Unveiling the Therapeutic Landscape of Oseltamivir Exploring Drug Utilization, Adverse Reactions and Interactions with Comorbidities A Prospective Study
Objective: This study aimed to investigate adverse drug reactions (ADRs) associated with Oseltamivir in the presence of various co-morbidities. The objective was to analyze prescription patterns, administration rationale, and ADR prevalence among patients receiving Oseltamivir for therapeutic or preventative purposes. Material and Methods: The study, conducted over six months at St. Philomena’s Hospital in Bengaluru, involved patients of all ages and genders. Ethical approval secured, the research gathered data from diverse sources for 140 patients. Naranjo’s scale was employed for causation, severity, and preventability assessments of Oseltamivir-related ADRs. Descriptive statistics were utilized to compare ADR frequencies between patients using Oseltamivir for prevention and those for therapeutic purposes. Results: The study revealed a 3.57% incidence of Oseltamivir-related ADRs, with co-morbidities contributing to 2.8% of cases, predominantly associated with hypertension. The research shed light on the importance of monitoring ADRs, particularly in the context of co-morbidities during Oseltamivir treatment. Conclusion: This research underscores the importance of monitoring ADRs in the context of co-morbidities during Oseltamivir treatment. The prevalence of hypertension as the most common co-morbidity highlights the need for careful prescription practices, especially for individuals with underlying medical conditions. These findings provide valuable insights into optimizing Oseltamivir usage in diverse patient populations.
Introduction
Oseltamivir is an antiviral drug used for the treatment and prophylaxis of influenza infection caused by viruses A and B [1, 2, 3]. It works by inhibiting the activity of the viral neuraminidase enzyme, which stops viral replication and infectivity. Oseltamivir is available in oral capsule and suspension forms, with the use of oral suspension preferred for pediatric administration [4, 5]. A stable formulation of oseltamivir phosphate as a suspension has been developed, which maintains a high rate of dissolution and stability after reconstitution in aqueous form [1].
Severe dermatologic and mucosal adverse reactions to oseltamivir are rare, but it is important to recognize these uncommon but serious adverse reactions [6]. Oseltamivir ethoxysuccinate, a synthetic derivative of oseltamivir, has been shown to be effective against influenza virus A (H1N1) [7, 8, 9]. Granule formulations containing oseltamivir or its salts have also been disclosed [10, 11]. Oseltamivir has been associated with specific adverse drug reactions (ADRs). One of the ADRs is abnormal behaviors, including fatal outcomes, and sudden death [12, 13]. Another ADR is the risk of developing neuropsychiatric adverse events (NPAE), such as aggressive behavior, restlessness, hallucinations, paranoid ideas, and insomnia. These ADRs are thought to be related to the effects of oseltamivir on the central nervous system (CNS). Oseltamivir, an antiviral medication used for the treatment and prevention of influenza, has been studied for its interactions with various co-morbidities.
One study found that patients on chronic warfarin therapy who received oseltamivir experienced a significant increase in international normalized ratio (INR), particularly within 7-10 days of oseltamivir initiation and in patients with impaired renal function [14]. Another case report described a patient who developed delirium with psychotic and paranoid symptoms after taking oseltamivir, suggesting a potential neuropsychiatric side effect. Additionally, sinus bradycardia was reported in a patient receiving oseltamivir therapy for H1N1 influenza. Another case report highlighted a patient on warfarin who experienced worsening coagulopathy after starting oseltamivir, emphasizing the need for close monitoring of INR in such patients. Overall, while oseltamivir is generally well-tolerated, these studies suggest that it may have interactions and potential side effects in patients with certain co-morbidities.
One study found that patients on chronic warfarin therapy who received oseltamivir experienced a significant increase in international normalized ratio (INR), particularly within 7-10 days of oseltamivir initiation and in patients with impaired renal function [14]. Another case report described a patient who developed delirium with psychotic and paranoid symptoms after taking oseltamivir, suggesting a potential neuropsychiatric side effect [15, 16]. Additionally, sinus bradycardia was reported in a patient receiving oseltamivir therapy for H1N1 influenza [17, 18].
Another case report highlighted a patient on warfarin who experienced worsening coagulopathy after starting oseltamivir, emphasizing the need for close monitoring of INR in such patients [19, 20]. Overall, while oseltamivir is generally well-tolerated, these studies suggest that it may have interactions and potential side effects in patients with certain co-morbidities [21]. In this study, examined the occurrence of ADRs associated with Oseltamivir in relation to co-morbidities at a tertiary care hospital.
Methodology
This prospective observational study was conducted at St. Philomena’s Hospital (a tertiary care hospital), Bengaluru, over a six-month period from July 2020 to August 2020.
Eligibility Criteria: Total, 140 patients receiving Oseltamivir were selected. Ethical clearance was obtained from the Institutional Ethics Committee of St. Philomena’s Hospital. The ethical clearance number was IERB NO: AL- Am/2020/179.
Inclusion Criteria: Inclusion criteria encompassed patients of all ages and genders receiving Oseltamivir for prophylactic or therapeutic purposes.
Exclusion Criteria: Pregnant and lactating women, as well as patients or caregivers unwilling to participate, were excluded.
Study Sampling
All patients (140) receiving Oseltamivir and meeting the inclusion criteria, were approached, informed about and invited to participate by a researcher at St. Philomena’s Hospital (a tertiary care hospital), Bengaluru, over a six- month period from July 2020 to August 2020. During the 6 months of data collection. Data collection from 140 patients was done different methods included patient case sheets, personal interviews with residents/consultants, and information obtained through ward rounds and the medical records department (MRD).
Study Tools
Causality, severity, and preventability of influenza virus and ADRs were assessed using Naranjo’s scale [22]. The Naranjo scale has implications for clinical practice in assessing adverse drug reactions (ADRs) [23, 24]. In daily clinical practice, The Naranjo scale consists of 10 questions, with scores ranging from -1 to +2. The higher the score, the more likely the adverse drug reaction (ADR) is considered to be caused by the drug. Questions with a score of +2 include if the effect occurred after the drug was administered, if it recurred when the drug was re-administered, or if no other explanation could be found. Questions with a score of -1 include if the effect did not develop after the drug was given, if it did not recur when the drug was readministered, if it occurred with placebo, or if an alternative explanation could be found. A score of 1 to 4 is considered a possible ADR, 5 to 8 is considered probable, 9 or greater is considered definite, and 0 is considered doubtful [25].
Results and Discussion
Demographic and Age Distribution
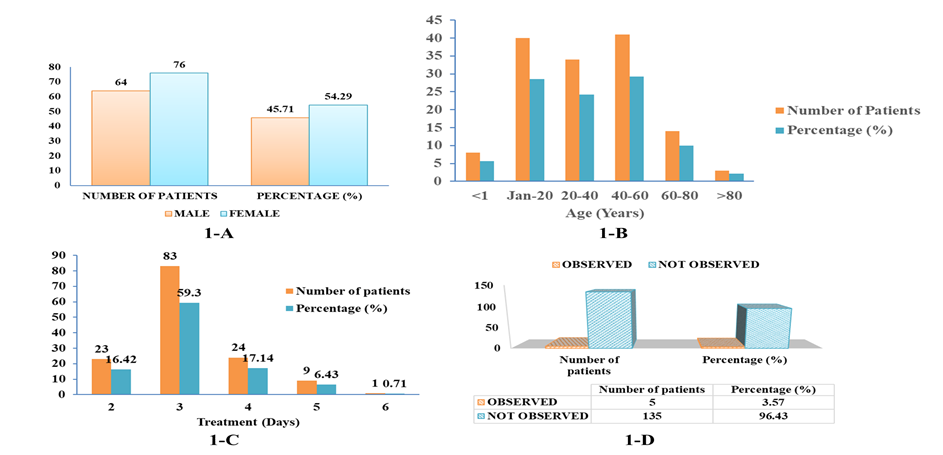
A prospective observational study was carried out at St. Philomena’s hospital for a period of 6 months. The male patient population is lower than the female population with the count of 64 (46.0% approximately) against 76 (54.0% approximately). The age category 40-60 years had the highest number of patients 41, perhaps indicating a higher prevalence of the disease in this age group. Interestingly, the age category >80 years had the lowest percentage (2.14%) and lowest number of patients-3 indicating a possible good health status amongst the elderly or fewer in the population.
The percentage of patients under one year is relatively low (5.71%), possibly due to more robust immune systems at this age or less exposure to risk factors. The age categories <1 and 1-20 years combined had nearly the same percentage (34.28%) as the 40-60 years group. This may warrant further investigation into disease transmission amongst young age groups. The data is mentioned in Table 1 and graphical representation in Figure 1 A & B. This data aligns with existing literature by Zipfel et al, suggesting higher susceptibility among middle-aged individuals [26].
| Number of Patients | Percentage (%) | |
|---|---|---|
| MALE | 64 | 45.71 |
| FEMALE | 76 | 54.29 |
| Age (Years) | ||
| <1 | 8 | 5.71 |
| 20-Jan | 40 | 28.57 |
| 20-40 | 34 | 24.29 |
| 40-60 | 41 | 29.29 |
| 60-80 | 14 | 10 |
| >80 | 3 | 2.14 |
| Duration of Oseltamivir (days) | ||
| 2-Jan | 23 | 16.42 |
| 3-Jan | 83 | 59.3 |
| 4-Jan | 24 | 17.14 |
| ADR observed | ||
| Observed | 5 | 3.57 |
| Not Observed | 135 | 96.43 |
| Co-morbidities | ||
| COPD | 1 | 20 |
| HTN+ DM | 2 | 40 |
| HTN+ ASTH | 1 | 20 |
| No co-morbidities | 1 | 20 |
| ADRs and co-morbidities observed | ||
| Adverse effect | Frequency | Percentage |
| Insomnia | 1 | 20 |
| Nausea | 1 | 20 |
| Redness of eye | 1 | 20 |
| Vomiting | 1 | 20 |
| Dizziness | 1 | 20 |
Table 1: Distribution of patients based on gender and age, adverse drug reactions observed and co-morbidities (COPD-chronic obstr
Duration of Oseltamivir Therapy
Duration of oseltamivir therapy was found to be higher in 83(59.3%) patients with a period of 1-3 days, followed by 24(17.14%) patients with a period of 1-4 days and 23(16.42%) patients with a period of 1-2 days. There’s a sharp decline in the number of patients taking oseltamivir for more than 3 days, with as low as 0.71% of patients following a 1-6day regimen, indicating efficacy within the first 3 days likely. There is a significant drop (from 17.14% to 6.43%) in the percentage of patients taking oseltamivir from 1-4 days to 1-5 days as mentioned in Table 1 & Figure 1C. This suggests that oseltamivir may be effective within the initial three days of therapy, emphasizing the importance of early intervention [27].
Adverse Drug Reactions (ADRs)
Factors that may increase the risk of adverse drug reactions are advanced age, high comorbidities, impaired renal function. Despite the therapeutic effects, studies have shown that use of antiviral can cause undesirable adverse reaction of varying degree of severity. ADR’s increase patients suffering and incur additional charge because of added tests, prolongation of hospital stay and are also the one of the cause of non- adherence. The number of observed ADR patients makes up a small fraction only 5 out of 140, (3.57%).
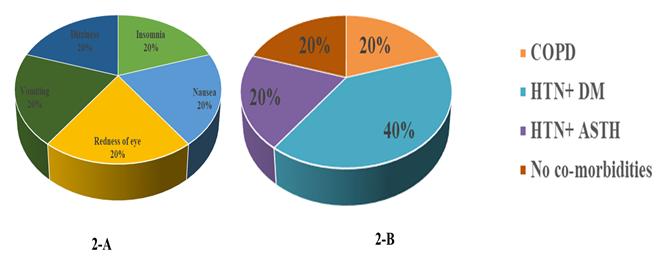
Among 5 ADR’s observed in 5 patients, each one got different ADR’s such as insomnia, nausea, redness of eyes, vomiting and dizziness. This suggests that adverse drug reactions may not be a common occurrence in this data. Conversely, 96.43% of patients did not experience observable ADR Table 1 & Figure 1D, indicating the majority did not have harmful drug interactions or side effects. Insomnia appears as regularly as the other side effects, making up 20.0% of the reported issues.
Might be the medication causing sleep disruption. Nausea, also representing 20.0% of complaints, is a common side effect to watch out for. This implies that digestive disturbances are a common problem. Eye redness also makes up 20.0% of reported issues, possibly indicating a side effect that impacts ocular health as shown in Table 1 & Figure 2A. This suggests that oseltamivir generally has a favorable safety profile. The low ADR percentage might be influenced by reduced medical visits during the pandemic due to fears [1, 28].
Comorbidities and ADRs
Comorbidities associated with adverse drug reactions (ADRs) of oseltamivir include hypersensitivity, gastritis, depression, anxiety, renal disorders, hyperglycemia, and psychiatric disorders [29, 30]. Presence of comorbidities among patients complicates the therapy and increase the risk of drug induces adverse reaction. It was found that out of 5 patients who experienced ADR’s, 4 had comorbidities and hypertension was the most common comorbidity observed. The dataset presents the number and percentage of patients with different comorbidities. It shows that hypertension + diabetes mellitus (HTN+DM) has the highest number of patients with a percentage of 40.0%. On average, there are 1.25 patients per comorbidity with a maximum of 2 and a minimum of 1. The percentage of patients with co-morbidities varies widely, with an average of 25.0%, but ranging from 20.0% to 40.0%. This broad distribution suggests varied prevalence of different co-morbidities as shown in (Table 1 & Figure 2B).
Gender Differences in ADR Reporting
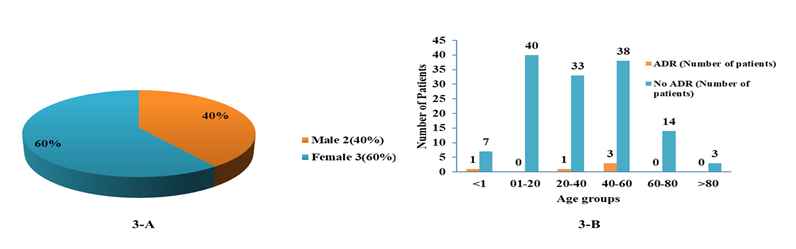
ADR Observed for females is higher than males, which could indicate women are more likely to report ADRs. Females constitute 60.0% of ADR cases, potentially pointing to gender differences in treatment response or usage as shown in table 2 and figure 3-A. Females report a higher percentage of ADRs compared to males due to several factors. Firstly, there are sex differences in the pharmacokinetics and pharmacodynamics of drugs, which can lead to variations in drug metabolism and response [31, 32]. Secondly, women tend to use more medications than men, which increases their exposure to potential ADRs [33, 34]. Additionally, hormonal factors may play a role, as evidenced by the higher prevalence of ADRs in women for drugs affecting the cardiovascular and gynecological systems [35].
| ADR observed | Percentage (%) | |
|---|---|---|
| Male | 2 | 40 |
| Female | 3 | 60 |
| Age group | ADR (Number of patients) | No ADR (Number of patients) |
| <1 | 1 | 7 |
| 20-Jan | 0 | 40 |
| 20-40 | 1 | 33 |
| 40-60 | 3 | 38 |
| 60-80 | 0 | 14 |
| >80 | 0 | 3 |
Table 2: Distribution of ADR’s based on gender and age groups.
Age and ADRs
Most ADR incidents were observed among patients less than 1 year and those between 40-60 years. Perhaps, the immune system’s strength and drug absorption vary at these ages. Surprisingly, aging doesn’t seem to increase ADR incidents significantly. It may reflect the effectiveness of routine health checkups and therapeutic approaches for older patients. Group ‘01-20’ years possessed the maximum number of patients who experienced no ADR as shown in Table 2 and Figure 3B. The absence of a significant increase in ADR incidents with aging may reflect effective health checkups and therapeutic approaches for older patients [36].
Causality Assessment
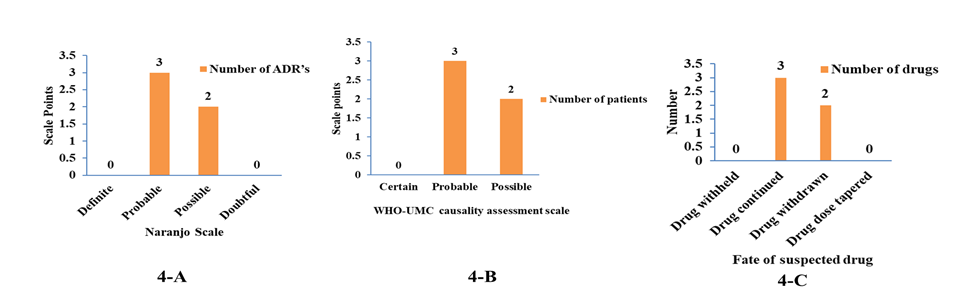
The assessment of the ADR’s was done according to Naranjo causality scale, it was found that 3(60.0%) of ADR’s were assessed as probable, and 2(40.0%) ADR’s were possible. The majority of Adverse Drug Reactions (ADRs) in the data are labeled as ‘probable’ with a count of 3. This suggests that clinicians are quite certain about their diagnoses. Interesting to note, the categories ‘definite’ and ‘doubtful’ have zero counts. This indicates a lack of extreme cases–either absolutely certain or highly questionable ADRs.
- Distribution of ADR’s based on Naranjo scale
- Scale
- Number of ADR’s
- Percentage (%)
- Definite
- 0
- 0
- Probable
- 3
- 60
- Possible
- 2
- 40
- Doubtful
- 0
- 0
- Distribution of ADR’s based on WHO-UMC causality assessment scale
- Causality term
- Number of patients
- Percentage (%)
- Certain
- 0
- 0
- Probable
- 3
- 60
- Possible
- 2
- 40
Table 3: Distribution of ADRs based on Naranjo scale and WHO-UMC causality assessment scale.
There are only 2 ‘possible’ ADRs cases Table 3 & Figure 4A, signifying most ADRs possibly have enough evidence to be judged as ‘probable’. This can improve trust in diagnosis. The assessment of ADR’s was also done according to WHO- UMC causality assessment scale, it was found that 3(60.0%) of ADR’s were assessed as probable, and 2(40.0%) of ADR’s were possible. The majority of Adverse Drug Reactions (ADRs) fall under ‘Probable’ category with a total of 3 cases. This suggests that our drug might have quite a high potential of triggering unwanted reactions. ‘Definite’ and ‘Doubtful’ ADRs are not present in our record, indicating that the cases are not absolutely clear-cut or questionable in their origins [37, 38]. There are 2 ‘Possible’ ADRs reported as shown in (Table 3 & Figure 4B).
Physician Decision Regarding Medication or Drug Fate
The majority of physicians decided to continue the drug (3 out of 5 instances) Table 4 & Figure 4C, rather than withdraw it (2 out of 5). No instances of drug withdrawal or tapering were recorded. Might this indicate that these were not considered viable options in the patient’s situations. With both drug withholding and dose tapering having zero instances, it seems that less disruptive strategies were not being frequently utilized. This suggests that alternative strategies were not frequently considered, possibly due to the perceived necessity of antiviral therapy in these situations [1, 39].
The patient’s medication chart was evaluated for oseltamivir related drug interaction. Out of 140 patients, drug interaction was not observed in majority of the patients and in only one patient with antiplatelet, the interaction was seen i.e., clopidogrel have decreased the level of oseltamivir.
| Number of drugs | Percentage (%) | |
|---|---|---|
| Drug withheld | 0 | 0 |
| Drug continued | 3 | 60 |
| Drug withdrawn | 2 | 40 |
| Drug dose tapered | 0 | 0 |
Table 4: Fate of the suspected drug.
Conclusion
In conclusion, this prospective observational study conducted at St. Philomena’s hospital over a span of 6 months provided valuable insights into the demographic distribution, treatment patterns, and adverse drug reactions (ADRs) associated with oseltamivir therapy. The majority of patients received oseltamivir therapy for 1-3 days, indicating a trend towards shorter treatment durations, possibly due to observed efficacy within the initial three days. The incidence of ADRs was relatively low, with only 3.57% of patients experiencing adverse reactions. Insomnia, nausea, and eye redness were the most commonly reported side effects, emphasizing the importance of monitoring and managing these issues during treatment. Comorbidities, particularly hypertension, were prevalent among patients experiencing ADRs, highlighting the challenges posed by underlying health conditions in antiviral therapy.
The Naranjo causality scale and WHO-UMC causality assessment scale both categorized the majority of ADRs as ‘probable,’ instilling confidence in the diagnostic accuracy. The decision to continue oseltamivir despite ADRs in most cases indicates a perceived necessity of the medication, with withdrawal or tapering rarely considered viable options. In the evaluation of drug interactions, the study found a minimal occurrence, with only one patient experiencing a decrease in oseltamivir levels due to an interaction with clopidogrel. Overall, this study contributes valuable information to the understanding of oseltamivir therapy in a hospital setting, providing a basis for further research and improvement in patient care strategies.
Acknowledgement
Authors want to extend sincere gratitude to all the participants who participated and contributed to this study. First of all, our sincere gratitude to St. Philomena’s Hospital, Bengaluru, for providing the necessary resources and support for conducting this research, Authors are also thankful to Institutional Ethics Committee, for their guidance and approval for the study.
Conflict of Interest
There is no conflict of interest.
References
-
Hanula R, Bortolussi CÉ, Mendel A, Ward BJ, Lee T, et al. (2024) Evaluation of Oseltamivir Used to Prevent Hospitalization in Outpatients With Influenza: A Systematic Review and Meta-Analysis. JAMA Intern Med 184(1): 18-27.
-
Li XG, Chen J, Wang W, Lin F, Li L,et al. (2022) Oseltamivir Treatment for Influenza During the Flu Season of 2018– 2019: A Longitudinal Study. Front Microbiol 13: 865001.
-
Chan RW, Tao KP, Ye J, Lui KKY, Yang X, et al. (2022) Inhibition of Influenza Virus Replication by Oseltamivir Derivatives. Pathogens 11(2): 237.
-
Yao B, Guo Y, Xie Q, Jiang M, Sun F, et al. (2022) Characterization of two excipient interaction degradation products in oseltamivir phosphate powder for oral suspension by MS and NMR. Journal of Mass Spectrometry 57(12): e4899.
-
Karavasili C, Gkaragkounis A, Fatouros DG. (2021) Patent landscape of pediatric-friendly oral dosage forms and administration devices. Expert Opin Ther Pat 31(7): 663-685.
-
Hasson KJ (2022) Innovated formulation of oseltamivir powder for suspension with stability study after reconstitution using a developed ion-pair reversed phase high-performance liquid chromatography method. J Adv Pharm Technol Res 13(3): 177-181.
-
García MJ, Felip E, Plana A, Boada A, Angelats L, et al. (2017) Osimertinib-related skin and mucosal adverse events. Cancer Treat Res Commun 12: 53-55.
-
Harp JL, Kinnebrew MA, Shinkai K (2014) Severe cutaneous adverse reactions: impact of immunology, genetics, and pharmacology. Semin Cutan Med Surg 33(1): 17-27.
-
Siemieniak S, Yoo MJ (2022) Oseltamivir induced oral- only erythema multiforme. Am J Emerg Med 55: 232 e1- 232 e2.
-
Li S, Zhong W, Xiao J, Xie Y, Li X, et al. (2016) Oseltamivir phosphate granule and preparation method thereof. Google Patents EP2005945B1.
-
Lee SJ, Cho JH (2016) Solid pharmaceutical composition comprising oseltamivir free base. Google Patents WO2016003091A1.
-
Asetskaya IL, Polivanov VA, Zyryanov SK (2022) Methodological Approaches to Studying Fatal Adverse Drug Reactions. Safety and Risk of Pharmacotherapy 10(4): 381-395.
-
Marwitz K, Jones SC, Kortepeter CM, Pan GJ, Muñoz MA (2020) An Evaluation of Postmarketing Reports with an Outcome of Death in the US FDA Adverse Event Reporting System. Drug Saf 43(5): 457-465.
-
Smith KR, Bryan WE, Townsend ML, Randolph AE, Vanderman AJ, et al. (2020) Impact of prophylactic oseltamivir on INR in patients on stable warfarin therapy. J Thromb Thrombolysis 50(2): 452-456.
-
Zareifopoulos N, Lagadinou M, Karela A, Kyriakopoulou O, Velissaris D (2020) Neuropsychiatric Effects of Antiviral Drugs. Cureus 12(8): e9536.
-
Shaik AB, Prabhu M, Shenoy S, Thomson SR (2018) Oseltamivir-induced neuropsychiatric symptoms. J Pharmacol Pharmacother 9(1): 43-45.
-
Chahine K, Maria EA, Soufi Y, Chahine C, El Murr T (2019) Oseltamivir-induced bradycardia in an adult patient. Pharm Pharmacol Int J 7(4): 155-156.
-
MacLaren R, Francisco J, Fetters M, Brady J, Kim C, et al. (2021) Oseltamivir-Associated Bradycardia in Critically Ill Patients. Ann Pharmacother 55(11): 1318-1325.
-
Zhang X, Jiao F, Li G, Yu X, Pei Y, et al. (2023) Elevated INR in a COVID-19 patient after concomitant administration of azvudine and anticoagulants. Front Pharmacol 14: 1191608.
-
Shah SP, Patel KM, Subedi R, Gambhir HS (2017) Review of potential drug interaction between Oseltamivir and Warfarin and why it is important for emergency medicine physicians. Am J Emerg Med 35(8): 1207 e3- 1207 e4.
-
Das SK, Shenoy S, Varma M, Rajesh R, Shankar R, et al. ( 2022) A Study of Potential drug-drug interactions in HIV positive individuals with Co-morbidities. Res J Pharm Technol 15(5): 1960-1966.
-
Anovadiya AP, Barvaliya MJ, Shah RA, Ghori VM, Sanmukhani JJ, et al. (2011) Adverse drug reaction profile of oseltamivir in Indian population: A prospective observational study. Indian J Pharmacol 43(3): 258-261.
-
Malbari F, Erker C, Driever PH, Pillay SN, Avery RA, et al. (2022) OTHR-08. Pediatric Neurologic Assessment in Neuro-oncology (pNANO) Scale: A tool to assess neurologic function for Response Assessment in Neuro- oncology (RAPNO). Neuro Oncol 24(1): i148-i148.
-
Murali M, Suppes SL, Feldman K, Goldman JL (2021) Utilization of the Naranjo scale to evaluate adverse drug reactions at a free-standing children’s hospital. PLoS One 16(1): e0245368.
-
Friedman JH (2019) The Naranjo Scale and Tardive Syndromes, a Historical Perspective. Clin Neuropharmacol 42(5): 188.
-
Zipfel CM, Colizza V, Bansal S (2021) Health inequities in influenza transmission and surveillance. PLoS Comput Biol 17(3): e1008642.
-
Qin J, Lin J, Zhang X, Yuan S, Zhang C, et al. (2022) Evaluation of the Clinical Effectiveness of Oseltamivir for Influenza Treatment in Children. Front Pharmacol 13: 849545.
-
Aliyu B, Raji YE, Chee HY, Wong MY, Sekawi Z (2022) Systematic review and meta-analysis of the efficacy and safety of oseltamivir (Tamiflu) in the treatment of Coronavirus Disease 2019 (COVID-19) PLoS One 17(12): e0277206.
-
Ueda N, Umetsu R, Abe J, Kato Y, Nakayama Y, et al. (2015) Analysis of Neuropsychiatric Adverse Events in Patients Treated with Oseltamivir in Spontaneous Adverse Event Reports. Biol Pharm Bull 38(10): 1638-1644.
-
Hama R (2016) The mechanisms of delayed onset type adverse reactions to oseltamivir. Infect Dis (Lond) 48(9): 651-660.
-
Matveev AV, Васильевич МА, Krasheninnikov AE, Евгеньевич КА, Egorova EA, et al. (2022) Gender characteristics of adverse drug reactions development: experience of regional database analysis. Pharmacy & Pharmacology 10(2): 174-186.
-
Shan Y, Cheung L, Zhou Y, Huang Y, Huang RS (2023) A systematic review on sex differences in adverse drug reactions related to psychotropic, cardiovascular, and analgesic medications. Front Pharmacol 14: 1096366.
-
Vries ST, Denig P, Ekhart C, Burgers JS, Kleefstra N, et al. (2019) Sex differences in adverse drug reactions reported to the National Pharmacovigilance Centre in the Netherlands: An explorative observational study. Br J Clin Pharmacol 85(7): 1507-1515.
-
Rydberg DM, Holm L, Engqvist I, Fryckstedt J, Lindh JD, et al. (2016) Adverse drug reactions in a tertiary care emergency medicine ward- Prevalence, preventability and reporting. PLoS One 11(9): e0162948.
-
Castellana E, Chiappetta MR, Cattel F (2018) Gender differences and pharmacovigilance: analysis in the Italian population. Journal of Sex- and Gender-Specific Medicine 4(1): 27-33.
-
Zazzara MB, Palmer K, Vetrano DL, Carfì A, Graziano O (2021) Adverse drug reactions in older adults: a narrative review of the literature. Eur Geriatr Med 12(3): 463-473.
-
Um SH, Abuzgaia A, Rieder M (2023) Comparison of the Liverpool Causality Assessment Tool vs. the Naranjo Scale for predicting the likelihood of an adverse drug reaction: A retrospective cohort study. Br J Clin Pharmacol 89(8): 2407-2412.
-
Shukla A, Jhaj R, Misra S, Ahmed S, Nanda M, et al. (2021) Agreement between WHO-UMC causality scale and the Naranjo algorithm for causality assessment of adverse drug reactions. J Family Med Prim Care 10(9): 3303- 3308.
-
Okada N, Fujiwara N, Azuma M, Tsujinaka K, Chuma M, et al. (2021) Assessment of Adherence to Post-exposure Prophylaxis with Oseltamivir in Healthcare Workers: A Retrospective Questionnaire-Based Study. Biol Pharm Bull 44(6): 869-874.
- Acido Labile or Gastro Irritant Apis and Enteric Release in Galenic Practice: An Overview
- A Study on Knowledge, Attitude and Practice of Hand Hygiene among Healthcare Professionals at a Tertiary Care Hospital, India
- Influence of Inoculum Concentration on In Vivo Incubation Period of Emmia lacerata, Pathogenesis and Management of Wilt in Pepper (Capsicum annuum L.)
- Vanilla’s Chemistry
- Marine Anti-Cancer Compounds and Adverse Effects of Global Warming on Oceans: An Overview
- Serological Investigation of Chikungunya Virus Antibody among Malaria-Suspected Febrile Patients in Some Healthcare Facilities in Rivers State