Unraveling the Significance of Etiology in Allergic Rhinitis: Leveraging Artificial Intelligence (AI) to Analyze Clinical Profiles for Suitable Interventions in South Indian Patients
Background: Allergic rhinitis (AR) is a prevalent global disorder affecting millions across the world among all age groups. This study delves into the etiology of AR, unravelling the natural progression of the disease from its inception and identifying causative factors. The primary aim of this investigation was to explore the etiology of allergic rhinitis, paving the way for informed decisions regarding prevention, treatment, or cure. Methods: Using Artificial Intelligence (AI) to delineate the clinical profiles of patients suffering from allergic rhinitis, including symptom severity, duration, and associated comorbidities were assessed in the fifteen case studies. Other parameters were studied by regular standard laboratory procedures as described in the text. Results: A total of 15 patients with age-wise distribution showed females were 60 % (9) and males 40 % (6). A total of 11 cases (73.33%) had IgE values between 20–100 IU/mL and 26.66 % (4) had IgE values above 100 IU/mL. In all other cases, IgE levels were less than 20 IU/mL and therefore were not considered important. Other data such as nasal congestion, rhinorrhea, sneezing, and nasal itching, were highlighted, alongside other associated manifestations and are presented in tables and graphs. Conclusions: It is concluded that in these 15 cases with complaints of AR, a correlation between the levels of IgE and age distribution, gender distribution, and eosinophil counts was observed. These factors were also found to correlate with IgE levels, indicating the severity of the disease. By understanding how the disease initially manifests and its underlying causes, valuable insights were gained into predicting its future course using AI. Additionally, patient education and awareness were enhanced based on individual clinical profiles. With a steady increase in the application of AI models for healthcare, the day is not far when AI may become the essential feature of all medical care in the future.
Introduction
We are witnessing how health care is being revolutionized by Artificial Intelligence [1]. In the field of Allergic rhinitis (AR), few studies are available in Artificial Intelligence (AI) [2, 3]. AR commonly known as hay fever is an allergic inflammation of the nasal airways triggered by exposure to allergens such as pollen, dust mites, animal dander, and mold spores [4]. Allergic rhinitis was found to affect 20 to 30% of adults worldwide and perhaps a somewhat higher percentage (40%) of children and about 15 % develop asthma. Moreover, allergic rhinitis symptoms develop at the age of 20 years and peak at the age of 22-40 years before progressively decreasing after that. Clinically, it is characterized by four major symptoms–rhinorrhea, sneezing, nasal itching, and nasal congestion. It can also be associated with co-morbid conditions such as asthma, atopic dermatitis, and nasal polyps. The diagnosis and treatment of allergic rhinitis follow the ARIA (Allergic Rhinitis and its Impact on Asthma) guidelines while for asthma the GINA (Global Initiative for Asthma) guidelines [5].
Allergic rhinitis is divided into two forms the first form is intermittent and the second form is persistent as seasonal and perennial [6]. Based on severity, allergic rhinitis can be categorized into mild, moderate, and severe for management purposes. Occasionally the allergic rhinitis diagnosis is clinically based on the history and physical examination of patients. In most cases, environmental determinants, such as allergen exposure, air pollution, climate change, ozone, smoking, viral infection, and environmental toxicants, may underlie much of the increase in allergic rhinitis prevalence [7]. The classic symptoms of nasal congestion, nasal runny nose and ocular symptoms are directly related to the allergic process, interference with their symptoms leads to daytime sleepiness and impaired quality of life. Allergic rhinitis patients fail to carry out their regular activities because of discomfort and if the symptoms become more severe the problem is interference with work productivity, which has been the biggest contributor to the total economic cost of allergic rhinitis. It was found that among the atopic disorders, allergic rhinitis was the most prevalent [8].
The fundamental mechanism responsible for nasal symptoms varies depending on the kind of rhinitis and allergen sensitization or atopy is represented-IgE. Since humans are predisposed to produce IgE reactions to biochemically diverse substances found in their surrounding environment [9]. These molecules or allergens come from various sources such as dust, foods, molds, pollens and arthropods. Allergy-related rhinitis is limited to individuals with a genetic predisposition to allergies. Even while everyone is constantly exposed to allergens in the environment, only those who are predisposed to being hypersensitive suffer symptoms. In these sensitive individuals, repeated exposure to aeroallergens causes B cell activation and plasma cell maturation, which in turn produces specific IgE antibodies [10]. IgE attaches itself to certain receptors on the outside of basophils and mast cells. The release or production of chemical mediators by the cells causes allergy symptoms when the sensitizing allergen cross-links to the specific IgE that is attached to the cell [11]. Proof of sensitization to an allergen includes coupling of skin or blood testing and the patient’s exposure history [12].
In addition to the history and physical examination, specific allergy tests are performed to make the diagnosis, as the clinical characteristics may appear similar in other types of non-infective rhinitis. Among these diagnostics are skin prick testing for particular allergens [13, 14]. Although they are a little more expensive, allergen-specific IgE tests (RASTs/ ELISA) are thought to be as useful tests for diagnosing AR as they indicate atopy. On the other hand, eosinophilia and allergic respiratory disease are known to be associated with nasal smears for eosinophilia, and systemic eosinophilia is also regarded as a crucial investigative tool for the diagnosis of allergic rhinitis.
Moreover, elevated IgE (often referred to as high and very high serum IgE levels) is normally considered a serum signature for allergic/atopic conditions [15, 16]. In clinical practice, these patients are sent to allergy clinics if they have suspected allergic illnesses or other conditions characterized by increased IgE levels. For instance, atopic dermatitis and hyper-IgE syndrome are common among the disorders with higher blood serum IgE levels (typically IgE greater than 10,000 IU/mL), followed by asthma, parasitosis, and allergic rhinitis [16]. This study aimed to comprehend whether etiology and family history could be the major determinants of AR. The IgE is an antibody that plays a crucial role in the immune system’s response to allergens. IgE levels are closely associated with the development and manifestation of allergic rhinitis. Furthermore, we hypothesized that serum biomarkers (total IgE and serum eosinophil) could predict nasal eosinophilia to simplify our daily practice and reserve more time-consuming and expensive tests for some patients. Hence our objective was to determine the role of IgE in AR.
Material and Methods
Study Group and Ethical Approval
Subjects with a history of allergic rhinitis (AR) were selected by the ENT and Allergy Department at Mahavir Hospital and Research Centre, Hyderabad. The study group included 15 AR cases. Written informed consent was obtained from all participants after explaining the study objectives. The study design adhered to the principles of the Declaration of Helsinki and was approved by the hospital’s Ethics Committee. Inclusion criteria: This study included only those patients who were suffering from allergic rhinitis caused by aeroallergens. Only healthy individuals with no diseases were selected as control subjects. Exclusion criteria: This study excluded children, pregnant women, diabetics, and those who were suffering from some other allergies like food allergy and chronic asthma Demographic Information: A questionnaire was designed to collect the demographic information of all the patients and Data was collected. Etiological information: Etiological information of AR patients as described by Small P, et al. [17], as described in the Table 1 below was referred to as standard [17].
| Allergic Rhinitis | AETIOLOGY/ DESCRIPTION |
|---|---|
| IgE-mediated (allergic) | • IgE-mediated inflammation of the nasal mucosa, resulting in eosinophilic and Th2-cell infiltration of the nasal lining |
| • Further classified as intermittent or persistent | |
| Autonomic | • Vasomotor |
| • Drug-induced (rhinitis medicamentosa) | |
| • Hypothyroidism | |
| • Hormonal | |
| • Non-allergic rhinitis with eosinophilia syndrome (NARES) | |
| Infectious | • Precipitated by viral (most common), bacterial, or fungal infection |
| Idiopathic | • Aetiology cannot be determined |
Table 1: Etiological classification of Rhinitis.
Table 1: Etiological classification of Rhinitis.
Blood Collection and Immunoglobulin E (IgE) test
Venous blood samples were collected in serum separator tubes (BD Vacutainers) The blood samples were kept at room temperature for 20-30 minutes to allow proper clot formation, and then blood samples were centrifuged at 3600 rpm for 10 minutes (5430R, Eppendorf, Germany). The serum samples were separated and stored at 4Oc for further analysis.
Enzyme-Linked Immunosorbent Assay (ELISA)
The semiquantitative analysis of the serum IgE antibody detection test was performed by Enzyme-Linked Immunosorbent Assay (ELISA). The allergen-specific immunoglobulin E (IgE) test is a blood test that measures the levels of different IgE antibodies in the serum of a person’s blood. We used a sandwich-ELISA kit (Peprotech, USA) which is based on the specific binding between an allergen and its corresponding antibody and is therefore highly specific. The binding of an antibody to an allergen is detected by colorimetric analysis after the addition of substrate using a standard ELISA plate reader (Lambda Scientific, Australia). Ferastraoaru, et al. [18] classified serum total IgE levels into four categories: ultra-low, defined as less than 20 IU/mL; normal, defined as total IgE levels between 20 and 100 IU/ml; high, defined as total IgE levels between 100 and 1000 IU/ml; and very high, defined as total IgE levels between 1000IU/mL and above. Elevated IgE levels are associated with allergic conditions, including allergic rhinitis [18].
Absolute Eosinophil Count
Absolute Eosinophil Count (AEC) is measured as the number of Eosinophils per microliter (cells/μL) of blood. A normal absolute Eosinophil count is typically in the range of 30 to 350 cells/μL. Eosinophils are a type of white blood cell, and elevated Eosinophil counts were associated with allergic rhinitis. Standard lab procedure was used to measure AEC counts.
Results
In this study, we could identify the risk factors and define their impact on AR patients. Hay fever symptoms appear throughout the year, outdoor allergies are worse in the spring, summer, and early fall. In warm weather, weeds and flowers bloom and pollen counts are higher. Indoor allergies such as those that result from pet dander and dust mites, get worse in winter because people spend more time indoors. Environmental determinants, such as allergen exposure, air pollution, climate change, ozone, smoking, viral infection, and environmental toxicants, may underlie much of the increase in AR prevalence. In addition, specific epigenetic changes caused by environmental exposure may contribute to cellular homeostasis and the development of allergic diseases.
Symptoms of AR Include
- Nasal stuffiness (congestion), sneezing, and runny nose.
- Itchy nose, throat, and eyes.
- Headaches, sinus pain, and dark circles under the eyes.
- Increased mucus in the nose and throat.
- Fatigue and malaise (general feeling of discomfort).
- Sore throat from mucus dripping down the throat (postnasal drip).
- Wheezing, coughing, and trouble breathing.
- Hives
| Case | Age | Symptoms | IgE Levels (IU/µl) | AEC Levels (cells/mL) | Duration of AR Symptoms | Additional Findings |
|---|---|---|---|---|---|---|
| 1 | 23 | Frequent cold, heaviness in head (sinusitis), vague abdominal discomfort, allergic rhinitis | 2114 | 385 | Last 4-5 years | Positive skin prick test to many allergens |
| 4 | 23 | Sneezing, runny nose, allergic rhinitis | 350 | 128 | Last 6 months | Positive skin prick test to many allergens |
| 8 | 47 | Sneezing, runny nose, blocked nose | >400 | 130 | Since childhood | Positive skin prick test to many allergens |
| 10 | 35 | Sneezing, nasal discharge, wheezing | >400 | 327 | Last 3-4 years | Positive skin prick test to many allergens |
| 14 | 20 | Sneezing, nasal discharge, wheezing, nasal congestion | >400 | 315 | Since childhood | Positive skin prick test to many allergens |
| 15 | 14 | Sneezing, runny nose, blocked nose | 1511 | 172 | Since childhood | Positive skin prick test to many allergens |
Table 2: Male Cases: providing details of their symptoms, IgE levels, AEC levels, duration of AR symptoms.
| Case | Age | Symptoms | IgE Levels (IU/µl) | AEC Levels (cells/mL) | Duration of AR Symptoms | Additional Findings |
|---|---|---|---|---|---|---|
| 2 | 28 | Runny nose, sneezing, allergic rhinitis | 400 | 650 | Last 3 years | Positive skin prick test to many allergens |
| 3 | 22 | Deviated nasal septum, immediate type hypersensitivity, allergic rhinitis | 1056 | 350 | Last 5 years | Positive skin prick test to many allergens |
| 5 | 32 | Watery nasal discharge, excessive sneezing, maxillary polyp, mucosal colena | 1324 | 400 | Last 4 years | Positive skin prick test to many allergens |
| 6 | 20 | Recurrent urinary infection, watery discharge, sneezing, cough, adenoid hypertrophy | >400 | 162 | Since childhood | Immediate type hypersensitivity, allergic mucosa, deviated nasal septum, adenoid hypertrophy |
| 7 | 25 | Blocked nose, post-nasal drips | >400 | 162 | Since childhood | Allergic mucosa |
| 9 | 19 | Sneezing, nasal obstruction, adenoid hypertrophy | 320 | 219 | Since childhood | Bilateral inferior turbinate hypertrophy, granular throat, sphenoid sinusitis, spur, bilateral tympanic membrane intact |
| 11 | 26 | Nasal discharge, nasal congestion, headache | >400 | 176 | Last 4-5 years | Allergic mucosa, |
| 12 | 22 | Wheezing, internal irritation, nasal congestion, asthma | 1402 | 340 | Since childhood | Bilateral inferior turbinate hypertrophy |
| 13 | 40 | Sneezing, runny nose, wheezing, headache | 275 | 650 | Last 4-5 years | Granular throat |
Table 3: Female Cases: providing details of their symptoms, IgE levels, AEC levels, duration of AR symptoms.
These Tables 2 & 3 segregate the cases into male and female category, providing details of their symptoms, IgE levels, AEC levels, duration of AR symptoms, and additional findings.
Patient’s Age-Wise and Gender-Wise Distribution
In this study, a total of 15 patients with age-wise distribution showed females are 60 % (9) and males 40% (6) as shown in Figure 1a. Furthermore, age-wise distribution indicates that 26.66% of patient arebetween 14-20 years, followed by 46.66% in the 21-30 age group, 20% in the 31- 40 range, and 6.66%in the 41-50 category Figure 1b.
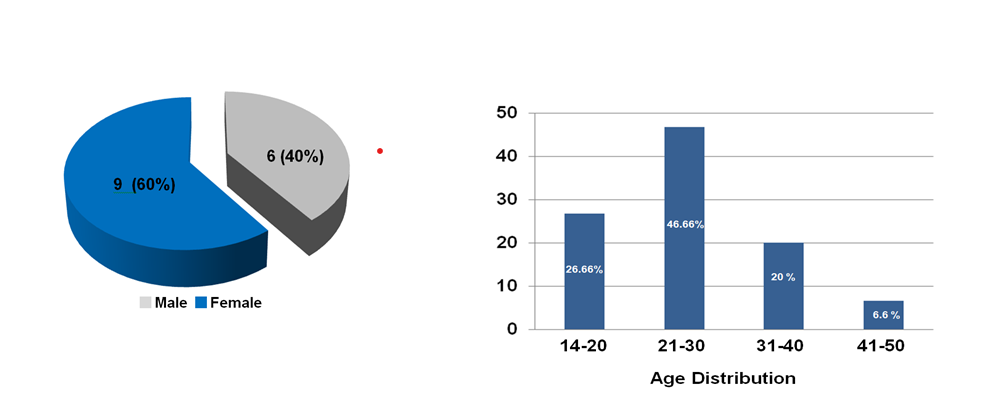
According to health experts, there was a substantial increase in AR incidence and mortality, the details of all the above parameters are presented in the form of graphs and tables.
A total of 11 cases (73.33%) had IgE values of 20–100 U/ml, and 4 cases (26.66 %) had IgE values above 100 U/ml Table 4.
| Age | Sex | Total IgE range 20- 100U/ml | Total IgE above 100- 1000U/ml | Total IgE above 1000- 2000U/ml | |
|---|---|---|---|---|---|
| Patients number | Min: 22 Max: 53 Mean: 33.2 | Male: 6 Female: 9 | 10 cases (66.66%) | 4 cases (26.66%) | 1 case (6.66%) |
Table 4: Showing the demographic structure and the distribution of the antibody.
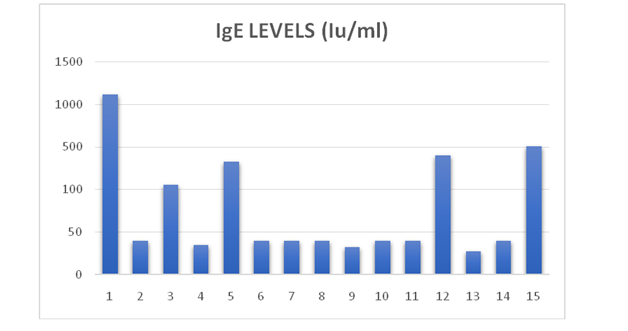
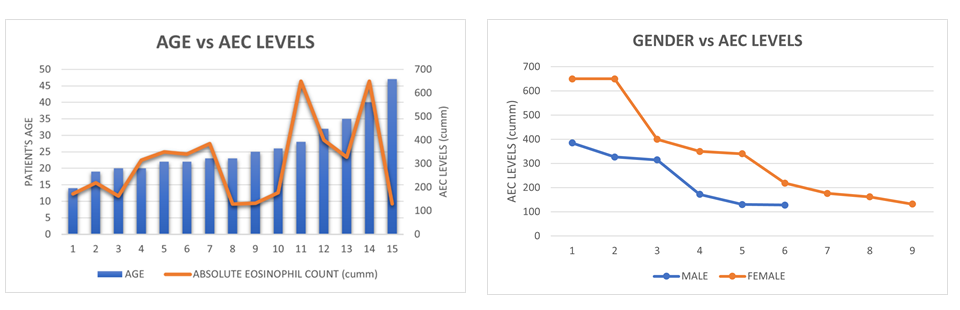
Results of the few important parameters such as IgE levels and AEC of the patients are presented below. In this study we found that all the cases had high levels of IgE Figure 2, which is a common symptom of Allergic rhinitis; these patients had been treated with a series of therapeutic drugs. In Figure 3a, the graph shows total IgE level decreases with age in patients with allergic rhinitis. Figure 3b shows Gender versus Ig levels: It appears from this study that females are more likely to suffer from allergic rhinitis than males.
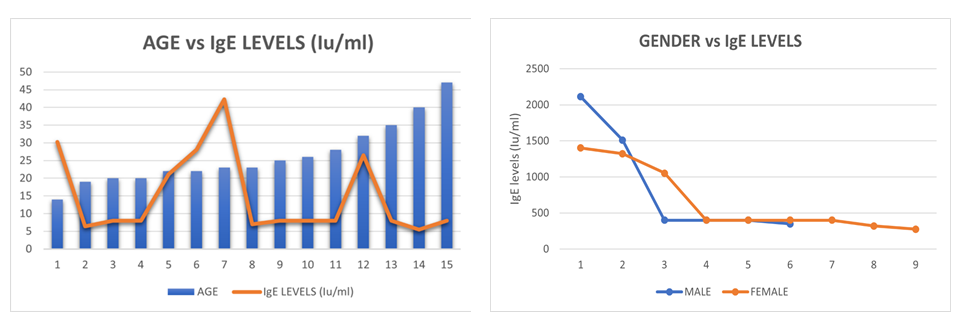
.
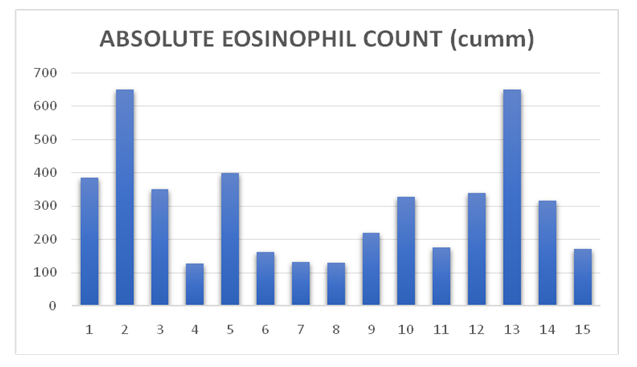
As seen in Figure 4 all the cases had high levels of AEC, which is a common symptom of Allergic Rhinitis, these patients had been treated with a series of therapeutic drugs. In Figure 5a it is seen that AEC increases with age. It reflects an increase or decrease to the exposure time of the individuals to the allergens. In Figure 5b, we have found that AEC among females and males shows a decreasing tendency in both sexes, it varies with the time of exposure to the allergens and is not due to an increase in age parameter.
Discussion
This study investigated the etiology of allergic rhinitis among South Indian patients and explored the clinical profiles associated with Allergic Rhinitis. The study could identify some of the prevalent parameters responsible for allergic rhinitis in these cases through clinical testing and patient history. Using Artificial Intelligence (AI) it was possible to delineate the clinical profiles of patients suffering from allergic rhinitis, including symptom severity, duration, and associated comorbidities [19]. Further, counselling to enhance patient education on disease awareness, based on individual clinical profiles was useful. By achieving these objectives, the study provided a comprehensive understanding of allergic rhinitis in the South Indian context and enhanced the effectiveness of its prevention and management through personalized treatment approaches.
Allergic Rhinitis like any other disease passes through various stages of initial susceptibility followed by pathological onset, this is the time when symptoms appear which require clinical interventions and then resolution [20]. Each stage of the illness may be modifiable by intervention, such as prevention, treatment, and rehabilitation, as well as by self- care and social adjustments. The crucial purpose of etiology is to identify the risk factors to cure the patients and prevent the occurrence of the disease by examining the biomarkers of the risk factors. It is now well recognized that all diseases are multifactorial, having various combinations of causative agents or risk factors that produce an effect of the health of the individual. Thus, the biomedical concept of disease has grown to include psychosocial elements critical to functional health. AI is still in stage of infancy and can never replace a doctor for patient diagnosis and treatment but the big question is how machine learning can be better than human intelligence for healthcare therapeutics. It is understood that AI is based on various inputs that acknowledge the information retrieved to imitate human knowledge into AI and this can help both medical specialists and patients in various ways [21].
Allergic rhinitis affects 20-30% of people across the globe and accounts for approximately 50% of allergies in India [22]. It has significant economic and health outcomes [23]. The present study revealed that the incidence of allergic rhinitis was much higher during the spring and winter seasons when there was pollen in the air. The mean age in this study was similar to the studies conducted by Jagadeeshwar, et al. [24] (33.1 years) and Tegnoor, et al. [25] (33.12 years). The patients were primarily young adults, which may have contributed to seasonal or demographic disparities in allergen exposure [24, 25]. Upon reviewing various literature studies, AI has also predicted that allergic rhinitis was more common in young adults and children, while it decreases in the elderly. This finding was concordant with studies similar to previous studies, there were more cases of females than males [26].
Interestingly, Serum IgE levels and Eosinophil Counts were consistent investigation tools for the diagnosis of Allergic Rhinitis [27]. Several laboratory tests confirm the diagnosis of allergic rhinitis based on medical history and physical examination which helps in determining the underlying cause of allergic rhinitis disease. Numerous researches have explored the link between allergies and clinical conditions. One study indicated that lgE levels in serum were elevated in 88% of patients [28]. Allergic Rhinitis has a well-established association with eosinophils. Demirjian et al. found increased serum IgE and eosinophil levels in patients with AR, indicating an atopic etiology [29]. In our study, we have seen that absolute eosinophil count (AEC) increases with age. Patel, et al. [30] found a substantial link with nasal smear eosinophilia, while Allergic Rhinitis shows no significant correlation with systemic eosinophilia30. Mostafa, et al. [31] found that Absolute Eosinophil Count was positive in 70.4% of Allergic Rhinitis patients, making it a reliable indication of the condition31. However, allergic rhinitis is a mechanism that contributes to disease occurrence and is usually more complex, the association between the atopic reaction and clinical phenotypes cannot be easily understood in clinical practice.
The study has some limitations, first, the sample size was very small, and secondly, a significant portion of the study participants were outdoor patients, however AI inputs had matching outputs. Although increased IgE levels and eosinophils counts were expected due to allergic reaction, it was not possible to further investigate due to limited resources. The facts presented here were amply supported by other studies and also by AI. The etiology factors significantly contribute to the development of allergic rhinitis, but it is important to determine the interaction between genes and environmental triggers which can ultimately determine an individual’s susceptibility to this allergic condition. Further research into these mechanisms underlying allergic rhinitis could pave the way for more personalized approaches to diagnosis, prevention, and treatment.
Conclusion
Allergic diseases are amongst the most prevalent diseases worldwide and the burden of these diseases continues to increases. The use of AI to answer clinical issues in allergic rhinitis has the potential to improve diagnostic accuracy, therapeutic approaches, and overall patient care. As the field of AI research grows fast, there are numerous opportunities to use AI to better understand and define allergic disease processes in order to provide personalized care. Furthermore, understanding the role of IgE and eosinophils count in allergic rhinitis is essential for developing the application of AI methods to targeted treatments and interventions to alleviate symptoms and improve the treatment strategies for individuals affected by this condition.
Declarations
Acknowledgements: we are grateful to the Chairman and Research Director of Bhagwan Mahavir Medical Research Centre for their encouragement and support. Ethical Approval and Consent to Participate: The Institutional Ethics Committee (IEC) which met on 23rd December 2022, approved this study. The informed consent process and the standards of the Ethics Committee were in accordance with the guidelines of the World Medical Association, Declaration of Helsinki 2008.
Competing Interests: The authors declare that they have no competing interests.
Funding: No funds were received for this study.
References
-
Alowais SA, Alghamdi SS, Alsuhebany N, Alqahtani T, Alshaya AI, et al. (2023) Revolutionizing healthcare: the role of artificial intelligence in clinical practice. BMC Medical Education 23: 689.
-
Jamil K, Uddin MA, Gade S (2023) Leveraging Artificial Intelligence for Targeted Response in Allergic Rhinitis. British Journal of Healthcare and Medical Research 10(3): 281-283.
-
Chen YH, Liao EC, Chen WL (2018) Applications of artificial intelligence in allergic rhinitis and asthma. Allergy, Asthma & Immunology Research 10(4): 370- 376.
-
Shyam G, Chandana R, Anusha Reddy GA, Asimuddin M, Jamil K (2022) Allergic Rhinitis and Atopy: The Causative Role of Aeroallergens: A Review. Acta Scientific Medical Sciences 66: 55-64.
-
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, et al. (2008) Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 63(86): 8-160.
-
Corsico AG, De Amici M, Ronzoni V, Giunta V, Mennitti MC, et al. (2017) Allergen-specific immunoglobulin E and allergic rhinitis severity. Allergy Rhinol (Providence) 8(1): 1-4.
-
Gerven LV, Alpizar YA, Steelant B, Callebaut I, Krohn IK, et al. (2017) Enhanced chemosensory sensitivity in idiopathic rhinitis patients and its reversal by nasal capsaicin treatment. J Allergy Clin Immunol 140(2): 437- 446.
-
Meltzer EO (2016) Allergic Rhinitis: Burden of Illness, Quality of Life, Comorbidities, and Control. Immunol Allergy Clin North Am 36(2): 235-248.
-
Caraballo L, Valenta R, Puerta L, Pomes A, Zakzuk J, et al. (2020) The allergenic activity and clinical impact of individual IgE-antibody binding molecules from indoor allergen sources. World Allergy Organ J 13(5): 100118.
-
Dullaers M, De Bruyne R, Ramadani F, Gould HJ, Gevaert P, et al. (2012) The who, where, and when of IgE in allergic airway disease. J Allergy Clin Immunol 129(3): 635-645.
-
Shade KT, Conroy ME, Anthony RM (2019) IgE Glycosylation in Health and Disease. Curr Top Microbiol Immunol 423: 77-93.
-
Long A, McFadden C, DeVine D, Chew P, Kupelnick B, et al. (2002) Management of Allergic and Nonallergic Rhinitis: Summary. AHRQ Evidence Report Summaries.
-
Bernstein IL, Li JT, Bernstein DI, Hamilton R, Spector SL, et al. (2008) Allergy diagnostic testing: an updated practice parameter. Ann Allergy Asthma Immunol 100(3): S1-148.
-
Carosso A, Bugiani M, Migliore E, Anto JM, DeMarco R (2007) Reference values of total serum IgE and their significance in the diagnosis of allergy in young European adults. Int Arch Allergy Immunol 142(3): 230-238.
-
Wittig HJ, Belloit J, De Fillippi I, Royal G (1980) Age- related serum immunoglobulin E levels in healthy subjects and in patients with allergic disease. J Allergy Clin Immunol 66(4): 305-313.
-
Van de Veen W, Kratz CE, McKenzie CI, Aui PM, Neumann J, et al. (2019) Impaired memory B-cell development and antibody maturation with a skewing toward IgE in patients with STAT3 hyper-IgE syndrome. Allergy 74(12): 2394- 2405.
-
Small P, Frenkiel S, Becker A, Boisvert P, Bouchard J, et al. (2007) The Canadian Rhinitis Working Group Rhinitis: a practical and comprehensive approach to assessment and therapy. J Otolaryngol 36.
-
Ferastraoaru D, Hudes G, Jerschow E, Jariwala S, Karagic M, et al. (2021) Eosinophilia in Asthma Patients Is Protective Against Severe COVID-19 Illness. J Allergy Clin Immunol Pract 9(3): 1152-1162.e3.
-
Aamir A, Iqbal A, Jawed F, Ashfaque F, Hafsa H, et al. (2024) Exploring the current and prospective role of artificial intelligence in disease diagnosis. Ann Med Surg (Lond) 86(2): 943-949.
-
Wang J, Zhou Y, Zhang H, Hu L, Liu J, et al. (2023) Pathogenesis of allergic diseases and implications for therapeutic interventions. Sig Transduct Target Ther 8(1): 138.
-
Rahat K, Avlokita S, Pratyush S, Richa T (2021) Role of Artificial Intelligence in Diagnosis and Treatment of Various Medical Diseases in Patients. AMEI’s Curr Trends Diagn Treat 5(2): 92-98.
-
Chandrika D (2017) Allergic rhinitis in India- an overview. Int J Otorhinolaryngol Head Neck Surg 3(1): 1-6.
-
Srivastava T, Shamanna K, Viswanatha B (2018) Role of IgE and Absolute Eosinophil Count as Prognostic Markers to Determine the Optimum Duration of Therapy in the Management of Seasonal Allergic Rhinitis. Research in Otolaryngology 7(2): 36-42.
-
Jagadeeshwar K, Venumadhav V, Sangram V, Chowdary S, Rani S, et al. (2012) A study on serum IgE levels, peripheral eosinophils and individual symptoms in patients with noninfective rhinitis and asthma and related conditions. Int J Pharm Pharm Sci 4(1): 88-92.
-
Tegnoor MS, Jabri OBA, Kumar MV, Kurle V (2017) Assessment of serum IgE levels in patients of allergic rhinitis. Al Ameen J Med Sci 10(2): 136-140.
-
Fröhlich M, Pinart M, Keller T, Reich A, Cabieses B, et al. (2017) Is there a sex-shift in prevalence of allergic rhinitis and comorbid asthma from childhood to adulthood? A meta-analysis. Clin Transl Allergy 7: 44.
-
Sharma M, Khaitan T, Raman S, Jain R, Kabiraj A (2019) Determination of Serum IgE and Eosinophils as a Diagnostic Indicator in Allergic Rhinitis. Indian J Otolaryngol Head Neck Surg 71(Suppl 3): 1957-1961.
-
Han D, Lai X, Gjesing B, Zhong N, Zhang L, et al. (2011) The specific IgE reactivity pattern of weed pollen-induced allergic rhinitis patients. Acta Otolaryngol 131(5): 533- 538.
-
Demirjian M, Rumbyrt JS, Gowda VC, Klaustermeyer WB (2012) Serum IgE and Eosinophil count in allergic rhinitis-Analysis using a modified Bayes’ theorem. Allergol Immunopathol (Madr) 40(5): 281-287.
-
Patel AK, Nagpal TP (2014) Comparison of blood absolute eosinophil count and nasal smear eosinophils with symptoms and severity of clinical score in patients of allergic rhinitis. Indian Journal of Allergy, Asthma and Immunology 28(2): 74.
-
Mostafa HS, Qotb M, Hussein MA (2019) Allergic rhinitis diagnosis: skin-prick test versus laboratory diagnostic methods. Egypt J Otolaryngol 35: 262-268.
- Pattern of Gonadal Hormones in Oral Testosterone-Supplimented Male Wistar Rats with Diabetes-Induced Hypogonadism
- Re-Evaluation of the Genotoxicity of Currently Used Food Dyes in Mouse Multiple Organs Via Continuous Administration by Drinking Using the Comet Assay
- Pharmacogenetics of Type 2 Diabetes Mellitus: Linking Genetic Variability to Drug Efficacy and its Cardiovascular Outcomes
- Exploratory Proteomic Profiling of SARS-CoV-2 Infected THP-1 Macrophages Reveals Alterations in Inflammatory Response and Cellular Metabolism
- Study of Genotoxicity of Hepatocarcinogens in Multiple Organs in Mice by Feeding and Drinking Using the Comet Assay
- Spirulina Polypeptides Inhibit the Growth of Human Lung Tumor (H460) Cells