News Media Coverage of Snakebite Incidence in Nepal during 2010–2022
Background: Despite snakebite being a medical emergency, it is still a neglected health issue in Nepal. Further, there exists gap of knowledge on snakebite epidemiology. Therefore, an analysis of incidence of snakebites reported in news is essential to understand snakebite epidemiology in Nepal and fill up existing knowledge gap in some extent. Objectives: We aimed analysing incidence of snakebites reported in the news media to know whether news-based incidence of snakebite is comparable to the similar incidence reported most comprehensively by Nepal Government, know the snakebite distribution patterns across its geo-climatic regions, provinces, and districts, understand supra-annual variations of snakebite incidence, and measure association between incidences of snakebites with the respective districts’ human population density. Methods: We retrospectively searched and analyzed incidence of snakebites reported in news articles published between 2010 and 2022. Using line graphs and plotted maps, we compared the annual patterns of snakebites with the national data of snakebites reported by Department of Health Services of Nepal Government. Further, we used non-parametric inferential statistics to know representativeness of our dataset and association of snakebite incidence with population density of snakebite prone districts. Results: Snakebites were reported from 53 out of 77 districts of Nepal. People inhabiting 50 out of 53 districts were affected by snakebite envenoming (with 11% of collective envenoming rate) that resulted in deaths of people inhabiting 43 districts (with 15% of collective case fatality rate). The most of envenomings and deaths occurred in the lowlands of Nepal along the northern border of India. We deemed at least 10,339 snakebites, 2,113 envenomings, and 101 deaths annually in Nepal. Conclusions: The incidences of snakebites were high in flood affected areas, terai regions as well as some districts in the hills and mountains. Therefore, improvement of the snakebite risk map released by Nepal Government is essential to ensure prevention and control of snakebite envenoming in these high affected areas. Inclusion of urban areas in terai regions of this country is essential while designing the next more representative community-based study.
Introduction
Snakebite, a neglected tropical disease [1], causes 1.8 to 2.7 million envenomings [2, 3] and 81,000 to 138,000 human deaths annually worldwide [4]. This has significant social and economic impacts in South Asia [2], particularly in India and Pakistan [5] from where remarkably high incidence of snakebite envenomings and deaths are reported. Similar impact can be expected in Nepal where about 20,000 to 37,661 people are bitten by snakes resulting in 1,000 to 3,225 deaths annually [6, 7]. However, there is an epidemiological knowledge gap due to inconsistent and incomplete hospital-based records of admitted snakebite cases [8, 9] and limitations of recently accomplished community-based snakebite studies [10]. While designing the cross-sectional survey in the 23 districts of terai region of Nepal [7], investigators excluded towns and cities from where snakebite envenomings and deaths are frequently reported [11, 12, 13, 14]. This exclusion of agrarian urban areas might distort estimation of the envenoming and mortality rate. Further, the findings from inadequately designed study could not represent the snakebites in the tropical and agrarian terai of Nepal. For the appropriate extrapolations signifying the representativeness of the snakebite burden in Nepal, the news media reported snakebite incidences can provide useful information required to evaluate the epidemiological situation in study areas and design more appropriate epidemiological studies of snakebites across terai, hills, and mountains of Nepal. In Nepal, at least 863 media publish news regularly mainly in Nepali, followed by English and indigenous languages [15]. Although the first print news media “Gorkhapatra” was published in 1858 [16], the online news media coverage of snakebite incidences have been rapidly increased nationwide, particularly after the reinstatement of multiparty democracy in 1990 [17]. Therefore, properly analyzed media-based information can be a cost-effective approach to understand the epidemiological situation in snakebite prone areas and determine the snakebite burden more reliably than the previous comprehensive studies.
Assessing news media-reported snakebite incidence can be a new approach for examining the burden of snakebites and envenomings in different provinces and districts where healthcare facilities are inadequate, although this approach has many advantages and some limitations [14, 18]. Since data from news media are typically available in near real-time and provide earlier estimates of epidemic issues [19], the trend of snakebite envenomings can be understood readily and cost- effectively by analyzing media-reported snakebites.
In Nepal, several communities [7, 20] and hospital- based studies Pandey DP, et al. [12, 21] provided snakebite incidence over less than two years. They did not depict annual variations in snakebites. Next, news media-based analyses included out-of-hospital cases and deaths that do not appear in a hospital-based data set [14] as well as snakebite incidence from urban to rural areas of Nepal [14]. However, there has yet to be an analysis of media-reported snakebite incidences in provinces and districts of this country.
Herein, we analyzed media-reported incidences of snakebites that occurred in Nepal during 13 years to know whether supra-annual variations in incidence of envenoming and deaths exist in this country, determine the prevalence of snakebite envenomings across the districts, provinces, climatic zones, and along the altitudinal gradients, and compare incidences of snakebites, envenomings, and deaths with the most updated reports of Nepal Government. Further, we aimed to determine the size of the population at risk of envenomings and associated deaths. Also, we aimed to know any association between snakebite envenomings and human population density in the snakebite prone districts of Nepal. Therefore, findings from this study can be used to make snakebite envenoming a serious issue in Nepal.
Materials and Methods
Topography, Climate, and Populations Vulnerable to Snakebites in Nepal
Nepal has diversified lands extending 60–8,848 meter (m) above sea level (asl) (Figure 1). The news media- reported snakebite cases represented Nepal’s lowlands featured by a hot tropical climate, with Chure hill ranges having a mild subtropical climate, and Mahabharat ranges having temperate and subalpine climates (Figures 1 & 2).
A total population of Nepal is 29,192,480 (Nepal Population Census 2021) and total population of 53 districts from where snakebite incidence was reported in news, is 24,785,096 i.e., 85% of national population. Federal Democratic Republic of Nepal is divided into seven provinces (the first order administrative units), 77 districts (the second order units), 753 local bodies (the third order units), and 6,443 wards (the last administrative units) since the last eight years (cited in: https://en.wikipedia.org/wiki/Village_development_ committee_(Nepal), accessed in 12 August 2023). Before 2015, the first level administrative units were five development regions, the second level units were 14 zones, the third level units were 75 districts, and the fourth level units were 58 municipalities and 3,157 Village Development Committees (VDCs). Depending on the human populations, each of the VDCs was divided into nine wards which were the last level units.
![Figure 1: Divisions of Nepal’s topography and geographic locations of the major sources for news media-reported snakebites included in this study. The symbol “H” stands for hospitals where patients visited. But, the status of antivenom supply was unclear to us. In legend, the “STCs” stands for Snakebite Treatment Centers and “DRs” stands for Development Regions (The details about sources are mentioned in S2 Table [14]). Those news reported snakebites from 53 districts [that are displayed in numerals 1 through 53 from the eastern to far-western Nepal as: 1: Jhapa; 2: Morang; 3: Sunsari; 4: Ilam; 5: Udayapur; 6: Panchthar; 7: Khotang; 8: Taplejung; 9: Saptari; 10: Siraha; 11: Dhanusha; 12: Mahottari; 13: Sarlahi; 14: Rautahat; 15: Bara; 16: Parsa; 17: Sindhuli; 18: Makawanpur; 19: Chitwan; 20: Dhadhing; 21: Kathmandu; 22: Bhaktapur; 23: Lalitpur; 24: Dolakha; 25: Sindhupalchowk; 26: Nuwakot; 27: Rasuwa; 28: Nawalpur (aka Nawalparasi East); 29: Gorkha; 30: Lamjung; 31: Kaski; 32: Syangja; 33: Parbat; 34: Baglung; 35: Parasi (aka Nawalparasi West); 36: Rupandehi; 37: Kapilvastu; 38: Dang; 39: Banke; 40: Bardiya; 41: Palpa; 42: Pyuthan; 43: Rolpa; 44: Salyan; 45: Surkhet; 46: Dailekh; 47: Humla; 48: Kailali; 49: Kanchanpur; 50: Achham; 51: Doti; 52: Baitadi; 53: Bajhang].](/fulltextimages/11476/fig_1.png)
Figure 1: Divisions of Nepal’s topography and geographic locations of the major sources for news media-reported snakebites included in this study. The symbol “H” stands for hospitals where patients visited. But, the status of antivenom supply was unclear to us. In legend, the “STCs” stands for Snakebite Treatment Centers and “DRs” stands for Development Regions (The details about sources are mentioned in S2 Table [14]). Those news reported snakebites from 53 districts [that are displayed in numerals 1 through 53 from the eastern to far-western Nepal as: 1: Jhapa; 2: Morang; 3: Sunsari; 4: Ilam; 5: Udayapur; 6: Panchthar; 7: Khotang; 8: Taplejung; 9: Saptari; 10: Siraha; 11: Dhanusha; 12: Mahottari; 13: Sarlahi; 14: Rautahat; 15: Bara; 16: Parsa; 17: Sindhuli; 18: Makawanpur; 19: Chitwan; 20: Dhadhing; 21: Kathmandu; 22: Bhaktapur; 23: Lalitpur; 24: Dolakha; 25: Sindhupalchowk; 26: Nuwakot; 27: Rasuwa; 28: Nawalpur (aka Nawalparasi East); 29: Gorkha; 30: Lamjung; 31: Kaski; 32: Syangja; 33: Parbat; 34: Baglung; 35: Parasi (aka Nawalparasi West); 36: Rupandehi; 37: Kapilvastu; 38: Dang; 39: Banke; 40: Bardiya; 41: Palpa; 42: Pyuthan; 43: Rolpa; 44: Salyan; 45: Surkhet; 46: Dailekh; 47: Humla; 48: Kailali; 49: Kanchanpur; 50: Achham; 51: Doti; 52: Baitadi; 53: Bajhang].
![Figure 2: Ecological regions of Nepal and approximate geographic locations of news media-reported venomous snakebites and associated deaths [Locations of envenomed cases are shown in black circles and localities from where snakebite deaths were reported are indicated with red “pin” symbols. There are chances of overlaps of these symbols because several envenomings and deaths were reported from nearby localities]. The details of envenoming and associated deaths are mentioned in Table 1. The blue ellipses indicated districts where several areas were deluged often by over-flooding in monsoon.](/fulltextimages/11476/fig_2.png)
Figure 2: Ecological regions of Nepal and approximate geographic locations of news media-reported venomous snakebites and associated deaths [Locations of envenomed cases are shown in black circles and localities from where snakebite deaths were reported are indicated with red “pin” symbols. There are chances of overlaps of these symbols because several envenomings and deaths were reported from nearby localities]. The details of envenoming and associated deaths are mentioned in Table 1. The blue ellipses indicated districts where several areas were deluged often by over-flooding in monsoon.
Data Sources, Their Validation, and Ethical Approval
This article is an offshoot of analyzing case reports with substantial information reported in news media [14]. Snakebite incidence data were randomly and retrospectively searched and extracted from news reports of snakebites that occurred in Nepal over 13 years between January 2010 and December 2022 and published in international, national, and local newspapers. Snakebites not registered in healthcare institutions were validated by news reporters and those registered in healthcare systems were validated by hospital authorities or healthcare personnel involved in snakebites. The data searching methods are mentioned in a recently published article [14] and the ethical approval was not sought because we analyzed publicly available news reports.
Inclusion and Exclusion Criteria
We included news media reporting Nepalese snakebite incidences if articles contained incidences as well as case reports or case reports only. Then, we counted envenomings, deaths, nonvenomous snakebites, uncategorized snakebites that occurred in defined dates and places (i.e., geographic locations (addresses) where snakebite occurred) or those incidence data were directly cited either from certain healthcare facilities or Nepal Police Offices (NPOs). Although
we included case reports for the counts of incidence of envenomings and deaths, we excluded demographics, circumstances, pre-hospital care, and outcomes from those case reports. We included Nepalese snakebite cases referred to Indian healthcare systems to understand the burden of snakebite envenoming in Nepal. However, we excluded all media-reported snakebites that occurred out of Nepal. We excluded the incidence of snakebites, envenomings, and associated deaths without referring to either snakebite treatment centers (STCs), NPOs, or hospitals where antivenom supply was unclear and without geographic locations where snakebite occurred. We did not include journal articles describing snakebites, personal websites and blogs, and social media describing snakebites without original webpage links of the news media.
Data Collection and Management
Herein, we used unpublished data of snakebite incidence that were collected during the recently published study Pandey DP, et al. [14]. The data collection and their management are described in the published article [14]. Data Analysis We analyzed incidence of snakebites and associated envenomings and deaths by augmenting the respective numbers of cases mentioned in news articles reporting incidences only, both incidences and case reports, and case reports only (Figure 3). We measured total incidences of snakebites, envenomings, and associated deaths, including non-venomous and uncategorized snakebites (Figure 3).
![Figure 3: Flow diagram showing numbers of included and excluded news media articles, snakebite incidences, and outcomes of envenomated cases [STCs: Snakebite Treatment Centers, Hs: hospitals where antivenom supply was unclear but snakebite cases accessed, NPOs: Nepal Police Offices].](/fulltextimages/11476/fig_3.png)
We grouped the reported incidences into incidences known with localities where snakebites occurred, incidences extracted from STCs, and incidences based on hospitals (where antivenom supply was unclear) and NPOs. We considered that reporters correctly assigned envenomed cases by consulting with experienced medical personnel. If patients received antivenom or developed neurotoxicity or hemotoxicity, we grouped them into venomous snakebites. After 20 September 2015, Nawalparasi District was divided into Nawalpur and Parasi Districts following the state’s reconstruction of administrative divisions. The cases reported with locality data as “Nawalparasi” represented either district. Therefore, we grouped it as “Nawalparasi (either Nawalpur or Parasi District).”During data extraction, we did not extrapolate incidence data given for a particular year from the particular healthcare facilities into additional years for the same center. Next, news media might not cover all snakebites from Nepal.
The continuous data (e.g., elevations of localities where snakebites, snakebite envenomings, and snakebite deaths occurred) were not normally distributed. We used box plots and the Grubbs test to identify any outliers in the dataset and histogram and the Shapiro-Wilk test to examine the normality of continuous data distribution. We mentioned medians, interquartile ranges (IQRs), and ranges for the non-normally distributed continuous data where as we analyzed categorical data as proportions with percentages. We measured 95% confidence interval (CI) of all non-normal data using Wilcoxon test involving median. The statistical tests were performed at a 5% significance level. The most comprehensive datasets available are the Nepal Government’s annual reports [22, 23]. We used the Wilcoxon rank sum test to compare the incidence of snakebites known from news media during the last 13 years and Nepal Government’s snakebite data collected during the corresponding time frame. The variables “total annual envenomings” and “total annual deaths” were used to determine whether our data provided comparable or representative samples of all snakebites in Nepal. By evaluating the corresponding line graphs, we determined the existence of annual variations in snakebite envenomings and deaths in Nepal. Further, we calculated the size of the vulnerable population at risk of snakebite envenomings and associated deaths by the summation of the total human populations in districts where envenomated and/or dead cases were reported in news outlets. Further, we determined the association of “district-wise envenomings” with the human population density of respective districts using Spearman’s rank correlation (rho). The aforementioned total annual envenomings and deaths, district wise envenomings, and population density of the respective districts were not normally distributed. Hence, we used non- parametric inferential statistics. We measured outcomes in terms of the number and percentage of envenomed cases who died. We defined the absence of values for the aforementioned variables in news articles included in this study (the list of news articles and corresponding web links are available in S1 Table of the recently published article [14] as “Not available” or “NA”. While calculating inferential statistics and developing figures, we excluded these missing values adopting complete case analysis [24]. We performed all statistical analyses with the R statistical program (R version 4.1.2 (2021-11-01), The R Foundation for Statistical Computing Platform).
Results
A total of 43,482 snakebites were reported in 296 news articles published by 107 news media (Figure 3) during 2010 to 2022. This incidence was reported from across the terai, the hills, and the mountains (Figures 1 & 2) representing 53 districts, 36 STCs, eight hospitals (where antivenom supply was unclear), and four NPOs and across the altitudinal ranges from 62–2870 m asl [median: 174, CI: 178–214, IQR: 110–273 (Figure 4)] covering all provinces, all former development regions, including rural municipalities (i.e., rural areas) and municipalities (i.e., towns, cities, and suburb areas ).
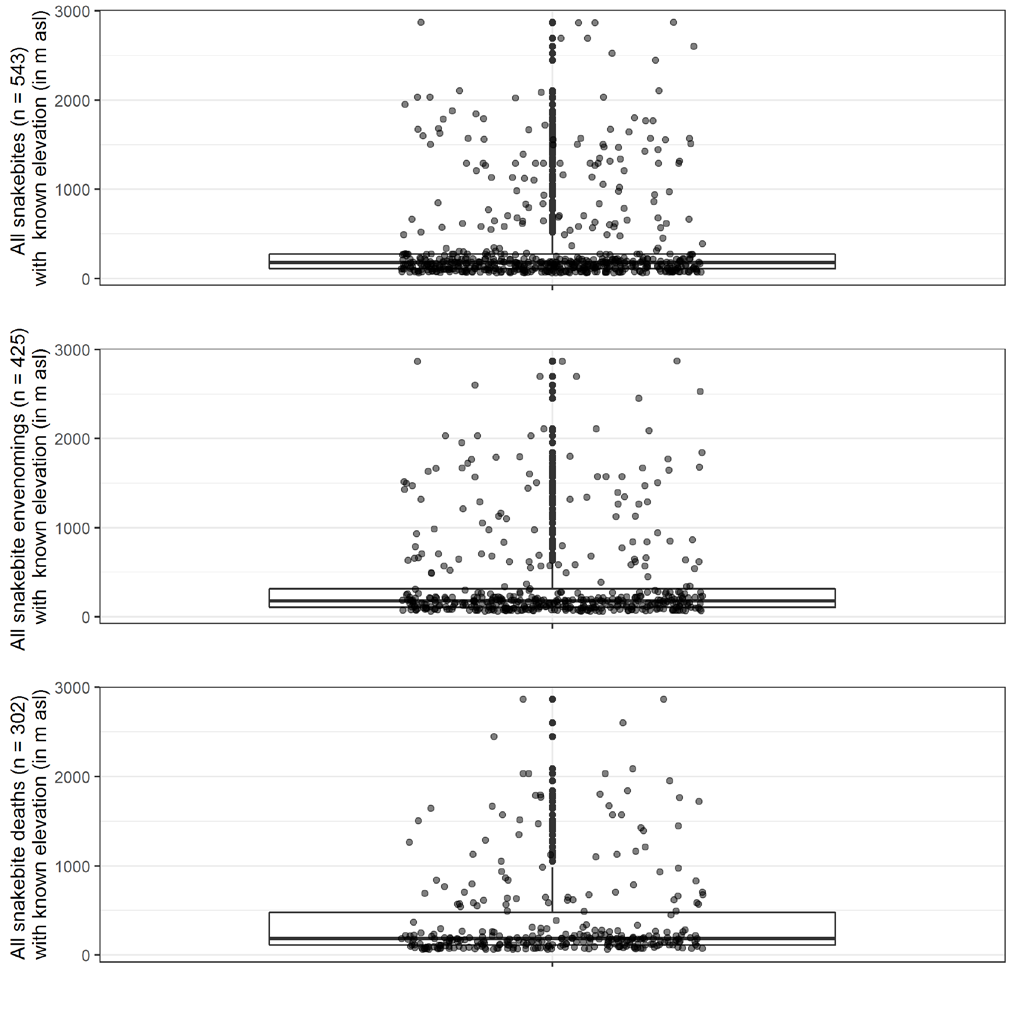
Only 11% (n = 4,593) of the total snakebites were envenomed (Figure 3). The majority of these envenomings occurred in Nepal’s lowlands (Figure 2). These envenomed cases represented 50 districts, 27 STCs, three hospitals (where the supply of antivenom was unclear), and four NPOs. These envenomings occurred across the altitudinal ranges from 62–2870 m asl [median: 179, CI: 185–245, IQR: 107–312 (Figures 3 & 4), with the highest incidence of envenomings in Jhapa (n = 225), followed by Dang (n = 63), Kanchanpur (n = 62), Saptari and Mahottari (n = 39 each), Taplejung and Rautahat (n = 23 each), Banke (n = 20), Sindhuli (n = 15), Baitadi (n = 13), Kailali, Morang, and Udayapur (n = 12 each) (Table 1).
| Incidence of envenomings reported from | |||||||
|---|---|---|---|---|---|---|---|
| Categories [DC: District codes; PC: province codes] | 50 districts (representing terai, hills, and mountains) in this study | 23 districts of terai region in other’s study† | |||||
| DC | PC | a. Districts* | Enveno mings | Snake bite deaths | Year ranges (within which cases were reported) | Snake bites n=166) | Deaths (n = 13) |
| 1 | I | Jhapa (994090; 619) | 225 | 24 | 2013, 2015–16, 2018– 19, 2021–22 | 9 | 1 |
| 38 | V | Dang (676277; 229) | 63 | 59 | 2015, 2017, 2018–22 | 6 | 1 |
| 49 | VII | Kanchanpur (517645; 322) | 62 | 57 | 2010–17, 2020–22 | 3 | 0 |
| 12 | II | Mahottari (715040; 714) | 39 | 28 | 2015–18, 2020–22 | 12 | 1 |
| 9 | II | Saptari (713203; 523) | 39 | 22 | 2012, 2015, 2017–22 | 28 | 1 |
| 8 | I | Taplejung (120359; 33) | 23 | 20 | 2012, 2015, 2018–21 | – | – |
| 14 | II | Rautahat (825623; 733) | 23 | 11 | 2014–19, 2021 | 0 | 0 |
| 39 | V | Banke (603393; 258) | 20 | 2 | 2016–18, 2020 | 6 | 0 |
| 17 | III | Sindhuli (300117; 120) | 15 | 2 | 2014, 2018–19, 2021, 2022 | – | – |
| 52 | VII | Baitadi (244400; 161) | 13 | 12 | 2019–22 | – | – |
| 2 | I | Morang (1147186; 618) | 12 | 8 | 2015, 2017–19, 2021– 22 | 5 | 0 |
| 5 | I | Udayapur (342773; 166) | 12 | 12 | 2010, 2013, 2016, 2018–20 | 2 | 0 |
| 48 | VII | Kailali (911155; 282) | 12 | 7 | 2010, 2013–14, 2018– 20, 2022 | 6 | 0 |
| 15 | II | Bara (743975; 825) | 8 | 6 | 2010, 2013–14, 2016, 2020–21 | 0 | 0 |
| 40 | V | Bardiya (460831; 228) | 8 | 5 | 2012, 2015–16, 2018, 2020, 2022 | 3 | 0 |
| 44 | VI | Salyan (238668; 163) | 7 | 7 | 2017, 2022 | – | – |
| 10 | II | Siraha (748416; 630) | 6 | 6 | 2017–18, 2020, 2022 | 8 | 1 |
| 42 | V | Pyuthan (231848; 177) | 6 | 6 | 2018, 2020 | – | – |
| 4 | I | Ilam (280565; 165) | 5 | 5 | 2011, 2017, 2019 | – | – |
| 16 | II | Parsa (649397; 480) | 5 | 4 | 2015, 2020 | 1 | 0 |
| 13 | II | Sarlahi (857360; 681) | 5 | 5 | 2015, 2019, 2022 | 26 | 4 |
| 19 | III | Chitwan (722168; 326) | 5 | 3 | 2014, 2018, 2020 | 3 | 1 |
| 28 | IV | Nawalpur (aka Nawalparasi East; 381105; 267) | 5 | 5 | 2016, 2021 | – | – |
| 37 | V | Kapilvastu (686739; 395) | 5 | 5 | 2020 | 12 | 1 |
| 35 | V | Parasi (aka Nawalparasi West; 385515; 525) | 5 | 3 | 2015, 2021–22 | – | – |
| 36 | V | Rupandehi (1118975; 823) | 5 | 5 | 2014–15, 2020, 2022 | 12 | 0 |
| 51 | VII | Doti (205683; 102) | 5 | 5 | 2015, 2019–20 | – | – |
| 3 | I | Sunsari (934461; 743) | 4 | 4 | 2015, 2019–20 | 6 | 0 |
| 45 | VI | Surkhet (417776; 170) | 4 | 3 | 2018, 2020, 2022 | 3 | 0 |
| 50 | VII | Achham (229816; 137) | 4 | 4 | 2017–18, 2021–22 | – | – |
| 20 | III | Dhadhing (322751; 168) | 3 | 1 | 2016, 2022 | – | – |
| 47 | VI | Humla (55496; 10) | 3 | 3 | 2018–19 | – | – |
| 22 | III | Bhaktapur (430408; 3617) | 2 | – | 2015 | – | – |
| 31 | IV | Kaski (599504; 297) | 2 | – | 2020–21 | – | – |
| 41 | V | Palpa (242423; 177) | 2 | 2 | 2014, 2018 | – | – |
| 46 | VI | Dailekh (253319; 169) | 2 | 2 | 2017 | – | – |
| 53 | VII | Bajhang (189097; 55) | 2 | 2 | 2012, 2019 | – | – |
| 6 | I | Panchthar (174419; 141) | 1 | – | 2017 | – | – |
| 11 | II | Dhanusha (873274; 740) | 1 | 1 | 2020 | 7 | 0 |
| 24 | III | Dolakha (172726; 79) | 1 | – | 2022 | – | – |
| 21 | III | Kathmandu (2017532; 5108) | 1 | 1 | 2016 | – | – |
| 18 | III | Makawanpur (461053; 190) | 1 | – | 2022 | 7 | 1 |
| 27 | III | Rasuwa (45554; 30) | 1 | 1 | 2015 | – | – |
| 25 | III | Sindhupalchowk (262852; 103) | 1 | – | 2016 | – | – |
| 34 | IV | Baglung (250554; 140) | 1 | 1 | 2019 | – | – |
| 29 | IV | Gorkha (252201; 70) | 1 | – | 2019 | – | – |
| 30 | IV | Lamjung (153480; 91) | 1 | 1 | 2014 | – | – |
| 33 | IV | Parbat (132703; 269) | 1 | 1 | 2020 | – | – |
| 32 | IV | Syangja (254965; 219) | 1 | 1 | 2022 | – | – |
| 43 | V | Rolpa (236226; 126) | 1 | 1 | 2022 | – | – |
| Subtotal A | 679 | 363 | – | – | |||
| b. Undefined areas (UA) | |||||||
| Terai areas | 5 | 4 | 2012, 2019 | – | – | ||
| Nawalparasi (either Nawalpur or Parasi District) | 1 | 1 | 2022 | 8 | 1 | ||
| Subtotal B | 6 | 5 | – | – | |||
| SN | c. Snakebite Treatment Centers where antivenom was supplied during the report of snakebites by news media reporters | ||||||
| 1 | V | Rupandehi District’s Bhairahawa based Bhim Hospital | 1155 | – | 2017 | – | – |
| 2 | V | Banke District’s Nepalgunj based Bheri Zonal Hospital (aka Bheri Hospital) | 906 | 65 | 2014, 2015–18, 2020, 2022 | – | – |
| 3 | V | Rupandehi District’s Butwal based Lumbini Zonal Hospital Data | 505 | 80 | 2011, 2013, 2016–17 | – | – |
| 4 | III | Chitwan District’s Bharatpur based Bharatpur Hospital Data | 362 | 33 | 2014, 2017, 2020, 2021 | – | – |
| 5 | I | Sunsari District’s Itahari based Community STC Data | 191 | – | 2017–18 | – | – |
| 6 | VII | Kailali District’s Dhangadi based Seti Zonal Hospital (now aka Seti Provincial Hospital) Data | 162 | 36 | 2014, 2016–18, 2022 | – | – |
| 7 | I | Jhapa District’s Damak based STC (run by Nepal Red Cross Society) Data | 130 | – | 2018 | – | – |
| 8 | VII | Kanchanpur District’s Bheemdatta Municipality, Mahendranagar based Mahakali Zonal Hospital (aka Mahakali Hospital) Data | 110 | 2 | 2016–17, 2020–21 | – | – |
| 9 | II | Mahottari District’s Bardibas-03, Gauridanda based STC Data | 72 | 4 | 2014–17, 2019–22 | – | – |
| 10 | II | Sarlahi District’s Nawalpur based STC Data | 52 | 2 | 2021–22 | – | – |
| 11 | II | Siraha District’s Choharwa based Jayakali STC | 52 | – | 2017–18 | – | – |
| 12 | I | Morang District’s, Biratnagar based Koshi Zonal Hospital Data | 50 | 3 | 2012 | – | – |
| 13 | II | Rautahat District Hospital, Gaur Data | 19 | 13 | 2014–17 | – | – |
| 14 | II | Sarlahi District’s Malangawa based Sarlahi District Hospital Data | 11 | 11 | 2019 | – | – |
| 15 | II | Saptari District’s Khadak Municipality-07, Kalyanpur based STC (run by Nepl Army) Data | 10 | – | 2019 | – | – |
| 16 | V | Bardiya District’s Thakurbaba Municipality, Sainbar based STC (run by Nepal Army) | 10 | 10 | 2017 | – | – |
| 17 | II | Saptari District’s Rajbiraj based Gajendra Narayan Singh Sagarmatha Zonal Hospital Data | 9 | 2 | 2019 | – | – |
| 18 | III | Shukraraj Tropical and Infectious Disease Hosptal, Teku (aka Teku Hospital) Data | 7 | – | 2019 | – | – |
| 19 | I | Jhapa District’s Kehankawal Rural Municipality, Baniyani-based STC Data | 6 | – | 2021 | – | – |
| 20 | II | Bara District Hospital, Kalaiya (aka Kalaiya Hospital) Data | 6 | 6 | 2010 | – | – |
| 21 | I | Jhapa District’s Kankaimai Municipality-04, Kotihom based Kankai Sahara STC Data | 5 | – | 2019 | – | – |
| 22 | II | Mahottari District’s Jaleshwor based Jaleshwor Hospital Data | 4 | 1 | 2013 | – | – |
| 23 | III | Parsa District’s Birgunj based Narayeni Hospital Data | 4 | 4 | 2020 | – | – |
| 24 | III | Sindhuli District’s Dudhauli Municipality-09, Dudhauli based STC Data | 4 | 1 | 2016–17 | – | – |
| 25 | V | Bardiya District’s Gulariya based Bardiya District Hospital Data | 3 | 1 | 2018 | – | – |
| 26 | V | Kapilvastu District’s Buddhabhumi-02, Garusinghe based STC Data | 2 | 2 | 2020 | – | – |
| 27 | I | Udayapur District’s Katari Municipality based STC Data | 1 | 1 | 2018 | – | – |
| Subtotal C | 3848 | 277 | – | – | |||
| SN | d. Known from hospitals where snakebite cases accessed (availability of antivenom to these healthcare systems was unknown) | ||||||
| 1 | VII | Baitadi District Hospital Data | 7 | – | 2019 | – | – |
| 2 | III | Rasuwa District Hospital Data | 2 | – | 2016 | – | – |
| 3 | VII | Darchula District Hospital Data | 1 | – | 2018 | – | – |
| Subtotal D | 10 | – | – | – | |||
| SN | e. Nepal Police Offices | ||||||
| 1 | VII | Sudurpaschim Pradesh Police Office, Dipayal Data | 43 | 43 | 2018 | – | – |
| 2 | I | Udayapur District’s Area Police Office Data | 4 | 4 | 2018 | – | – |
| 3 | I | Jhapa District Police Office Data | 2 | 2 | 2022 | – | – |
| 4 | VI | Salyan District Police Office Data | 1 | 1 | 2022 | – | – |
| Subtotal E | 50 | 50 | – | – | |||
| Grand total (subtotal A+B+C+D+E) | 4593 | 695 | |||||
| Abbreviations and symbols: aka: also known as; SN: serial number; STCs: Snakebite Treatment Centers; *the numerals in the parenthesis represents respective district’s human population and population density, respectively, as mentioned in Nepal Population Census 2021; total Nepal population = 29192480; total population of 50 districts = 24785096, i.e., 85% of national population; †Snakebite epidemiology in humans and domestic animals across the terai region in Nepal: a multicluster random survey. Lancet Global Health, 10 (3): e398-e408. |
Table 1: Distribution of news media reported incidences of snakebite envenomings and associated deaths during 2010–2022 by distri
Among the reported envenomed cases, 695 snakebite deaths represented 43 districts, 19 STCs, and four NPOs. These envenomings occurred across the altitudinal ranges from 62–2866 m asl [median: 182, CI: 190–325, IQR: 110– 479 (Figures 3 & 4, Table 1), with the highest incidence of deaths reported from Dang (n = 59), followed by Kanchanpur (n = 57), Mahottari (n = 28), Jhapa (n = 24), Saptari (n = 22), Taplejung (n = 20), Baitadi and Udayapur (n = 12 each), and Rautahat (n = 11) (Table 1). The overall case fatality rate (CFR) was 15%.
| News media-reported incidence of snakebites | Incidence of snakebites reported in Nepal Government’s national reports | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Years | Venomous snake bites | Nonve nomous snake bites | UCS | Total snake bites | AER | Snake bite deaths | CFR | Fiscal years | Venomous snakebites | Nonve nomous snake bites | Total snake bites | AER | Snake bite deaths | CFR | Refere nces no |
| 2010 | 24 | – | 500 | 524 | 4.6 | 24 | 100 | 2009-10 | 1319 | 15844 | 17163 | 7.7 | 131 | 9.9 | 2 |
| 2011 | 26 | – | 150 | 176 | 14.8 | 26 | 100 | 2010-11 | 1083 | 17121 | 18204 | 5.9 | 118 | 10.9 | 2 |
| 2012 | 65 | 79 | – | 144 | 45.1 | 16 | 24.6 | 2011-12 | 979 | 13789 | 14768 | 6.6 | 89 | 9.1 | 2 |
| 2013 | 220 | 857 | 1994 | 3071 | 7.2 | 13 | 5.9 | 2012-13 | 867 | 13462 | 14329 | 6.1 | 79 | 9.1 | 2 |
| 2014 | 317 | 559 | 1281 | 2157 | 14.7 | 65 | 20.5 | 2013-14 | 998 | 4145 | 5143 | 19.4 | 10 | 1 | 1, 2 |
| 2015 | 215 | 264 | 1416 | 1895 | 11.3 | 32 | 14.9 | 2014-15 | 667 | 3461 | 4128 | 16.2 | 1 | 0.1 | 1 |
| 2016 | 356 | 363 | 2366 | 3085 | 11.5 | 54 | 15.2 | 2015-16 | 663 | 2605 | 3268 | 20.3 | 20 | 3 | 1 |
| 2017 | 2113 | 927 | 7299 | 10339 | 20.4 | 101 | 4.8 | 2016-17 | 912 | 5209 | 6121 | 14.9 | 33 | 3.6 | 1 |
| 2018 | 364 | 1561 | 6504 | 8429 | 4.3 | 139 | 38.2 | 2017-18 | 794 | 4,812 | 5606 | 14.2 | 20 | 2.5 | 1 |
| 2019 | 156 | 366 | 3736 | 4258 | 3.7 | 92 | 58.8 | 2018-19 | 696 | 3871 | 4567 | 15.2 | NA | NA | 1 |
| 2020 | 250 | 60 | 3815 | 4125 | 6.1 | 58 | 23.2 | 2019-20 | 878 | 4203 | 5081 | 17.3 | NA | NA | 1 |
| 2021 | 327 | 902 | 2338 | 3567 | 9.2 | 25 | 7.6 | 2020-21 | 967 | 6935 | 7902 | 12.2 | NA | NA | 1 |
| 2022 | 160 | 90 | 1462 | 1712 | 9.3 | 50 | 31.3 | Total | 10823 | 95457 | 106280 | 10.2 | 501 | 4.6 | |
| Total | 4593 | 6028 | 32861 | 43482 | 10.6 | 695 | 15.1 | Pandey (2015) | 1172 | – | 22053 | – | 121 | 10.3 | 3 |
| Abbreviations and symbol: AER: annual envenoming rate (%); CFR: case fatality rate; UCS: uncategorised snakebites; “–”: not available or not mentioned. 1. Department of Health Services. Annual report 2077/78 (2020/2021); p.198–99. In: Department of Health Services, editor. Kathmandu: Annual Report published by Government of Nepal, Ministry of Health and Population, Department of Health Services. Available at: https://dohs.gov.np/annual-report-fy-2077-78-2019-20/; FY 2020/21. p. i–xxxv+512. 2. Department of Health Services. Annual Report 2070/71 (2013/2014); p. 108. In: Department of Health Services, editor. Kathmandu: Annual Report published by Government of Nepal, Ministry of Health and Population, Department of Health Services. Available at: https://dohs.gov.np/wp-content/uploads/2014/04/Annual_Report_2070_71.pdf; FY 2013/14. p. 425. 3. Pandey DP (2015). Venomous snakes of medical relevance in Nepal: study on species, epidemiology of snake bite and assessment of risk factors of envenoming and death. Frankfurt: Ph.D. dissertation published by J. W. Goethe University; Available at: http://publikationen.ub.uni-frankfurt.de/frontdoor/index/index/docId/38272. |
Table 2: The annual incidence of snakebites and associated envenomings and deaths reported by the news media during 2010– 2022 an
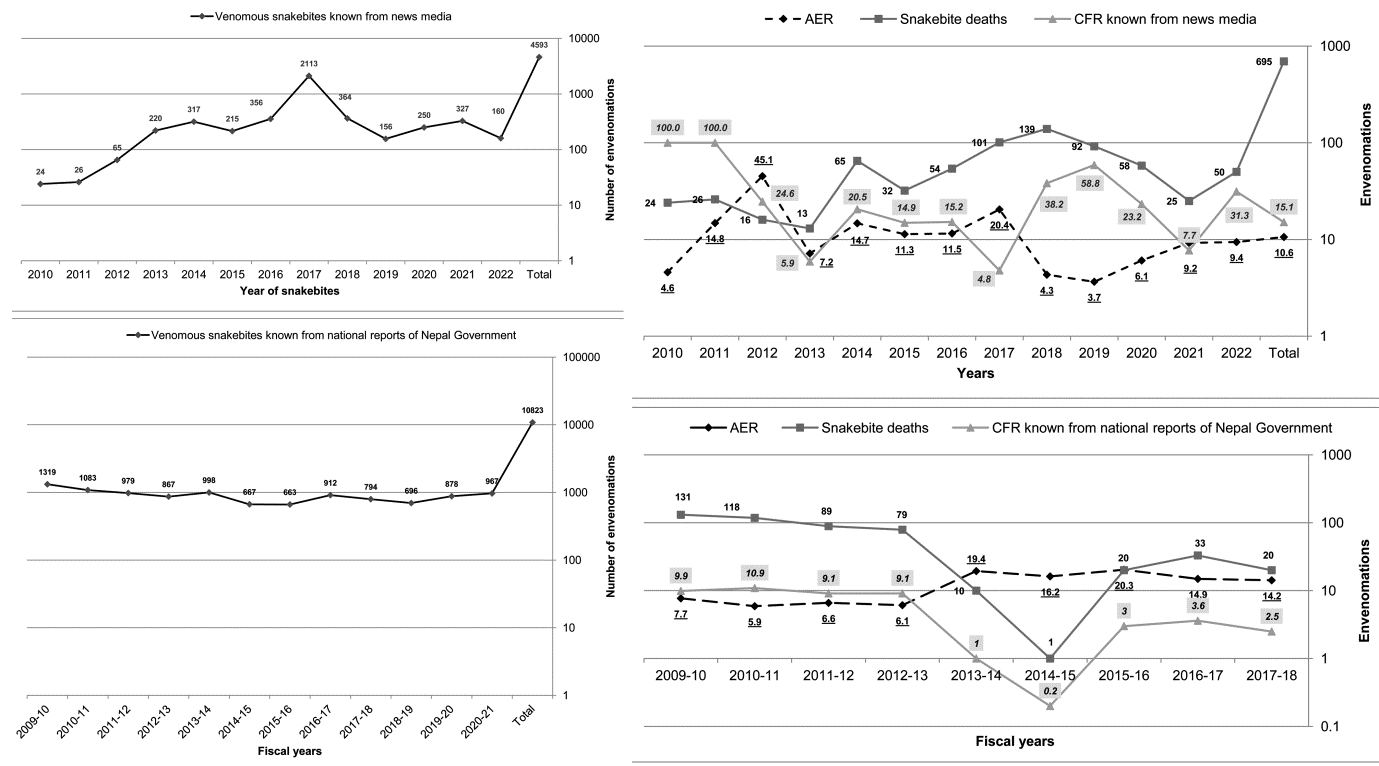
We conjectured that at least 10,339 snakebites cause 2,113 envenomings and 101 deaths annually in Nepal (Table 2). The news media and Nepal Government sources did not differ regarding annual envenoming rates (AER, p-value = 0.287) and annual incidences of snakebite deaths (AISD, p-value = 0.926). However, they did differ in case fatality rate (CFR, p-value = 0.001) and annual incidence of envenomings (AIE, p-value = <0.0001, Table 2). Further, line graphs Figure 5 showed distinct yearly variations in incidences of snakebite envenomings and deaths in Nepal. Next, snakebite envenomings were weakly positively associated with human population density in Nepal (rho = 0.304, p-value = 0.032).
Discussion
This comprehensive epidemiological study of Nepalese snakebite envenomings mentioned in news media provided a representative/comparable sample of all envenomings in Nepal (p-values for: AER = 0.287; AISD = 0.926). However, we found slightly greater annual CFR and AIE than the corresponding CFR and AIE reported by Nepal Government (Table 2). This could occur due to the high priority of journalists to expose envenomed and dead cases known from healthcare institutions as well as communities to the public. The government’s national database was based on hospitals where medical record systems were poor [9] or inadequate [25]. This epidemiological study is the most comprehensive because it illustrated incidences of Nepalese snakebite envenomings known for 13 years in the terai, hills, and mountains, representing all provinces, 50 districts and 27 STCs and highlighted deaths representing 43 districts and 19 STCs (Table 1, Figures 2 & 3). Next comprehensive study of 308 news media reported case reports with substantial information of envenomings also found similar influence of venomous snakebites in the terai, hills, and mountains, representing all provinces and 48 districts [14]. By analyzing the 308 envenomated case reports, Pandey and Thapa found snakebite fatalities from 43 districts [14] similar to this comprehensive analysis of snakebite incidence obtained from similar sources (Figure 3). But, other studies described the situations of snakebite envenomings and associated deaths from a maximum of 23 districts [7] or 15 district hospitals [6]. The altitudinal distribution of snakebite envenoming in our study was comparable to those reported in study of 308 news media reported envenomed case reports representing 48 districts of Nepal [14]. Although terai extending in between 60 m and 200 m asl (Figures 1, 2 & 4) is at the highest risk of envenoming and associated deaths, the districts located in the hills and mountains are also affected from snakebite-related fatalities perceptibly (Figures 1 & 2, Tables 1). In addition to the 23 districts of the terai region of Nepal [7] people inhabiting 20 other districts [Taplejung (n = 20 deaths), Baitadi (n = 12), Salyan (n = 7), Pyuthan (n = 6), Doti (n = 5), Achham (n = 4), Ilam (n = 4), Humla (n = 3), Bajhang, Dailekh, Palpa, and Sindhuli (2 deaths in each districts), Baglung, Dhadhing, Kathmandu, Lamjung, Parbat, Rasuwa, Rolpa, and Syangja (1 each)] were also affected by snakebite deaths (n = 77) frequently. Unlike the findings of seven snakebites and one death from Makawanpur District from November 2017 to April 2019 in a community survey [7], we found only one envenomed case. However, scores of envenomings and deaths in the top five districts Table 1 correspond to the report of incidence from the respective districts identified by Alcoba et al. [7]. However, around 85% of the national population is noticeably vulnerable to snakebite envenomings and at risk of snakebite deaths in aforementioned 50 districts of Nepal (Table 1). Therefore, the incidence rate reported by Alcoba et al. [7] from 23 districts along the lowlands of Nepal (where nearly half of the national population inhabits) cannot be generalized nationwide.
Since incidences of snakebite envenomings known from 50 districts Table 1 were positively associated with human population density in Nepal, the findings obtained by excluding urban areas having more than 20,000 people in the randomized cluster survey of snakebites in 23 districts located along the terai region [7] might not even represent those particular districts of Nepal. Such a biased study design might cause their findings of the lower influence of snakebite envenoming in the districts located in western terai compared to the eastern terai of Nepal [7]. On the contrary, we found the highest incidence of case fatalities from the Dang and Kanchanpur Districts located in western terai (Table 1).
The distribution of snakebite envenoming and associated deaths in the terai Figure 2 corresponds to the snakebite risk map published by Epidemiology and Disease Control Division, Nepal Government (EDCD) [26]. However, several hilly districts Figure 2 were not included in that snakebite risk map recommended by Nepal Government [22, 26] and previous studies were mainly based in terai region of Nepal. Our findings disclosed increased incidences of snakebite envenomings in the hills and mountains of Nepal. However, further study is needed to know whether this increase in snakebite envenoming in the hills and in some parts of mountains are associated with the impact of global warming and climate change. [27].
The snakebite envenomings and associated fatalities in the subtropical and temperate regions (Figures 1 & 2) suggest transcending of venomous snakes from tropical regions, probably due to the increment of road transport in the Chure and Mahabharat ranges of Nepal (Figure 1). Snakes could be transferred along with goods carried in trucks. Further, global warming might support their flourishing in those regions [27]. The incidences of envenomings also depend on the human population density and abundance of venomous snake species. Our findings of weak association of snakebite envenomings and human population density (rho = 0.304, p-value = 0.032) may not guarantee that more risks of envenomings in more densely populated areas. It is because the information of envenomings due to venomous snakebite might not be quickly disseminated in rural and urban areas where human population density is varied. Next, snakebite envenomings may be reported with the same accuracy in more densely populated areas as in more sparsely populated areas and with worse medical infrastructures. Therefore, more sophisticated research is needed to know the impact of human population density, transport, and effects of climate changes on envenomings in Nepal’s subtropical and temperate regions.
Although the incidence vary depending on the species of snake involved in envenoming [28], most of the envenomings occurred in tropical areas than in subtropical and temperate regions (Figures 1 & 2). Unlike the findings in a cross-sectional survey in villages of 23 districts of the terai region of Nepal [7], such envenomings occurred mainly in far- and mid-western Nepal [12]. Although the recall bias in community-based surveys might cause this variation, our findings correspond to the distribution and diversity of nocturnal medically relevant snake species distributed in Nepal [11, 12, 29, 30]. The geographical locations of reported deaths (Figure 2) signify the snakebite hotspots in tropical to temperate regions of Nepal. The case fatality rate (CFR) is noticeably higher than that is reported in a cross-sectional survey carried in rural areas of 23 districts across the lowlands in Nepal [7]. In Shukraraj Tropical and Infectious Disease Hospital, Teku, Kathmandu, more snakebite cases visited the hospital seeking snakebite treatment for the fiscal year 2014 (n = 420) than in 2013 (n = 248). Next, the Lumbini Zonal Hospital, Butwal, also experienced increased snakebite deaths in 2017 compared to 2016’s case fatality. These periodic increments were supported by the corresponding reports of snakebite incidence for 2013 and 2014 and 2016 and 2017, respectively (Table 2, Figure 5). The maximum incidence of snakebite envenoming during 2017 (Table 2, Figure 5) might be associated with the effects of over-flooding because the increased incidence of snakebites during flooding was reported elsewhere [31, 32, 33, 34]. Among the envenomed case reports mentioned in two news articles, there were instances of one snakebite envenoming and four deaths in areas deluged with a flood in 2017: one death in Siraha District’s Sakhuwanrkatti Rural Municipality, three deaths of envenomed patients from Saptari District’s Hanumannagar Kankalini Municipality (n=2) and Krishna Sabaran Rural Municipality (n=1); one envenomed case from Saptari’s Tilathi Koiladi Rural Municipality was referred to BPKIHS where the patient was under treatment, meantime. In the monsoon of 2017, from the flood-affected areas of Saptari, 36 snake-bitten people (uncategorized) were admitted to Gajendra Narayan Singh Sagarmatha Hospital in Rajbiraj within two weeks after the flooding.
Similarly, from the flood-affected Biratnagar of Morang District, 25 uncategorized snakebite patients were admitted daily to Koshi Hospital in Biratnagar. Within two weeks of the same year’s monsoonal flood-affected areas of Banke District in western Nepal, 15 envenomed cases and 27 uncategorized cases were admitted in Nepalgunj-based Bheri Hospital. In addition to the flood-affected districts, other districts having inundated areas during heavy monsoonal rainfall are indicated by blue ellipses (Figure 2). Saptari and Mahottari in the eastern Nepal and Dang and Kanchanpur districts in the western Nepal were affected by flooding, which might cause many envenomings in these districts (Figure 2, Table 1). Overall, the rainfall and flooding patterns might cause fluctuations in the annual incidences of snakebite envenomings and associated deaths in the lowlands and other regions of Nepal. However, a longitudinal, prospective study of envenomings and deaths is necessary to confirm regional or nationwide supra-annual variation of snakebite envenoming in Nepal.
In Nepal, a minimum of 10,339 snakebites occur annually resulting in 2,113 envenomings and 101 deaths (Table 2). We considered the highest snakebite incidences and associated consequences for a particular year in our incidence dataset to be the estimation of minimum incidence for this country. Our estimate of a minimum annual incidence of snakebite is, however, greater than the annual total snakebites reported by Department of Health Services (DOHS) during the fiscal years 2013 to 2021 (Table 2). Similarly, our estimation of annual CFRs is also greater than corresponding reports of DOHS during the fiscal years 2013 to 2018 (Table 2). But, the estimated AER is comparable with the reports of DHOS during the fiscal years 2015 to 2016 (Table 2). We inferred that our minimum estimation of annual incidence of snakebites and associated consequences can be increased because of several factors influencing on the snakebite incidence and its recording. Firstly, there were no mentions of dry bites at all in our data records, which indicated that news reporters might include dry bites either in category of nonvenomous snakebites or uncategorized snakebites (Figure 3). The incidences of nonvenomous snakebites may represent nonvenomous as well as dry bites. Next, 76% of snakebite incidences were uncategorized (Figure 3). This might include venomous, nonvenomous, and dry bites. Therefore, the annual incidence of snakebites and associated consequences in Nepal can be greater than our aforementioned estimates of snakebite burdens. The huge number of uncategorized snakebite incidences Figure 3 suggests the need of empowering journalists to define envenomed, non-envenomed, and dry bites consulting with related authorities and experts. Improved reporting of this neglected tropical issue can be analyzed in future by prospective researchers for more precise estimation of snakebite burden in Nepal and understanding the trend of envenomings annually and by different level of localities. There is potential of increasing annual snakebite burdens in Nepal if news reporters are empowered to define available snakebite information as envenomed, non-envenomed, and dry bites while reporting in news articles. Overall, our findings are important for policy makers in Nepal and other countries where the geo-climates and patterns of snakebite incidences and associated consequences are analogous.
Limitations
We estimated the maximum snakebite incidences and associated consequences Table 2 to be the minimum incidences because news media might not cover all snake bitten and envenomed cases and our eligible incidence related data could represent only a subset of all snakebites, envenomings, and associated deaths from Nepal. Several snakebites that occurred in the remote areas might not be reported in the news media. Likewise, the search keys and engines that we used retrospectively might cause missing of the news reporting of incidence of snakebites, envenomings, and deaths. Therefore, snakebite incidences can be increased by searching news media data prospectively using additional search strategies. Further, there was possible that our estimations of incidences could be influenced if journalists reported these incidences without consulting with authorities in healthcare systems or the patients or other eyewitnesses.
Conclusions
People inhabiting or working in 50 districts of Nepal are vulnerable to snakebites and associated consequences. Snakebite envenomings mostly affected tropical areas of this country, particularly in Lumbini and Sudurpaschim provinces and Dang and Kanchanpur Districts. Compared to the past records, case fatality rate has been decreased in Nepal. However, incidences of envenomings and fatalities in the hills and mountains are challenges for snakebite management in Nepal. Therefore, the snakebite risk map recommended by Nepal Government should be immediately updated for the effective and efficient snakebite management nationwide. This improvement supports medical authorities in antivenom distribution and estimating healthcare personnel requirements and their appropriate deployment in the snakebite affected areas. The patterns of heavy rain and flooding might influence on supra-annual variations of snakebite envenomings and deaths. However, additional research is needed to confirm association of supra-annual variations with rainfall and flooding patterns. Moreover, our findings can also be used to design and conduct more effective and knowledge-based educational interventions in high snakebite prone flood affected provinces and districts to reduce snakebite mortality substantially. Empowerment of journalists is essential to improve prospective snakebite reporting in news. Subsequently, the improved case reports in news supports to carry out more sophisticated research cost-effectively in Nepal and elsewhere having similar impact of snakebites.
Acknowledgments
We would like to thank Gita Subedi Pandey and Narayan
B. Thapa for their support to search and find news media- reported snakebites and data management. Further, we are grateful to anonymous reviewers for their comments.
Author Contributions
Study design and concept (DPP); data analysis (DPP); initial drafting of the manuscript (DPP, BC); multiple revisions of the manuscript (DPP, BC, AD, RKB); critical revisions of the manuscript (DPP); final approval of manuscript (DPP). All authors approved the final manuscript. DPP is guarantor of the paper.
Funding
None
Conflicts of Interests
None
Data availability
The data that support the findings of this study are available upon request from the corresponding author, DPP.
References
-
Chippaux JP (2017) Snakebite envenomation turns again into a neglected tropical disease. J Venom Anim Toxins Incl Trop Dis 23(1): 38.
-
Kasturiratne A, Wickremasinghe AR, de Silva N, Gunawardena NK, Pathmeswaran A, Premaratna R, et al. (2008) The global burden of snakebite: a literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS Med 5(11): 1591-1604.
-
Chippaux JP (1998) Snakebites: appraisal of the global situation. Bull World Health Organ 76(5): 515-524.
-
Gutiérrez JM, Calvete JJ, Habib AG, Harrison RA, Williams DJ, et al. (2017) Snakebite envenoming. Nat Rev Dis Primers 3(1): 17063.
-
Roberts NLS, Johnson EK, Zeng SM, Hamilton EB, Abdoli A, et al. (2022) Global mortality of snakebite envenoming between 1990 and 2019. Nat Commun 13(1): 6160.
-
World Health Organization (1987) Zoonotic disease control: baseline epidemiological study on snakebite treatment and management. Wkly Epidemiol Rec 62(42): 319-320.
-
Alcoba G, Sharma SK, Bolon I, Ochoa C, Martins SB, et al. (2022) Snakebite epidemiology in humans and domestic animals across the terai region in Nepal: a multicluster random survey. Lancet Global Health 10(3): 398-408.
-
Pandey DP (2007) Epidemiology of snakebites based on field survey in Chitwan and Nawalparasi Districts, Nepal. J Med Toxicol 3(4): 164-168.
-
Magar CT, Devkota K, Gupta R, Shrestha RK, Pandey DP, et al. (2013) A hospital based epidemiological study of snakebite in Western Development Region, Nepal. Toxicon 69: 98-102.
-
Basnyat B, Shilpakar O (2022) Snakebite envenoming: a hidden health crisis. Lancet Global Health 10(3): 311- 312.
-
Pandey DP (2015) Venomous snakes of medical relevance in Nepal: study on species, epidemiology of snake bite and assessment of risk factors of envenoming and death. pp: 231.
-
Pandey DP, Shrestha BR, Acharya KP, Shah KJ, Thapa- Magar C (2023) A prospective study of snakebite in a tertiary care hospital in south-western Nepal. Trans R Soc Trop Med Hyg 117(6): 435-443.
-
Pandey DP, Sharma SK, Alirol E, Sharma CM, Thapa-Magar C, et al. (2018) Eco-epidemiological circumstances, pre- admission histories and assessment of risk factors of envenoming and death due to krait and Russell’s Viper bites in Southern Nepal.
-
Pandey DP, Thapa NB (2023) Analysis of news media- reported snakebite envenoming in Nepal during 2010– 2022. PLoS Negl Trop Dis 17(8): e0011572.
-
Acharya BB (2018) An overview of Nepali news media: Challenges and prospects. Journal of University Grants Commission 7(1): 75-92.
-
Bara LR (1975) The press in Nepal (1951-74). Contributions to Nepalese Studies 2(1): 169-186.
-
Onta P (2001) The print media in Nepal since 1990: Impressive growth and institutional challenges. Studies in Nepali History and Society 6(2): 331-346.
-
Wasko DK, Bullard SG (2016) An analysis of media- reported venomous snakebites in the United States, 2011–2013. Wilderness Environ Med 27(2): 219-226.
-
Chunara R, Andrews JR, Brownstein JS (2012) Social and news media enable estimation of epidemiological patterns early in the 2010 Haitian cholera outbreak. Am J Trop Med Hyg 86(1): 39-45.
-
Sharma SK, Chappuis F, Jha N, Bovier PA, Loutan L, et al. (2004) Impact of snakebites and determinants of fatal outcomes in southeastern Nepal. Am J Trop Med Hyg 71(2): 234-238.
-
Pandey DP, Vohra R, Stalcup P, Shrestha BR (2016) A season of snakebite envenomation: presentation patterns, timing of care, anti-venom use, and case fatality rates from a hospital of southcentral Nepal. J Venom Res 7: 1-9.
-
Annual Report (2021/2022) Goverment of Nepal, Ministry of Health and Population, Department of Health Services Kathmandu.
-
Annual Report (2013/2014) Goverment of Nepal, Ministry of Health and Population, Department of Health Services Teku, Kathmandu.
-
Heymans MW, Twisk JWR (2022) Handling missing data in clinical research. J Clin Epidemiol 151: 185-188.
-
Pandey DP (2018) Retrospective study of snakebites in Nawalpur snakebite treatment center, south-central Nepal. Semantic scholar.
-
Bista MB, Banerjee MK, Thakur GD, Shrestha JM, Upadhyay PK, et al. (2005) Incidence of poisonous snakebite in Nepal. Kathmandu: Department of Health Services, Epidemiology and Disease Control Division, Ministry of Health, Government of Nepal.
-
Martin G, Yanez-Arenas C, Rangel-Camacho R, Murray KA, Goldstein E, et al. (2021) Implications of global environmental change for the burden of snakebite. Toxicon: X 9-10: 100069.
-
De Silva A (1981) Snake bites in Anuradhapura District. The Snake 13(2): 117-130.
-
Pandey DP, Bhattarai P, Piya RC (2020) Food spectrum of Common Kraits (_Bungarus caeruleus_): An implication for snakebite prevention and snake conservation. J Herpetol 54(1): 87-96.
-
Sharma SK, Kuch U, Höde P, Bruhse L, Pandey DP, et al. (2016) Use of molecular diagnostic tools for the identification of species responsible for snakebite in Nepal: a pilot study. PLoS Negl Trop Dis 10(4): e0004620.
-
Ochoa C, Bolon I, Durso AM, Ruiz de Castañeda R, Alcoba G (2020) Assessing the increase of snakebite incidence in relationship to flooding events. J Environ Public Health 6135149: 1-9.
-
Kathmandu 2077/78 (2020/2021) In: Department of Health Services. Annual Report published by Government of Nepal, Ministry of Health and Population. pp:198-99.
-
Kathmandu 2070/71 (2013/2014) In: Department of Health Services. Annual Report published by Government of Nepal, Ministry of Health and Population. pp: 108.
-
Pandey DP (2015) Venomous snakes of medical relevance in Nepal: study on species, epidemiology of snake bite and assessment of risk factors of envenoming and death.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells