Right Bundle Branch Block in Right Ventricular Apical Pacing
Right ventricular (RV) apical pacing results in left bundle branch block pattern with left axis deviation in electrocardiogram (ECG). Appearance of right bundle branch block (RBBB) pattern on electrocardiogram after RV apical pacing commonly denotes septal perforation or coronary sinus pacing. 59 year old male underwent permanent pacemaker implantation (VVI) for symptomatic complete heart block with tined pacing lead fixed in right ventricular apex. 12 lead ECG showed RBBB pattern after implantation, despite the lead in RV apex. Some of the mechanisms proposed are incorrect lead placement, left ventricle getting activated first through anomalous pathways, pacing stimulus travelling through right bundle to atrioventricular node retrogradely and down the left bundle branch and lastly diseased right ventricular conduction system leading the pacing stimulus to penetrate left ventricular conduction system early.
Introduction
Right bundle branch block (RBBB) pattern on 12 lead ECG after right ventricular (RV) apical pacing is a matter of concern as it commonly denotes septal perforation or coronary sinus pacing. However, this may not be the case always as RBBB pattern may occur in rare instances even when the lead is in the distal septum or RV apex. We came across a case of symptomatic third degree AV block who underwent permanent pacemaker implantation, following which RBBB pattern occurred despite the presence of lead in RV apex.
Case Report
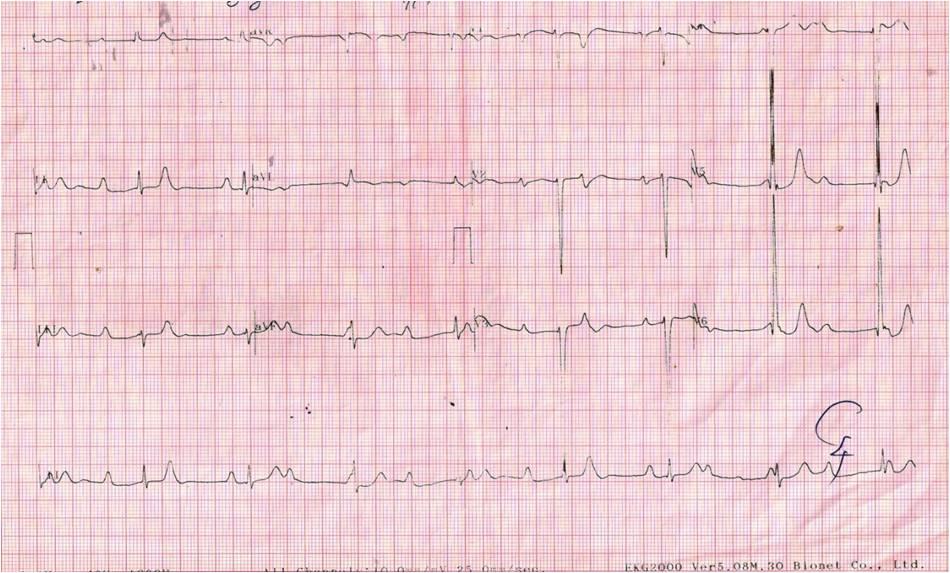
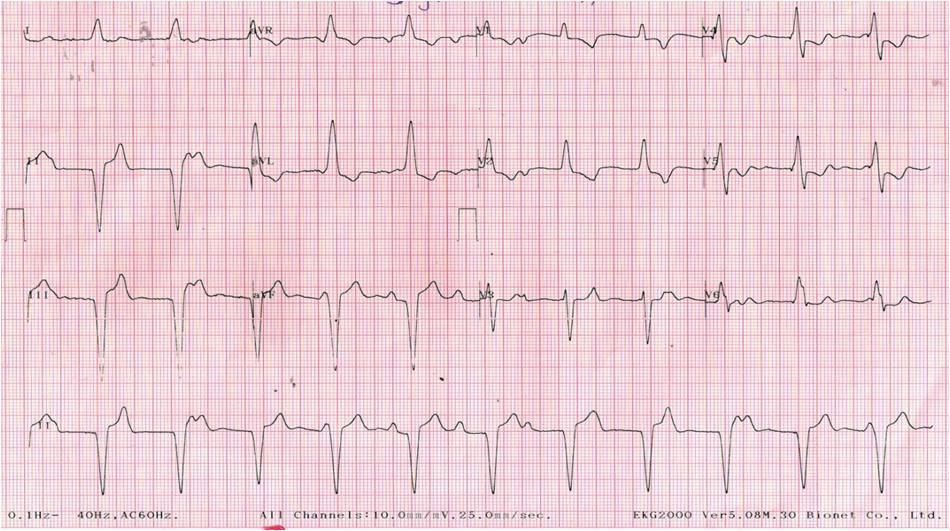
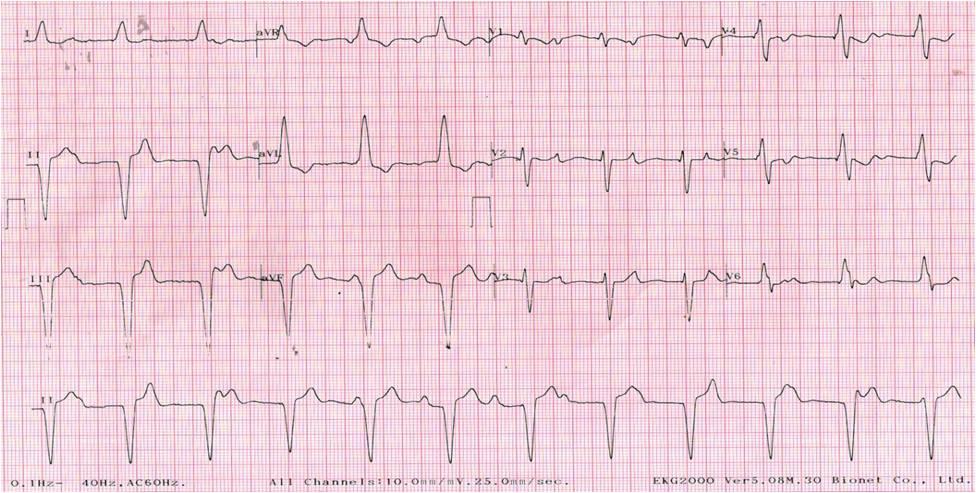
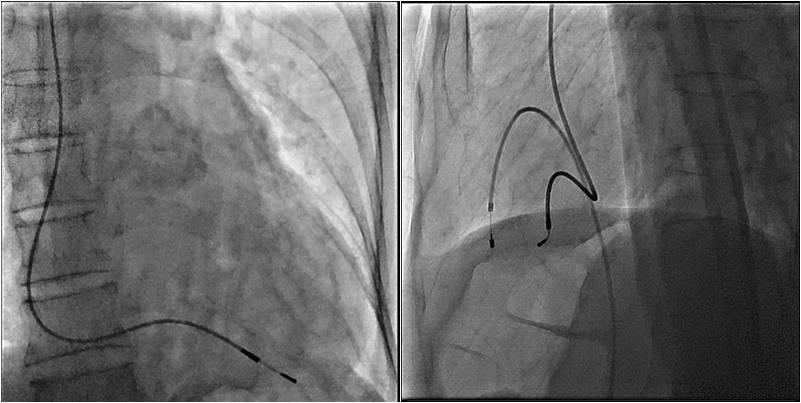
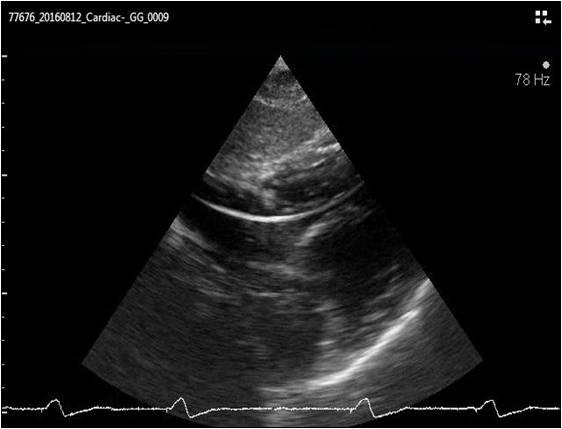
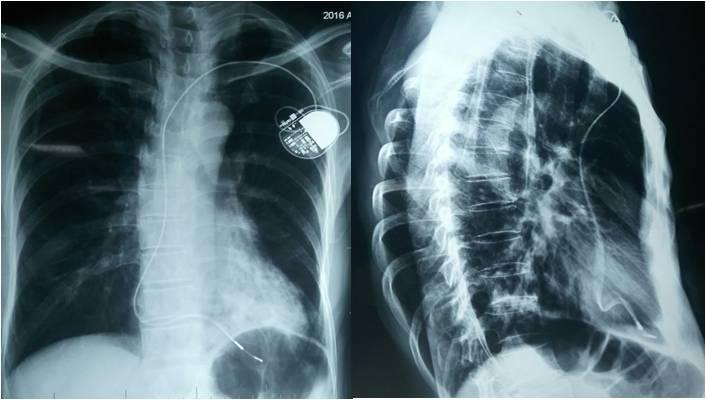
ECG done prior to cataract surgery 1 year ago was normal. General examination was normal. Pulse rate was 46/min, regular & felt in all peripheral pulses. Blood Pressure was 130/70 mmHg in both upper limbs. JVP showed intermittent cannon ‘a’ wave. Systemic examination was normal. ECG showed atrioventricular (AV) dissociation with atrial rate of 100 bpm & ventricular rate of 48 bpm suggestive of III° AV Block with suprahisian escape rhythm (Figure 1). Echocardiography showed no wall motion abnormality with normal ejection fraction. Holter monitoring showed complete heart block throughout with average heart rate of 54 bpm, minimum heart rate of 38 bpm and longest R- R interval was 2.7 seconds. Baseline investigations including thyroid function tests were normal. Permanent pacemaker implantation (MEDTRONIC RELIA) with VVI mode was done via left subclavian approach under local anaesthesia. Bipolar endocardial tined pacing lead was positioned in RV apex which was confirmed by fluoroscopy in both AP & lateral views (Figure 4). Procedure was uneventful. Post procedure ECG showed pacing rhythm with RBBB morphology in leads V1 & V2 with frontal QRS axis of around -60o (Figure 2). Echocardiography revealed pacing lead in RV apex (Figure 5). Notwithstanding, serial ECGs taken showed pacing rhythm with RBBB pacing morphology in V1 & V2 leads. ECG done with leads V1 & V2 placed one inter costal space below the standard position showed disappearance of RBBB pattern in V1 & V2 (Figure 3). Chest X rays both PA & lateral views confirmed the lead position in RV apex (Figure 6). Hence, patient was reassured and discharged in stable condition. During follow up patient was found to be asymptomatic and clinically stable. We report this case for its rarity.
Discussion
Right ventricular pacing usually results in pacing rhythm with left bundle branch block (LBBB) morphology on 12 lead surface ECG. RBBB morphology following RV pacing often indicates septal perforation or malpositioned pacing lead in coronary sinus or left ventricle (LV) which is known as “complicated RBBB pacing”. Malposition of pacing lead in the LV occurs when pacing lead inadvertently enters left atrium through patent foramen ovale or atrial septal defect and reaches the left ventricle [1]. Rarely, RBBB morphology can be seen even when the lead is correctly placed in right ventricular apex which is known as “uncomplicated or safe RBBB pacing” [2]. It is mandatory to differentiate between complicated and uncomplicated RBBB pacing as the former is potentially ominous which needs appropriate surgical intervention. Meticulous assessment with the help of ECG, chest X ray & 2-D echocardiography should be done to confirm the position of pacing lead. In literature, there are several case series of RBBB pattern that occurred following RV pacing. In 1985 Klein et al reported 8 cases of right ventricular pacing with RBBB morphology in leads V1 & V2, LBBB morphology in lead I and termed as “pseudo RBBB” pattern [3]. They also demonstrated that by placing leads V1 & V2 one intercostal space lower than the standard position, uncomplicated RBBB pattern could be eliminated if the lead is in distal septum or RV apex. However, RBBB pattern persisted when lead is in mid septum [3]. Friedberg, et al. demonstrated that RBBB pattern with maximal QRS vector oriented to left, superior and anterior may indicate uncomplicated right ventricular pacing where as QRS vector directed towards right, inferior and posterior may be a warning sign of right ventricle perforation [4]. In 1995, Coman & Trohman, et al. reported 7 cases of uncomplicated RBBB pattern in which pacing lead was confirmed to be in distal RV septum or RV apex [5]. They introduced a simple ECG based algorithm to distinguish between complicated and uncomplicated RBBB pacing using frontal plane QRS axis and precordial transition. A frontal QRS axis of 0o to -90o and precordial transition by lead V3 distinguishes RV septal or apical pacing from LV pacing with 86% sensitivity, 99% specificity and 95% positive predictive value [5]. The same frontal QRS axis of 0o to -90o but precordial transition after V4 denotes pacing in the posterior or postero lateral wall of left ventricle. Frontal QRS axes between 90o and 180o or -90o to -180o represents all other sites of left ventricle pacing [5]. In our patient, frontal QRS axis was around -60o and precordial transition occurred by lead V3 which satisfies the criteria of uncomplicated RBBB pacing. Several theories have been proposed to explain the mechanism of uncomplicated RBBB pattern following RV pacing. Mower MM, et al. proposed that when RV is paced, LV gets activated first through abnormal pathways or some portions of interventricular septum which belong to RV anatomically may act functionally and electrically as LV producing RBBB morphology [6]. Another explanation was that pacemaker stimulus may enter the right bundle branch and travels retrogradely to the AV junction and then down the left bundle branch [6]. Barold SS, et al. suggested that presence of severely diseased right ventricular conduction system causes right ventricular activation delay and early penetration of pacemaker stimulus into the left ventricular conduction system resulting in RBBB morphology [7].
Conclusion
Uncomplicated RBBB pacing pattern may occur as a benign variant following right ventricular apical pacing. Simple ECG based algorithm using frontal plane QRS axis and precordial transition may be used to differentiate between complicated and uncomplicated RBBB pacing. Other modalities like Chest X ray (PA and lateral views) and 2-D echocardiography can also be utilized to confirm the position of the lead.
References
-
Altun A, Akdemir O, Erdogan O, Aslan O, Ozbay G (2002) Left ventricular permanent lead insertion through the foramen ovale. A case report. Angiology 53: 609-611.
-
Yang YN, Yin WH, Young MS (2003) Safe right bundle branch block pattern during permanent right ventricular pacing. J Electrocardiol 36(1): 67-71.
-
Klein HO, Beker B, Sareli P, DiSegni E, Hadassa D, et al. (1985) Unusual QRS morphology associated with transvenous pacemakers. Chest 87(4): 517-521.
-
Friedberg HD (1980) Evaluation of unusual QRS complexes produced by pacemaker stimuli-with special reference to the vectorcardiographic and echocardiographic findings. J Electrocardiol 13(4): 409-415.
-
Coman JA, Trohman RG (1995) Incidence and electrocardiographic localization of safe right bundle branch block configuration during permanent ventricular pacing. Am J Cardiol 76(11): 781-784.
-
Mower MM, Aranaga CE, Tabatznik B (1967) Unusual patterns of conduction produced by pacemaker stimuli. Am Heart J 74(1): 24-28.
-
Barold SS, Narula OS, Javier RP, Linhart JW, Lister JW, et al. (1969) Significance of right bundle-branch block patternsduring pervenous ventricular pacing. Br Heart J 31(3): 285-290.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study