Inferior Wall Myocardial Infarction Haemodynamically Complicated by Associated Ebstein Anomaly
Ebsteins anomaly is an uncommon cardiac malformation affecting tricuspid valve and right ventricle. We report aware case of previously asymptomatic undiagnosed Ebstein anomaly presenting with decompensated haemodynamic status and cyanosis due to acute inferior wall myocardial infarction. Following aspects of this case makes it a rare presentation. Firstly, the unusual presentation of Ebstein anomaly as inferior wall myocardial infarction and atrio-ventricular dissociation. Secondly, the long asymptomatic period with two successfully completed pregnancies. Thirdly, particularly only right coronary artery involvement in Ebstein anomaly in this as well as previously reported 3 cases. Fourthly, coexistence of Ebstein anomaly with inferior wall myocardial infarction which lead to acute haemodynamic compromise and cyanosis. Lastly, this highlights the importance of early revascularization to salvage myocardium in already congenitally thin and fibrosed ventricles in Ebstein anomaly.
Introduction
Ebstein’s anomaly is a relatively rare congenital heart disorder characterized by downward displacement of septal and posterior leaflets of the tricuspid valve into right ventricle cavity. The usual presenting symptoms are cyanosis, right sided heart failure and arrhythmia. Progressive heart failure or tachyarrhythmia may worsen cyanosis. Acute myocardial infarction is less reported in Ebstein anomaly. The coronary arteries are usually normal except that the right coronary artery may be displaced superiorly and posteriorly because of aneurysmally dilated atrialized ventricle [1]. We report here a patient of Ebstein anomaly who was apparently asymptomatic and undiagnosed and presented with acute inferior wall myocardial infarction and her haemodynamic status and cyanosis was worsened more due to coexistence of above two mentioned conditions.
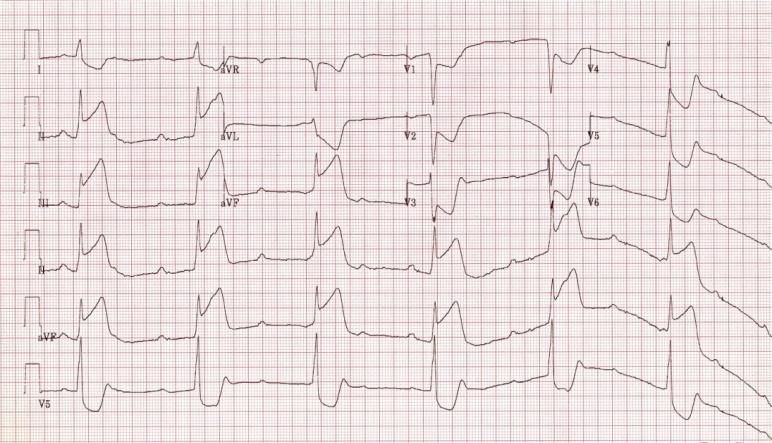
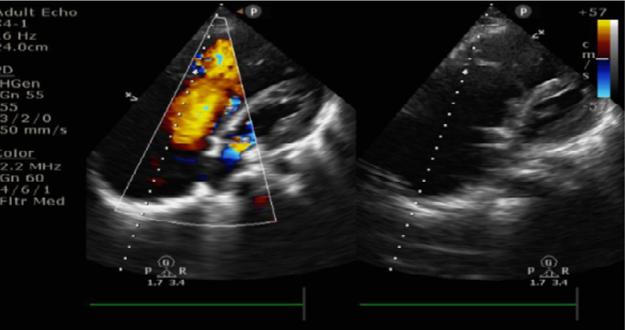
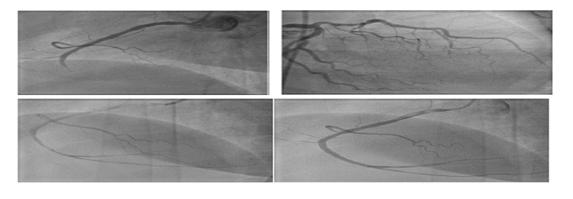
A 40 year female presented in cardiology emergency with complaint of sudden onset chest pain for 10 hours duration due to acute inferior wall myocardial infarction. Past history was suggestive of hypothyroidism. There was no history suggestive of diabetes, hypertension, addiction & any cardiac disorder. At presentation her vitals were heart rate 38/min, systemic blood pressure 80/40 mm Hg, respiratory rate of 30/min and cyanosed with oxygen saturation of 78%. Clubbing was not present. ECG revealed atrio-ventricular dissociation suggestive of complete heart block associated with ST elevation in leads II, III and a VF with reciprocal ST depression in leads I and a vl, chest leads V1-V6. Right sided chest leads also showed ST elevation suggestive of right sided infarction. Echocardiography revealed whole inferior wall and inferoseptal hypokinesia, large right atrium, small right ventricle with apical displacement of septal leaflet of tricuspid valve by 26mm and severe tricuspid regurgitation. A right to left intra atrial shunt was evident through patent foramen ovale. Ejection fraction was 30- 35%.Her routine biochemistry was normal with positive cardiac enzymes. The patient had no prior history of chest pain, exertional dyspnea and palpitations. Her two pregnancies were uneventful. Due to delayed presentation and worsened haemodynamic status patient was taken for emergent angiography which revealed, mid right coronary artery thrombotic cut off and normal left sided coronaries except minor plaque in proximal left anterior descending artery. Primary percutaneous intervention was performed successfully. Despite restoration of normal flow; patient was haemodynamically unstable after revascularization. There was no other evident cause of hypotension. Local access site haematoma, bleeding, anaphylaxis as causes of hypotension were ruled out. Patient was kept on Intra-aortic balloon pump support and mechanically ventilated to maintain vitals and oxygen saturation. Patient blood pressure improved after 48 hrs but she was persistently hypoxic and oxygen dependent. After 5 days, right heart catheterization was performed which revealed elevated right atrial pressure (mean right atrial pressure 13 mm Hg) and normal pulmonary artery (mean pressure12 mm Hg) and normal pulmonary capillary wedge pressure (6 mmHg), accounting for right to left interatrial shunt and systemic denaturation. Subsequently, patient was advised tricuspid valve replacement and closure of patent foramen ovale (Figures 1-3).
Discussion
Ebstein anomaly is uncommon congenital heart disease with varied presentations. The diagnosis of Ebstein anomaly is usually made by echocardiography. Apical displacement of the septal leaflet of the tricuspid valve by 8 mm/m2 or more (distance between septal insertion point of anterior tricuspid leaflet and septal insertion of anterior mitral leaflet divided by body surface area), along with an elongated sail-like appearance of the anterior leaflet, confirms the diagnosis [2]. Due to downward displacement of tricuspid valve, there occurs functional hypoplasia of right ventricle. Also the right ventricle free wall is often dilated and thin with fibrosis present in both right and left ventricle free walls [3]. Atrialized part of right ventricle has relatively less muscular tissue and is typically dilated. This part of right ventricle expands paradoxically during ventricular systole, acting as passive reservoir leading to decreased volume of ejected blood. Acute inferior wall and right sided myocardial infarction will further decompensate right ventricle which was already functionally hypoplastic. Hence this lead to acute haemodynamic decompensation as seen in our patient. Chest pain in Ebstein anomaly patients is usually of serous surface origin. A fibrinous pericardium has been found at necropsy over the atrialized right ventricle [2]. Coronary arteries are usually normal in Ebstein‘s anomaly. Secondly, progressive heart failure and arrhythmias are known to worsen cyanosis. But acute presentation with cyanosis due to myocardial infarction is an uncommon cause. Right ventricular and pulmonary artery pressures are usually normal in patients with Ebstein anomaly, although the right ventricular end-diastolic pressure may be increased. Right atrial pressure may be normal despite severe regurgitation of the tricuspid valve, due to chronic adaptation due to structural remodelling and enlarged right atrium. Raised right atrial pressure in our case, leading to right to left interatrial shunt and persistent hypoxia were due to inadequate compensation to sudden acute rise in pressure due to myocardial infarction. Role of Mechanical circulatory support devices (MCS) as bridge to recovery needs consideration in such situation. Use of left ventricle assist device (LVAD) can further worsen right ventricular function due to leftward septal shift that occurs with unloading of left ventricle because of left sided assist device. Leftward shifting of interventricular septum pulls the misaligned septal tricuspid leaflet and further worsens the tricuspid regurgitation and right ventricular function. So Biventricular assist devices or Total artificial heart (TAH) are to be considered in such a patient. Fukami, et al. reported a case of acute myocardial infarction complicated with Ebstein’s anomaly [3]. Batra R, et al. reported case of right ventricular myocardial infarction in 32 yr old male Ebstein patient with coronary angiogram showing non dominant right coronary artery with 95% stenosis in proximal segment [4]. This case reports rare presentation of Ebstein anomaly as chest pain due to myocardial infarction and further worsening haemodynamic status and right ventricular failure due to myocardial infarction in an Ebstein’s patient. Hence, this uncommon presentation highlights the importance of early revascularization to salvage myocardium in Ebstein anomaly where already RV myocardium is thin and fibrosed. Also it highlights Ebstein anomaly as an underlying uncommon cause of acute cyanosis in inferior wall myocardial infarction. Patient was apparently asymptomatic till 40 yr age and even completed two successful pregnancies which are highly unusual considering natural history of the disease. Also, all of the cases reported till now had inferior wall myocardial infarction. This needs further evaluation of the cause of particular involvement of right coronary artery in Ebstein’s heart.
References
-
Satpathy M (2008) Clinical diagnosis of congenital heart disease. 1st (Edn.), Jaypee.
-
Perloff JK (2012) Clinical recognition of congenital heart disease. 6th (Edn.), Philadelphia, PA: Elsevier Saunders.
-
Fukami K, Honda T, Haze K, Saito M, Umemoto M, et al. (1981) A case of acute myocardial infarction complicated withEbstein’s anomaly. KokyoToJunkan Japanese 29(10): 1125-1131.
-
Batra R, Nair M, Bhardwaj S, Kaul UA, Arora R, et al. (2002) Unusual ST–T Changes in Ebstein’s Anomaly with Occlusionof a Nondominant Coronary Artery. Indian Heart Journal 53(3): 292-294.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study