Assessment of Oral Bioavailability of Vitamin D3 and Its Metabolite, 25-hydroxy (OH) Vitamin D3 in Male Sprague Dawley Rats Following a Single Oral Dose of Biofield Energy Treated Vitamin D3
The present study was performed to determine the effects of The Trivedi Effect®-Energy of Consciousness Healing Treatment on vitamin D3 and rats through the pharmacokinetic parameters measurement of both plasma level of vitamin D3 and 25-hydroxy (OH)-vitamin D3 after the oral administration of vitamin D3 in rats. The test item, vitamin D3 was divided into two parts. One part was denoted as the control (without Biofield Energy Healing Treatment), while the other part was defined as the Biofield Energy Treated sample, which received the Biofield Energy Healing Treatment by renowned Biofield Energy Healer, Mahendra Kumar Trivedi. Additionally, one group of animals also received Consciousness Energy Healing Treatment per se by the Healer under similar conditions. Vitamin D3 oral formulations were administrated by oral gavage at a dose of 500 μg per kg in groups viz. G1 (untreated Vitamin D3), G2 (Biofield Energy Treated Vitamin D3) and G3 (Biofield Energy Treated animals received untreated Vitamin D3) group. The results showed that the relative oral exposure (AUC0–t) of vitamin D3 was significantly increased by 155.62% and 111.73% in G2 and G3 groups, respectively as compared to the control group. Biofield Energy Treatment also significantly improved the plasma peak concentration (Cmax) of vitamin D3 by 223.84% and 187.5% in G2 and G3 groups, respectively as compared to the control group. This study results also showed that the relative oral exposure (AUC0–t) of 25-hydroxy (OH)-vitamin D3 (metabolite) was significantly increased by 161.28% and 113.96% in G2 and G3 groups, respectively as compared to the control group (G1). Biofield Energy Treatment also significantly improved the plasma peak concentration (Cmax) of 25-hydroxy (OH)-vitamin D3 by 174.25% and 117.77% in G2 and G3 groups, respectively as compared to the control group. After oral administration, plasma concentrations of active metabolite, 25-hydroxy (OH)-vitamin D3 in all three groups were declined slowly. The mean residence time (MRTlast) and elimination rate constant (Kel) for this metabolite were unaltered in all three groups. These data suggest that Biofield Energy Treated vitamin D3 might be influenced in vivo biological activity of vitamin D3 due to increased plasma exposure (AUC) of both vitamin D3 and metabolite level, 25-hydroxy (OH)-vitamin D3 in rats. There was significant improvement (>100%) of relative oral bioavailability of both vitamin D3 and 25-hydroxy (OH)-vitamin D3 that might be due to the alteration of physicochemical properties and thermal properties of vitamin D3 by the Biofield Energy Treatment. Biofield Energy Healing Treatment could be an innovative strategy that opens new avenues to overcome poorly absorbed pharmaceuticals/nutraceuticals/herbal extracts and can also improve the therapeutic performance of orally active molecules.
Introduction
Vitamin D is a secosteroid and is related to the other steroid hormones, such as estrogen, progesterone and testosterone [1]. In the epidermis, endogenous 7-dehydrocholesterol is converted to pre-vitamin D when UVB breaks (290-310 nm) the β-ring of the cholesterol structure. Vitamin D is formed through thermal rearrangement of the pre-vitamin. The maximal concentration of pre-vitamin D in the skin is reached with a few hours of sun exposure, after which pre-vitamin D is reversibly converted into two inactive vitamin D compounds, lumisterol or tachysterol. This provides a natural limit on the amount of vitamin D produced [2]. There are several forms of vitamin D, but the two that are most biologically relevant are cholecalciferol (vitamin D3) and ergocalciferol (vitamin D2). Physiologically, they are recognized by the same enzymes and receptors; and overall, their metabolism is very similar [1]. Cholecalciferol is synthesized in the epidermis and can be obtained from a limited number of animal food sources in the diet such as salmon, cod liver oil, and egg yolks. Ergocalciferol is primarily obtained from mushrooms that are irradiated to convert naturally occurring ergosterol to ergocalciferol [3]. Both forms can be found in supplements and fortified foods, although the introduction of cholecalciferol fortification is more prominent than ergocalciferol. The prevalence of vitamin D deficiency and insufficiency is increasing in the US population. The overall prevalence of vitamin D deficiency and insufficiency are 29% and 68%, respectively [4]. It is apparent that vitamin D nutriture is an important aspect of health and disease in the US today. Hypertension, myocardial infarction, and stroke, as well as other cardiovascular related diseases, such as diabetes, congestive heart failure, peripheral vascular disease, atherosclerosis, and endothelial dysfunction have been associated with vitamin D deficiency and insufficiency [5, 6]. Vitamin D3 maintains and helps to absorb the calcium and phosphorus level that results in balanced skeletal metabolism and calcium homeostasis [7, 8]. It also plays an important role in maintaining the immunity, cardiovascular, and reproductive systems [9, 10]. Several health disparities have been associated with increased risk for vitamin D insufficiency. These include diabetes, cardiovascular disease, hypertension, pregnancy complications, and cancer [7, 8, 9]. Vitamin D insufficiency is among the risk factors for these health outcomes, and it is postulated that restoring vitamin D status may ameliorate some of the disparities [10]. The vitamin D intake of the US population does not meet the estimated average requirement (EAR) recommendations for vitamin D intake. In the US, 68% of adults and 70% children do not meet recommendations. More than half of the oral vitamin D intake for the US population is met by supplements and more than 1/3 is from fortified foods [11].
There are several reports which suggest that most of people Worldwide who are either deficient in (serum concentrations below 20 ng/ml ≈ 50 nmol/L) or have insufficient (20-30 ng/ml ≈ 50-75 nmol/L) vitamin D3 [12, 13, 14], a problem which can be addressed by fortifying foods with vitamin D3 and calcium. The mechanism of transformation of vitamin D and absorption kinetics of active form, vitamin D3 are very complicated to be concluded. Various factors are available that directly affect the vitamin D3 bioavailability such as dietary fiber, genetic factors, and effect of vitamin D3 status [15]. Surprisingly, there is little information available about the concentration of 25-hydroxyvitamin D3 in the blood, which is the best indicator of vitamin D3 status after its oral absorption. However, the biological activity of vitamin D3 is mediated via the formation of active metabolite, 1-α, 25-dihydroxyvitamin D3. There are several factors which affect its absorption and first-pass metabolism that lead to have very low plasma concentrations of both the metabolites (25-hydroxyvitamin D3 and 1-α, 25-dihydroxyvitamin D3) following an oral administration. Therefore, it is required to know how vitamin D3 metabolism modifies the active forms of vitamin D3 that circulate in the blood. Therefore, the current study was undertaken to assess the effects of the Biofield Energy Treatment on vitamin D3 bioavailability in rats.
Complementary and Alternate Medicine (CAM) methods have been reported with many clinical beneficial effects in energy healing therapies. Immune system function was significantly improved after Biofield Energy Treatment in case of cervical cancer patients [16], massage therapy [17], etc. Biofield Energy therapy has been discovered thousands year back, which were practiced worldwide such as improved quality of life in case of cancer patient [18], improved functional ability in case of arthritis patient [19], decreased pain and anxiety [20]. National Center for Complementary/ Alternative Medicine (NCCAM) has recommended with significant clinical outcome in various clinical pathogenic conditions [21, 22]. Biofield is generated from internal human processes such as blood flow, lymph flow, brain functions, and heart function. This energy can be harnessed and can transmit it into living organism and non-living materials by the process of Biofield Energy Healing. The Trivedi Effect®- Energy of Consciousness Healing Treatment had been extensively studied in the field of medical science [23, 24], microbiology [25, 26, 27, 28], genetics and biotechnology [29, 30], nutraceuticals [31, 32], agricultural science and livestock [33, 34, 35, 36], and materials science [37, 38, 39]. Recently, it has been reported that the Trivedi Effect® has significant capability to alter the physio-chemical and thermal properties of various pharmaceuticals, nutraceuticals, and organic compounds through possible intervention of neutrinos [40, 41, 42]. The Trivedi Effect®-Consciousness Energy Healing Treatment would be a useful approach for the enhancement of the bioavailability of pharmaceuticals and nutraceuticals. Thus, the aim of this study was to evaluate the effect of Biofield Energy Healing Treatment on the plasma pharmacokinetics of vitamin D3 and 25-hydroxy (OH)-vitamin D3 in rats after a single oral dose of vitamin D3.
Materials and Methods
Chemicals and Reagents
Vitamin D3, 25-hydroxyvitamin D3 and telmisartan were purchased from Sigma (St. Louis, MO, USA). The reagents used for sample preparation and bioanalysis included acetonitrile (HPLC Grade, Merck), methanol (HPLC Grade, Merck), water (Milli-Q), and formic acid (LC-MS Grade, Fluka). USP grade nitrogen was used as the curtain gas and collision gas for LC-MS/MS were supplied from air compressor (Anesta Iwata, Japan), polypropylene tubes (Tarsons, India), class-A, measuring cylinders and volumetric flasks (Borosil, Germany) and membrane filters, 0.22 μm and 0.45 µm (Millipore) were used during the study. All other reagents and solvents were of analytical grade available from India.
Energy of Consciousness Treatment Strategies
The test item, vitamin D3 was divided into two groups; one part was considered as the control sample, while other part of test item was known as the Biofield Energy Treated test sample. The treated test item group was subjected to the Trivedi Effect®-Energy of Consciousness Healing by Biofield Energy Healer (also known as the Trivedi Effect®). The Biofield Energy Treatment (Blessing) was provided by a renowned Biofield Energy Healer, Mr. Mahendra kumar Trivedi, USA. Moreover, one group of animals also received the Biofield Energy Treatment per se by the same Biofield Energy Healer under similar conditions at GVK Biosciences laboratory, Hyderabad, India. This Biofield Treatment was provided for ~3 minutes through the Biofield Energy Healer’s unique Energy Transmission process (the Trivedi Effect®), administered to the test formulation and animal without touching. Similarly, the control formulation was subjected to “sham” healer for ~3 minutes, under the same laboratory conditions. The “sham” healer did not have any knowledge about the Biofield Energy Treatment. After that, the Biofield Energy Treated and untreated test items were kept in similar sealed conditions and used for the study as per design.
In Vivo Pharmacokinetics Study
Animals
Male Sprague-Dawley (SD) rats (body weight 230 to 270 grams) were procured from Liveon Biosciences, Bangalore, India. Animals were housed in polycarbonate cage. Temperature and humidity were maintained at 22 ± 3°C and 40%-70%, respectively and illumination was controlled to give a sequence of 12 hours light and 12 hours dark cycle. The temperature and humidity were recorded by autocontrolled data logger system. All the animals were provided laboratory rodent diet (Vetcare India Pvt. Ltd, Bengaluru). Reverse osmosis water treated with ultraviolet light was provided ad libitum. The experiments using animals in this investigation were performed in accordance with the guidelines provided by the Committee for the Purpose of Control and Supervision of Experiments on Animals (CPCSEA) as published in The Gazette of India, January 7, 2010 and protocol approved by the Institutional (GVK Bio) Animal Ethics Committee (IAEC approval number: BA-011).
Experimental design
Rats were divided into three groups (n = 3): group 1 (Gr. 1) – per oral (p.o.) dosing of untreated vitamin D3, group 2 (Gr. 3) – per oral (p.o.) dosing of Biofield Energy Treated vitamin D3 and group 3 (Gr. 3) – per oral (p.o.) dosing of untreated vitamin D3 in Biofield Energy Treated animals. All animals were received per oral dose at 500 µg/kg of vitamin D3 solution formulation. The dose (500 µg/kg) of the test item was chosen based on the preliminary experiments performed in our laboratory and observed the quantifiable concentration of this analyte in rat plasma.
Formulation Preparation
Solution formulations of the test item was prepared in 14% v/v propyleneglycol, 1% v/v Tween 80, 45% v/v PEG, and 40% w/v 2-Hydroxypropyl-β-cyclodextrin in distilled water. All formulations were prepared freshly prior to dosing. The dose volume for per oral route was 5 mL/kg.
Pharmacokinetic Studies
The solution of test formulations was freshly prepared for per oral dosing. All rats were fasted overnight and the fasting continued up to 4 hours post dosing with free access to drinking water. The oral test formulation was administered at 500 µg/kg dose through oral gavage using an 18G stainless steel intubation cannula. The dosing volume administered was 5 mL/kg. Blood samples (~120 µL) were collected from the jugular vein catheter of three rats from each group at each time point [pre-dose, 0.25, 0.5, 1, 2, 4, 8, 24, 36, 48, 72 and 96 hours (p.o.)]. Samples were collected into labeled micro centrifuge tubes, containing 20% w/v K2EDTA as an anticoagulant. Plasma samples were separated from the blood by centrifugation at 2500 g for 10 min at 4 ± 2°C and stored below -40°C (Thermo Scientific, USA) deep freezer until bioanalysis.
LC-MS/MS Analysis
Analysis of rat plasma samples was performed using API 5500 QTRAP Applied Biosystem-Sciex LC/MS/MS (Concord, Ontario, Canada) triple quadruple mass analyzer system with an interface connected to a Shimadzu UFLC system (Shimadzu Corp., Japan). The optimum operating parameters were determined by atmospheric pressure chemical ionization (APCI) interface in positive ion mode. A generic mass spectrometry parameters of the analyte were developed and used for the analysis. These parameters were the declustering potential range (80), collision energy range (21), collision cell exit potential range (13), curtain gas (40 arbitrary units), collisionally activated dissociation gas (medium), ionspray voltage (5500 V), source temperature (550°C), and ion source gas 1 (70, arbitrary units each). Interface heaters were kept on for the analyte. The analyte was detected by positive ion spray in the multiple reaction monitoring mode (MRM) mode using predetermined parent/product mass transition ion pairs. The parameters of the selected MRM monitoring transitions for the [M + H] - precursor ion to selected product ion (m/z) were optimized with 383.20/365.40 (25-hydroxyvitamin D3), and 515.30/276.20 (telmisartan as an internal standard). The whole system was controlled by Analyst Classic 1.6.3® software (Applied-Biosystem-Sciex, Concord Canada). Stock solutions of 25-hydroxyvitamin D3 and telmisartan (internal standard, IS) were prepared in methanol at approximately 2.368 mg/mL and 0.98 mg/mL, respectively and subsequently diluted which were used for the bioanalysis.
The extraction procedure for plasma samples or the spiked in to plasma calibration standards were identical. A 50 µL sample of either study sample or spiked calibration standard was added to individual pre-labeled micro- centrifuge tubes. A 50 µL sample of either study sample or spiked calibration standard/quality control samples were added to individual wells of 96 well plate with 500 µL capacity. 200 µL of internal standard (IS) prepared in acetonitrile (ACN) was added to the samples in deep well plate except for blank, where 200 µL of ACN was added and vortexed for 5 minutes. Samples were centrifuged for 10 minutes at a speed of 4000 rpm (3220 g) at 4 oC. Following centrifugation, 120 µL of supernatant was transferred into 1000 µL capacity deep well plate and mixed with 120 µL of methanol: water, 50:50 v/v. The plate was kept in the auto- sampler for the LC-MS/MS analysis.
A Shimadzu LC-20AD LC system (Shimadzu Corp., Japan) was connected to a SIL -20 AC HT auto-sampler (Shimadzu Corp., Japan). The supernatant were injected (20 µL) onto a 50 x 4.6 mm (3.5 µm) Waters, X-Bridge, C18 HPLC column (Waters, Massachusetts, Ireland). Analytes were eluted using a gradient elution program with a mobile phase consists of 0.1% formic acid in water (pump A) with methanol (pump B) at a flow rate of 1.0 mL/min. The column temperature was at 40 °C and the sample temperature was at 15 °C. The following linear gradient was employed for the separation: 80% A for 0.01 min, 5% A at 2. 5 min and hold to 4.5 min, 80% A at 4.9 min, and hold to 6.0 min. The 25-hydroxyvitamin D3 and telmisartan elution times were approximately 3.61 and 2.45 min, respectively. Peak integration, regression and calculation of analytes concentration were computed using Analyst Classic (Version 1.6.3) software. The calibration curve was performed by linear curve fit of the peak area ratio (analyte/internal standard) as a function of the concentration in the respective matrix. A weighting of 1/x2 (where x is the concentration of a given calibration standard level) was found to be optimal. The Lower limit of quantification (LLOQ) in rat plasma was 1.02 ng/mL for 25-hydroxyvitamin D3. Analysis of 25-hydroxyvitamin D3 in plasma (1.09 to 252.65 ng/mL) showed a repeatability (relative standard deviation-RSD%) of 2.2% to 9.6% and accuracy of 85.70% to 95.65%.
Pharmacokinetic Analysis
The pharmacokinetic parameters of 25-hydroxyvitamin D3 were obtained by noncompartmental analysis module in Phoenix WinNonlin® (Version 7.0) (Pharsight, Mountain View, CA). The areas under the concentration time curve (AUC0-t and AUC0-∞) were calculated by linear trapezoidal rule. The terminal elimination rate constant (kel) was determined by regression analysis of the linear terminal portion of the log plasma concentration-time curve. The terminal half- life (T1/2) was estimated at 0.693/ke. The apparent oral clearance (CL/F) was calculated for per oral dose divided by AUC, respectively. Peak 25-hydroxyvitamin D3 concentrations (Cmax) and the times when they occurred (Tmax) were derived directly from the data. The relative oral bioavailability (Fr) was estimated by AUCtreated/AUCcontrol.
Statistical Analysis
All mean values are presented with their standard deviation (mean ± S.D.). Data were analyzed for statistically significant differences using analysis of variance followed by the two-sided unpaired Student’s t-test. Differences were considered to be significant at a level of p<0.05.
Results and Discussions
In vivo Effects of Biofield Energy Treatment for 25-hydroxyvitamin D3 Pharmacokinetics in Rats
The low plasma exposure of active metabolite(s) of vitamin D3 after a single oral dose of administration in rat is a key factor that may reduce the efficacy of vitamin D3 [43]. Therefore, we have taken this study to evaluate the pharmacokinetic properties of Biofield Energy treated vitamin D3. To the authors’ knowledge, this is the first report to demonstrate the effects of Biofield Energy Treatment on vitamin D3 pharmacokinetics in rats after a single dose of oral administration. Pharmacokinetic profiles of both vitamin D3 and 25-hydroxy (OH)-vitamin D3 in three different groups were compared in male rats following a single oral (gavage) dose of vitamin D3.
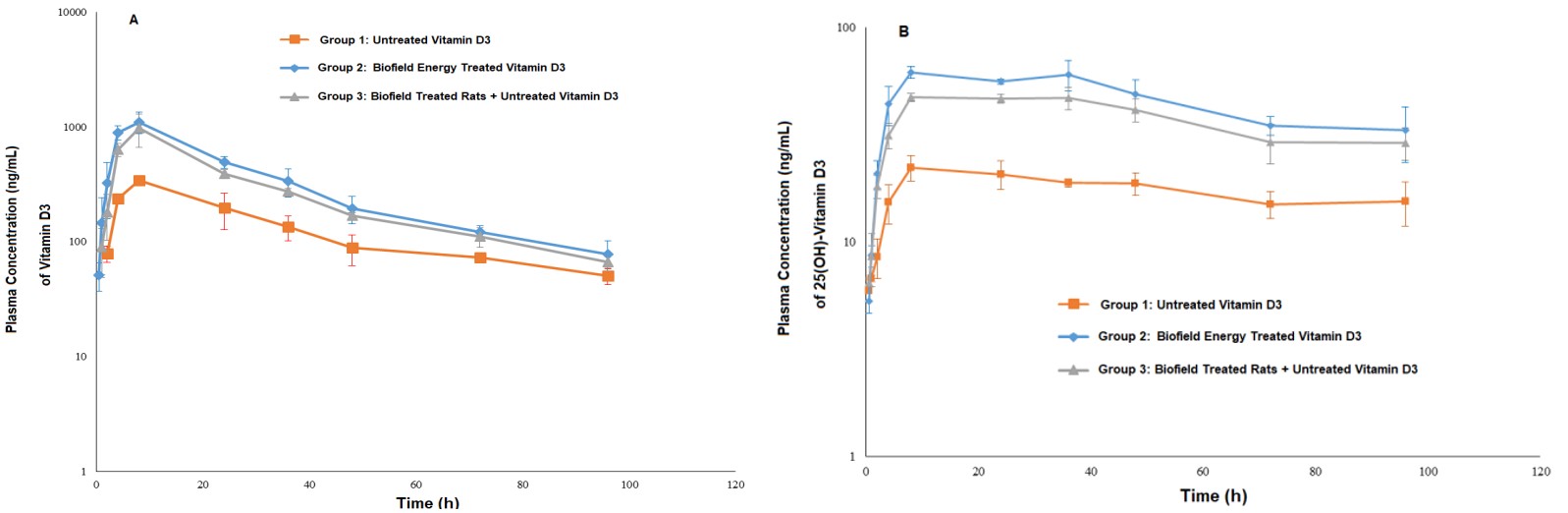
The mean pharmacokinetic parameters and profiles of vitamin D3 and 25-hydroxy(OH) vitamin D3 in the rat plasma after a single oral administration of vitamin D3 solution formulations in three different groups are summarized in Table 1 and Figure 1, respectively.
| Gr. 1-Untreated vitamin D3 | Gr. 2-Biofield Energy Treated vitamin D3 | Gr. 3-Biofield Energy Treated Rats + Untreated vitamin D3 | |
|---|---|---|---|
| Vitamin D3 | |||
| Formulation | Solution | Solution | Solution |
| Cmax(ng/mL) | 341.12 ± 19.16 | 1104.68 ± 232.4 | 980.75 ± 314.98 |
| Tmax(hours) | 8.0 ± 0.00 | 8.0 ± 0.00 | 8.0 ± 0.00 |
| AUC0-t(ng/mL*hours) | 12415.61 ± 2242.23 | 31736.66 ± 5191.99 | 26287.10 ± 2312.28 |
| T1/2(hours) | 56.69 ± 26.3 | 27.12 ± 0.41 | 33.83 ± 10.45 |
| MRTlast(hours) | 34.04 ± 0.53 | 28.42 ± 0.75 | 29.17 ± 0.84 |
| Kel(hours-1) | 0.01 ± 0.00 | 0.19 ± 0.03 | 0.17 ± 0.02 |
| % Change in Fr(relative oral bioavailability) | 155.62 | 111.73 | |
| 25-hydroxy (OH) - Vitamin D3(active metabolite) | |||
| Cmax(ng/mL) | 23.54 ± 2.71 | 64.56 ± 6.86 | 49.85 ± 3.57 |
| Tmax(hours) | 13.33 ± 9.24 | 17.33 ± 16.17 | 22.67 ± 14.05 |
| AUC0-t(ng/mL*hours) | 1684.97 ± 85.75 | 4402.53 ± 454.95 | 3605.29 ± 216.50 |
| T1/2(hours) | - | - | - |
| MRTlast(hours) | 45.89 ± 1.30 | 43.60 ± 1.65 | 44.49± 0.92 |
| Kel(hours-1) | 0.01 ± 0.00 | 0.01 ± 0.00 | 0.01 ± 0.00 |
| % Change in Fr(relative oral bioavailability) | 161.28 | 113.96 |
Table 1: Pharmacokinetic parameters of vitamin D3 and 25-hydroxy (OH) vitamin D3 after per oral (p.o.) administration at 500 µg/k
The data are expressed as mean values. AUC, area under the plasma concentration–time curve from 0 hours to infinity; Cmax: peak concentration; Tmax: time to reach peak concentration; T1/2: terminal half-life; Kel: absorption rate constant; MRT: Mean residence time; p.o.: per oral, Fr: Relative oral Bioavailability.
The Cmax of vitamin D3 in control group (G1) was 341.12 ng/mL after 8.0 hours, whereas it was 1104.68 ng/mL and 980.75 ng/mL for the vitamin D3 after 8.0 hours in G2 and G3 group, respectively. The results showed that plasma vitamin D3 had an oral exposure (AUC0–t) of 12415.61 ng/ mL in control (untreated) group. After the Biofield Energy Treatment by a renowned Biofield Energy Healer, Mahendra kumar Trivedi, the relative oral exposure (AUC0–t) of vitamin D3 was significantly increased by 155.62% and 111.73% in G2 & G3 groups, respectively as compared to the control group. Biofield Energy Treatment also significantly improved the plasma peak concentration (Cmax) of vitamin D3 by 223.84% and 187.5% in G2 and G3 groups, respectively as compared to the control group.
The Cmax of 25-hydroxy (OH)-vitamin D3 in control group (G1) was 23.54 ng/mL after 13.33 hours, whereas it was 64.56 ng/mL and 49.85 ng/mL for the 25-hydroxy (OH)-vitamin D3 after 17.33 hours and 22.67 hours in G2 and G3 group, respectively. The results showed that plasma 25-hydroxy (OH)-vitamin D3 had an oral exposure (AUC0–t) of 1684.97 ng/mL in control (untreated) group. After the Biofield Energy Treatment, the relative oral exposure (AUC0–t) of 25-hydroxy (OH)-vitamin D3 was significantly increased by 161.28% and 113.96% in G2 & G3 groups, respectively as compared to the control group. Biofield Energy Treatment also significantly improved the plasma peak concentration (Cmax) of 25-hydroxy (OH)-vitamin D3 by 174.25% and 111.77% in G2 and G3 groups, respectively as compared to the control group.
After oral administration, plasma concentrations of active metabolite, 25-hydroxy (OH)-vitamin D3 in all three groups were declined with slow excretion. The mean residence time (MRTlast) and elimination rate constant (K_el_) were unaltered in all three groups. These data demonstrates significant increased plasma exposure and peak plasma levels of both vitamin D3 and 25-hydroxy (OH)-vitamin D3 in rats which might be translated into altered in vivo biological activity of vitamin D3. The significant improvement (>100%) of relative oral bioavailability observed of both vitamin D3 and 25-hydroxy (OH)-vitamin D3 that might be due to the alteration of physicochemical properties and thermal properties of vitamin D3 by the Biofield Energy Treatment.
The results indicated that the Biofield Energy Treated vitamin D3 and animals per se significantly improved the rate and extent of oral absorption of both vitamin D3 and 25-hydroxy (OH)-vitamin D3. The increased absorption may be due to the increased specific surface area of the vitamin D3 formulation, or the stability of the vitamin D3 formulation in the gastrointestinal tract or due to the altered vitamin D3 metabolism pathways. The significant improvement of relative oral bioavailability of both vitamin D3 and 25-hydroxy (OH)-vitamin D3 in the Biofield Energy Treated groups might be helpful to show better pharmacological effects in vitamin D3 insufficiency associated different disease conditions such as diabetes, cardiovascular disease, hypertension, pregnancy complications, rheumatoid arthritis, osteoporosis, multiple sclerosis, thyroiditis, inflammatory bowel disease, cancer etc.
Conclusions
The study results showed that the relative oral exposure (AUC0–t) of vitamin D3 was significantly increased by
155.62% and 111.73% in G2 and G3 groups, respectively as compared to the control group. Biofield Energy Treatment also significantly improved the plasma peak concentration (Cmax) of vitamin D3 by 223.84% and 187.5% in G2 and G3 groups, respectively as compared to the control group. This study results also showed that the relative oral exposure (AUC0–t) of 25-hydroxy (OH)-vitamin D3 (metabolite) was significantly increased by 161.28% and 113.96% in G2 and G3 groups, respectively as compared to the control group (G1). Biofield Energy Treatment also significantly improved the plasma peak concentration (Cmax) of 25-hydroxy (OH)- vitamin D3 by 174.25% and 111.77% in G2 and G3 groups, respectively as compared to the control group. After oral administration, plasma concentrations of active metabolite, 25-hydroxy (OH)-vitamin D3 in all three groups were declined slowly. The mean residence time (MRTlast) and elimination rate constant (K_el_) for this metabolite were unaltered in all three groups. These data suggest that Biofield Energy Treated vitamin D3 might be influenced in vivo biological activity of vitamin D3 due to increased plasma exposure (AUC) of both vitamin D3 and metabolite level, 25-hydroxy (OH)-vitamin D3 in rats. There was significant improvement (>100%) of relative oral bioavailability of both vitamin D3 and 25-hydroxy (OH)-vitamin D3 that might be due to the alteration of physicochemical properties and thermal properties of vitamin D3 by the Biofield Energy Treatment. Hence, Biofield Energy Healing Treatment is considered as an innovative strategy which opens new opportunities in order to improve the poorly absorbed drug/nutraceuticals/herbal extracts that can improve the therapeutic performance of orally active molecules. Overall, the data suggest that vitamin D3 level can be maintained for longer period of time which can be helpful to convert slowly into specific hydroxylated forms of vitamin D3. As a result, The Trivedi Effect®-Energy of Consciousness Healing Treatment might be beneficial to the different groups of cardiac and kidney transplant patients, hip fracture patients, osteoporetic patients, hyperparathyroidism and cancer patient, neurodegenerative and ischemic heart patients.
Acknowledgements
Authors are grateful to GVK Bioscience, Trivedi Science, Trivedi Global, Inc., Trivedi Testimonials and Trivedi Master Wellness for their support throughout the work.
References
-
Henry HL (2011) Regulation of vitamin D metabolism. Best Practice & Research Clinical Endocrinology & Metabolism 25(4): 531-541.
-
Holick MF (2003) Vitamin D: A millenium perspective. Journal of Cellular Biochemistry 88(2): 296-307.
-
Holick MF, Smith E, Pincus S (1987) Skin as the site of vitamin-d synthesis and target tissue for 1,25-dihydroxyvitamin-D3 - use of calcitriol (1,25-dihydroxyvitamin-D3) for treatment of psoriasis. Archives of Dermatology 123(12): 1677-1683.
-
Ganji V, Zhang X, Shaikh N, Tangpricha V (2011) Serum 25-hydroxyvitamin D concentrations are associated with prevalence of metabolic syndrome and various cardiometabolic risk factors in US children and adolescents based on assay adjusted serum 25-hydroxyvitamin D data from NHANES 2001-2006. American Journal of Clinical Nutrition 94(1): 225-233.
-
Berg AH, Scherer PE (2005) Adipose tissue, inflammation, and cardiovascular disease. Circulation Research 96(9): 939-949.
-
Zhao GX, Ford ES, Li CY, Croft JB (2012) Serum 25-hydroxyvitamin D levels and all-cause and cardiovascular disease mortality among US adults with hypertension: The NHANES linked mortality study. Journal of Hypertension 30(2): 284-289.
-
McGreevy C, Williams D (2011) New insights about vitamin D and cardiovascular disease A narrative review. Annals of Internal Medicine 155(12): 820-865.
-
Grant WB, Peiris AN (2010) Possible role of serum 25-Hydroxyvitamin D in Black-white health disparities in the United States. Journal of the American Medical Directors Association 11(9): 617-628.
-
Fiscella K, Franks P (2010) Vitamin D, race, and cardiovascular mortality: Findings from a national US sample. Annals of Family Medicine 8(1): 11-18.
-
Bodnar LM, Simhan HN (2010) Vitamin D may be a link to black-white disparities in adverse birth outcomes. Obstetrical & Gynecological Survey 65(4): 273-284.
-
Fulgoni VL, Keast DR, Bailey RL, Dwyer J (2011) Foods, fortificants, and supplements: Where do americans get their nutrients? Journal of Nutrition 141(10): 1847- 1854.
-
IOM (2017) Dietary reference ranges for calcium and vitamin D.
-
Van Schoor NM, Lips P (2011) Worldwide vitamin D status. Best Pract Res Clin Endocrinol Metab 25(4): 671- 680.
-
NIST/NIH (2017) Vitamin D Metabolites Quality Assurance Program.
-
Lehmann U, Hirche F, Stangl GI, Hinz K, Westphal S, et al. (2013) J Clin Endocrinol Metab 98(11): 4339-4345.
-
Lutgendorf SK, Mullen-Houser E, Russell D, Degeest K, Jacobson G, et al. (2010) Preservation of immune function in cervical cancer patients during chemoradiation using a novel integrative approach. Brain Behav Immun 24(8): 1231-1240.
-
Ironson G, Field T, Scafidi F, Hashimoto M, Kumar M, et al. (1996) Massage therapy is associated with enhancement of the immune system’s cytotoxic capacity. Int J Neurosci 84(1-4): 205-217.
-
Giasson M, Bouchard L (1998) Effect of therapeutic touch on the well-being of persons with terminal cancer. J Holist Nurs 16(3): 383-398.
-
Peck SD (1998) The efficacy of therapeutic touch for improving functional ability in elders with degenerative arthritis. Nurs Sci Q 11(3): 123-132.
-
Turner JG, Clark AJ, Gauthier DK, Williams M (1998) The effect of therapeutic touch on pain and anxiety in burn patients. J Adv Nurs 28(1): 10-20.
-
Barnes PM, Bloom B, Nahin RL (2008) Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report 12: 1-23.
-
Rubik B (2002) The biofield hypothesis: Its biophysical basis and role in medicine. J Altern Complement Med 8(6): 703-717.
-
Trivedi MK, Patil S, Shettigar H, Mondal SC, Jana S (2015) The potential impact of biofield treatment on human brain tumor cells: A time-lapse video microscopy. J Integr Oncol 4(3): 1000141.
-
Trivedi MK, Patil S, Shettigar H, Gangwar M, Jana S (2015) _In vitro_ evaluation of biofield treatment on cancer biomarkers involved in endometrial and prostate cancer cell lines. J Cancer Sci Ther 7(7): 253-257.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Shettigar H, Mondal SC, Jana S (2015) Antibiogram pattern of _Shigella flexneri_: Effect of biofield treatment. Air Water Borne Diseases 4(2): 1000122.
-
Trivedi MK, Patil S, Shettigar H, Mondal SC, Jana S (2015) Antimicrobial susceptibility pattern and biochemical characteristics of _Staphylococcus aureus_: Impact of Biofield treatment. J Microb Biochem Technol 7(4): 238- 241.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Shettigar H, Mondal SC, Jana S (2015) Effect of biofield energy treatment on _Streptococcus_ group B: A postpartum pathogen. J Microb Biochem Technol 7(5): 269-273.
-
Trivedi MK, Patil S, Shettigar H, Bairwa K, Jana S (2015) Phenotypic and biotypic characterization of _Klebsiella_ _oxytoca_: An impact of biofield treatment. J Microb Biochem Technol 7(4): 202-205.
-
Trivedi MK, Branton A, Trivedi D, Gangwar M, Jana S (2015) Antimicrobial susceptibility, biochemical characterization and molecular typing of biofield treated _Klebsiella pneumoniae_. J Health Med Inform 6(5): 206.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Gangwar M, et al. (2015) Antibiogram, biochemical reactions, and genotypic pattern of biofield treated _Pseudomonas_ _aeruginosa_. J Trop Dis 4(1): 1000181.
-
Trivedi MK, Tallapragada RM, Branton A, Trivedi D, Nayak G, et al. (2015) Biofield treatment: A potential strategy for modification of physical and thermal properties of gluten hydrolysate and ipomoea macroelements. J Nutr Food Sci 5(5): 1000414.
-
Trivedi MK, Nayak G, Patil S, Tallapragada RM, Jana S, et al. (2015) Bio-field treatment: An effective strategy to improve the quality of beef extract and meat infusion powder. J Nutr Food Sci 5(4): 389.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Gangwar M, et al. (2015) Morphological and molecular analysis using RAPD in biofield treated sponge and bitter gourd. American Journal of Agriculture and Forestry 3(2): 264- 270.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Gangwar M, et al. (2015) Effect of biofield energy treatment on chlorophyll content, pathological study, and molecular analysis of cashew plant (_Anacardium_ _occidentale_ L.). Journal of Plant Sciences 3(6): 372-382.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Gangwar M, et al. (2016) Molecular analysis of biofield treated eggplant and watermelon crops. Adv Crop Sci Tech 4(1): 208.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Mondal SC, et al. (2015) Effect of Biofield treated energized water on the growth and health status in chicken (_Gallus gallus_ _domesticus_). Poult Fish Wildl Sci 3(2): 1000140.
-
Trivedi MK, Nayak G, Patil S, Tallapragada RM, Latiyal O, et al. (2015) An evaluation of biofield treatment on thermal, physical and structural properties of cadmium powder. J Thermodyn Catal 6(2): 1000147.
-
Trivedi MK, Nayak G, Patil S, Tallapragada RM, Latiyal O, et al. (2015) Effect of Biofield energy treatment on physical and structural properties of calcium carbide and praseodymium oxide. International Journal of Materials Science and Applications 4(6): 390-395.
-
Trivedi MK, Tallapragada RM, Branton A, Trivedi D, Nayak G, et al. (2015) Characterization of physical, thermal and structural properties of chromium (VI) oxide powder: Impact of biofield treatment. Journal of Civil & Environmental Engineering 5(6): 1000196.
-
Trivedi MK, Mohan TRR (2016) Biofield energy signals, energy transmission and neutrinos. American Journal of Modern Physics 5(6): 172-176.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Balmer AJ, et al. (2017) Evaluation of the energy of consciousness healing treated _Withania somnifera_ (Ashwagandha) root extract using LC-MS, GC-MS, and NMR spectroscopy. American Journal of Biomedical and Life Sciences 5(2): 16-25.
-
Trivedi MK, Branton A, Trivedi D, Nayak G, Balmer AJ, et al. (2017) Evaluation of physicochemical, spectral, thermal and behavioral properties of the biofield energy healing treated sodium selenate. Science Journal of Chemistry 5(2): 12-22.
-
Grady L, Thakker K (1980) Stability of solid drugs: Degradation of ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3) at high humidities and elevated temperatures. J Pharm Sci 69(9): 1099‐1102.
- Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review