaki M, Sato T, Fujii H (2015) Lower ankle-brachial index is associated with poor sleep quality in patients with essential hypertension. Am J Cardiovasc 5(1): 77- 82.
-
Lu Y, Zhu M, Bai B, Chi C, Yu S, et al. (2017) Comparison of Carotid-Femoral and Brachial-Ankle Pulse-Wave Velocity in Association with Target Organ Damage in the community dwelling Elderly Chinese: The Northern Shanghai Study. J Am Heart Assoc 6(2): e004168.
-
Prats AM, Triana Mantilla ME, Rodríguez Villalonga LE, Ramos Morales LE, Arpajón Peña Y (2021) Screening for peripheral arterial disease of the lower limbs in people over 50 years of age. Cuban Rev AngiolCirVasc 22(1): e296.
-
Carter BD, Abnet CC, Feskanich D, Freedman ND, Hartge P, et al. (2015) Smoking and mortality--beyond established causes. N Engl J Med 372(7): 631-640.
-
Rentería E, Jha P, Forman D, Soerjomataram I (2016) The impact of cigarette smoking on life expectancy between 1980 and 2010: a global perspective. Tob Control 25(5): 551-557.
-
Chiriano JT, Abou-Zamzam AM (2015) Lower Extremity Amputations. Essentials of Vascular Surgery for the General Surgeon, pp: 119-132.
-
García VR, Torres Tamayo CN, González Martínez YT, Borroto Pacheco J, Mederos González ME (2017) Clinical and epidemiological characteristics of amputee patients at the General Hospital of Ciego de Ávila. Medigraphic. com 23(4).
-
Shin JY, Roh SG, Sharaf B, Lee NH (2017) Risk of major limb amputation in diabetic foot ulcer and accompanying disease: A meta-analysis. J Plast Reconstr Aesthet Surg 70(12): 1681-1688.
-
Kennedy G, McGarry K, Bradley G, Harkin DW (2019) All-cause mortality amongst patients undergoing above and below knee amputation in a regional vascular centre within 2014-2015. Ulster Med J 88(1): 30-35.
-
Regalado-Solís F, Ziga-Martínez A, Olivares-Cruz S, Sierra-Juárez MÁ, Santillán-Aguayo E, et al. Mortality and perioperative comorbidities in patients with dysvascular amputations. Mexican journal of angiology 49(3): 80-87.
-
Gómez-Márquez GJ (2023) Chronic Obliterations of the Femoral Sector-Poplíteo. Revista médica hondureña 42(3).
-
Sereday M, Damiano M, Lapertosa S, Cagide A, Bragagnolo JC (2009) Amputations of lower limbs in diabetics and non-diabetics in the hospital setting. Revista alad 13(1): 9-15.
-
Mc Cook Martínez J, LopezMaranges L, de Armas Vicent Y, EdreiraPerez J, Gon-zalezGarcia A, et al. (1983) Major amputations of the lower limbs due to vascular causes Epidemiological study. Rev Cub Med 22(6): 516-530.
-
Rodríguez RY, Mayoral RJA (2020) Characterization of the stenocclusive aortoiliac disease. Rev Cuba Angiol Cir Vasc 21(2): e88.
-
Martínez NL, Pérez NC, Martínez FA, Martínez FA, Leonard FD, et al. (2021) Patients with amputation of lower limbs due to vascular causes in Cerro municipality. Rev Cuba Angiol Cir Vasc 22(2): 205.
-
Shatnawi NJ, Al-Zoubi NA, Hawamdeh HM, Khader YS, Garaibeh K, et al. (2018) Predictors of major lower limb amputation in type 2 diabetic patients referred for hospital care with diabetic foot syndrome. Diabetes Metab Syndr Obes. 11: 313-319.
-
Hernández Díaz AR, Acosta Díaz L, Hernández Rojas AL, Moreira Martínez MM, Rodríguez López M (2021) Behavior of non-traumatic lower limb amputations during 2019-2020. Revcienc médicas Pinar Río. 25(3): 5048.
-
Cabrera ZJL, Seara HA, Cisnero VH, Guzmán HM del C, Díaz LM, et al. (2013) Characteristics of major amputations in patients with acute thrombotic arterial ischemia of the lower limbs. Cuban Journal of Angiology and Vascular Surgery 14(1): 1-7.
-
Touzard EM, Peña ZE, Mc Martínez CJ (1994) Trend to major amputations at the National Institute of Angiology and Vascular Surgery. Rev cuba hig epidemiol 32(1/2): 11-18.
-
Martínez J, Díaz JJ, Luján VP, Fernández MR, Ramírez E (2017) Aortoiliac occlusive disease or Leriche syndrome. Rev Colomb Cir 32(3): 214-222.
-
Restrepo RMI, Castro LML, Muñoz PM, Daboín RJ (2018) Clinical case of interest: Leriche syndrome. An unusual manifestation of peripheral arterial disease. Biosalud 17(2): 105-111.
-
Azañero-Haro J (2022) Leriche Syndrome: Underdiagnosis in Peripheral Arterial Disease. Gaceta Médica Boliviana 45(1): 75-78.
-
Hernández SA, Cabrera ZJL, Viña CH, Hondares GMC, Licort LDMGE (2013) Characterization of patients admitted for critical ischemia of the lower limbs. Cuban Journal of Angiology and Vascular Surgery 14(1): 1-13.
-
González-de Leo S, Montbriand J, Eisenberg N, Roche- Nagle G (2022) Results of Hybrid Procedures to treat Peripheral Arterial Disease: experience of one center over 5 years. CirCir 90(5): 610-616.
-
Sousa PP (2022) Analytical Markers That Influence The Results Of Revascularization Surgery In Patients With Peripheral Arterial Disease. SPACV 17(2): 117-124.
-
(2020) Spanish multidisciplinary consensus guide on Peripheral Arterial Disease of the lower extremities. Fesemi.
-
Monteiro HC, Silva V de FA, Ferreira MB, Barbosa D, Martins CA, et al. (2018) Profile of lower limb amputees treated by a reference center: clinical and epidemiological study. RFS 6(1): 38-47.
-
Adame CX, de Ceniga VM, Arietaaraunabeña AC, Fernández GA, Laliena EL (2018) Overall prognosis of patients with critical lower extremity ischemia. Angiology 70(3): 113-119.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study