Risk Scores for Acute Vascular Events: Expectations and Limitations
Cardiovascular disease (CVD) is a major global health burden, despite declines in the mortality rate due to CVD in high-income and some middle-income countries, according to a study published in the Journal of American College of Cardiology (May 2017). The leading cause of healthcare related loss worldwide and in each region of the world is ischemic heart disease. Seventy years of dedicated research under the leadership of the National Institutes of Health and Boston University by the pioneering researchers of the now famous Framingham Heart Study, has provided a wealth of knowledge on the modifiable risk factor functions. One of the great contributions of FHS is that early work by this group opened up and supported the whole field of preventive cardiology by identifying modifiable risk factors for heart disease. Identification of these risk factors also raised the expectations of public in terms of possible reduction or reversal or prevention of this disease by the optimal management of these observed risks. In view of the fact, this was a one of a kind study that received the support of NIH for the longest time, generated more than 3000 articles; expectations of policy makers as well as general public have consistently remained high. Public health policies that were developed based on these findings have contributed significantly to the reduction in smoking, blood pressure, lowering of elevated levels of cholesterol and triglycerides. Considering the twin epidemics of obesity and type-2 diabetes, which are out of control worldwide, what we have gained in the management of modifiable risks may be lost, if the present trend in the increase of obesity and diabetes are not brought into control. Based on the results of FHS a Risk Score calculator has been developed. Development of new biomarkers, and new diagnostic imaging techniques, have provided additional data points for fine tuning the risk stratification for the development of the cardiovascular disease as well as for acute vascular events. In this brief overview, we have discussed some salient points and expressed our viewpoint on this topic of great public health importance.
Introduction
Coronary artery disease (CAD) is the leading cause of death for both men and women worldwide [1]. More than half of the deaths due to heart disease in the USA in 2015 were men. That does not mean that women are free of heart disease. They are equally at risk but at a later stage in their life. About 800,000 Americans die every year from heart disease. The American Heart Association developed methodology to project future costs of care for hypertension, coronary heart disease, heart failure, stroke, and all other related causes from 2010 to 2030. This methodology avoided double counting of costs for patients with multiple cardiovascular conditions. By 2030, 40.5% of the adult US population is projected to have some form of CAD. Between 2010 and 2030, real (208 billion) total direct medical costs of CAD are projected to triple, from $273 billion to $818 billion [2]. Elevated blood pressure, high LDL cholesterol, and smoking are the key risk factors. Other risks which promote heart disease include; inflammation, excess weight, subclinical atherosclerosis, endothelial dysfunction, obesity, type-2 diabetes, metabolic syndrome, poor diet, sedentary habits and excess alcohol consumption [3, 4, 5, 6, 7, 8]. The Framingham Heart Study (FHS) is a project of the National Heart, Lung and Blood Institute (NHLBI), USA, and the Boston University School of Medicine (BUSM) (www.framinghamheartstudy.org). Started in 1948, the family-based study developed much of the earliest scientific evidence of the relationship between cardiovascular disease, smoking, obesity, diabetes, high blood pressure and high cholesterol. Framingham Heart Study is one of the most informative and longest running studies on cardiovascular disease. The FHS leaders are Vasan Ramachandran MD, the BUSM principal investigator and Daniel Levy, MD, the NHLBI Director. More than 3000 articles based on the results of these ongoing studies have been published. Based on the collective knowledge gained by these studies, researchers formulated Framingham risk functions, risk score algorithms and risk calculators. Clinicians, patients, healthcare workers, and wellness programs use these calculators to estimate, decades in advance, individual risks for developing cardiovascular diseases. If one makes a search for information on cardiovascular disease risk score, Google and other search engines provide links to a variety of sites, including Risk Score Charts, European Society of Cardiology Risk Score, American Heart Association Risk Score for Heart and Stroke, The Reynolds Risk Score, Canadian Acute Coronary Syndrome Risk Score, Heart disease risk calculator (Mayo Clinic), ACC/AHA ASCVD Risk Calculator, and ASCVD Risk Estimator. Most calculators use a 10-year time frame (77%), but a few use 5-year time frame (7%), 3-year (3%) and lifetime (7%) risk. From the time FHS developed risk assessment analytics, based on their preliminary investigations, considerable progress has been made in this area, many population based studies have been conducted, and new biomarkers have been added for improving or fine tuning risk assessment algorithms. From the time FHS formulated Heart Disease Risk Score, to the present time, there are many populations based studies validating the benefits or otherwise of using this kind of risk assessment. In a short overview, we can only provide limited insights on this topic; Readers are urged to consult original articles and reviews on this subject [9, 10, 11, 12, 13, 14, 15]. Michael Allan and associates have published their findings on the agreement among cardiovascular disease risk calculators, in which they concluded that, “The decision as to which calculator to use for risk estimation has an important impact on both risk categorization and absolute risk estimates. This has broad implications for guidelines recommending therapies based on specific calculators” [16]. Over the years, researchers in this field have been adding additional risk factors to various currently existing risk formulas, to try and improve the risk stratification. After testing dozens of risk factors, Harvard researchers have found that just addition of two risk factors, C- reactive protein (CRP), and whether the patient had a previous heart attack before age 60 to the Framingham model, made the resulting predictions even more accurate [15]. On the other hand, based on the information collected from more than 24,000 women for a decade, researchers created a new tool called the Reynolds Risk Score [17]. This method of scoring (http://www.reynoldsriskscore.org/) did as well as Framingham Risk Score in later studies. In the National Cholesterol Education Program Adult Treatment Panel 111 guidelines published in 2001, estimation of CVD risk was recommended based on the Framingham Risk Score
for 10-year risk of MI. During joint guidelines development American Heart Association and American College of Cardiology made a decision to develop a new Risk Score. This resulted in the ACC/AHA Pooled Cohort Equations Risk Calculator. There is continuing improvements in the development of Risk Score Calculators [9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22]. Having said that, we would like to inform the readers that currently there are no Risk Calculators that are 100% predictive of acute vascular events (Heart attacks and Stroke). On the other hand, cardiovascular researchers at the University of Minnesota have taken a totally different approach to the management of cardiometabolic disorders. Rasmussen Center for Cardiovascular Disease Prevention at the University of Minnesota under the leadership of Professor Jay Cohn claims, that they take prevention a step beyond traditional search for risk factors [23, 24, 25, 26]. Professor Cohn and associates advocate the management of the disease aggressively, rather than to focus on the management of conventional risk factors. Their comprehensive disease assessment includes following tests: resting blood pressure, retinal-eye blood vessel analysis, electrocardiogram, measurement of large and small artery elasticity, ultrasound of the heart (left ventricle), ultrasound of the carotid (neck) artery thickness, walking treadmill exercise test, lipid panel, blood glucose, C-reactive protein (CRP), NT-pro BNP, and urinary micro albumin. Patients have been followed for the last 18 years with no history of cardiovascular disease. In a recent article in the American Journal of Medicine, Professor Cohn concludes that, “In order to develop strategies to prolong cardiovascular disease-free life expectancy, studies in early stages of disease aimed at slowing disease progression should be encouraged rather on the current focus no risk reduction” [27]. There is considerable debate about whether CAD Risk screening of heart disease in asymptomatic individuals especially in diabetic subjects will offer a better preventive care. In view of the fact that diabetic subjects are at a greater risk for acute vascular events, researchers have felt a greater need to early detection of silent CAD in these subjects. In addition to exercise electrocardiogram test (EET), recent emerging imaging noninvasive CAD screening modalities include, stress echocardiography (SE), stress radionuclide perfusion imaging (SRPI), coronary artery calcium scoring (CACS), and computed tomography coronary angiography (CTCA). Experts favoring noninvasive screening feel the need to improve the risk stratification and the reduction of scintigraphic CAD progression with invasive treatment. A systematic review and meta-analysis suggests reduction of cardiac events with the use of CAD screening strategy in asymptomatic diabetic patients. According to the authors, compared with standard care, non-invasive CAD screening reduced cardiac events by 27% in asymptomatic diabetic subjects [28]. In a series of articles published recently (2014-2018), in the European Heart Journal-Cardiovascular Imaging, on the topic related to the benefits of non-invasive imaging, researchers concluded that, “The addition of coronary computed tomography angiography (CCTA) improved category-free net reclassification (cNRI) of major adverse cardiovascular events” (MACE) [28, 29, 30, 31]. Furthermore, among elderly patients under 65 or older than 65, individuals experienced higher risk-adjusted hazards for MACE for non-obstructive, one-, and two vessels, with similar event rates for three vessel or left main compared with under 65 years individuals, suggesting additional risk with each advancing decade of life [31]. In spite of the fact that several recent studies have suggested additional non-invasive imaging for improved risk stratification in diabetic subjects, opponents of this diagnostic approach advocate optimal medical treatment without screening, because revascularization has not been convincingly demonstrated to reduce or reverse CVD events in diabetic patients. The Association for Eradication of Heart Attack (AEHA) has made an observation, which is worth considering when calculating the risk for acute vascular events. According to them, inability to predict the risk for major cardiac adverse events accurately in the case of Ex- President Bill Clinton (Vulnerable Patient) illustrates the serious gap in our understanding of the underlying causes that precipitate these events. The organization in their press release reports that, the former president’s heart disease was not detected in his regular check-ups when physicians screened for traditional risk factors, including cholesterol and an ECG-stress test. On the other hand, the same organization, AEHA Shape Task Force applauded President Bush’s medical team for recognizing the value of screening for prevention of an unpredicted attack. Medical team found a small amount of calcification in the President’s coronary arteries through non-invasive CT imaging. Soon after this incident was reported Professor Jay Cohn of University of Minnesota, a member of the AHEA Shape Task Force said, “We are pleased to see that the President’s team is leading the way for the rest of the medical community by adopting screening for subclinical disease”. He further expressed his hope, “that a comprehensive vascular structural and functional assessment will be included in every American’s preventive care”. A recent study published in the Journal
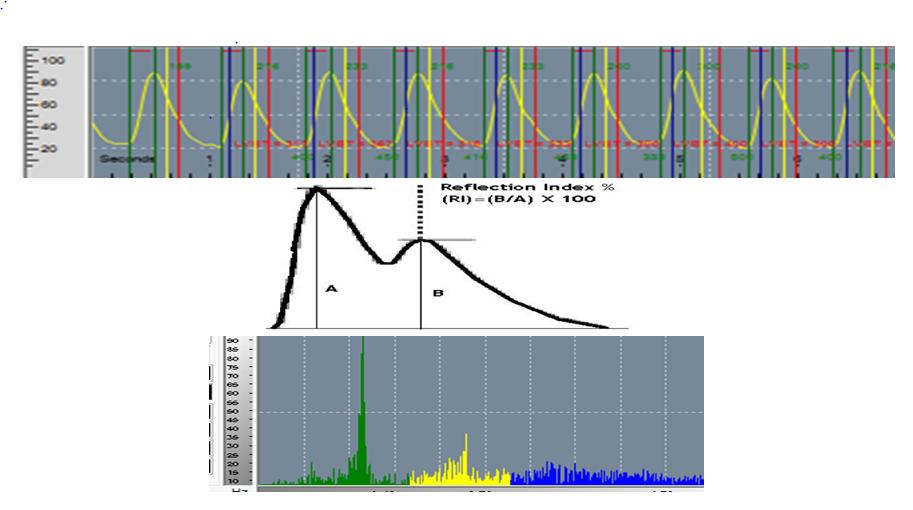
of American College of Cardiology reported that 88 percent of heart attack victims would have been considered low to moderate risk if they were tested with current national guidelines [32]. Dr Shah, Chief Cardiologist at Cedars-Sinai Medical Center in Los Angles says, “We have to seek direct anatomical evidence of arterial plaque build-up or thickening using non-invasive imaging technology”. In a recent article in the Journal of American College of Cardiology, Professor Valentin Fuster (Director, Zena and Michael A. Weiner Cardiovascular Institute, The Mount Sinai Hospital, New York), and his associates demonstrated that after age and male sex, LDL- Cholesterol was the main predictor of the presence of arterial atherosclerotic plaques [33]. Using the latest non- invasive imaging technology they demonstrated that, “atherosclerotic plaques were present in 50% of the middle-aged individuals with no classical risk factors and they also had hardened arteries. Researchers of this study concluded that, “these findings could help improve cardiovascular risk prevention in the general population even before the appearance of conventional risk factors, an example of primordial prevention”. This sub-analysis of the PESA study (Progression of Early Subclinical Atherosclerosis) evaluated 1779 study participants who had no classical risk factors. This observation by Professor Fuster and associates brings back the immediate need for the development of non-invasive cost effective tests for determining the subclinical atherosclerosis, hardening of the arteries, endothelial dysfunction, and altered blood flow dynamics in non- symptomatic or asymptomatic individuals [34, 35]. Common clinical factors such as age, gender, ethnicity, excess weight, obesity, hypertension, type-2 diabetes, hyper lipidemia, and family history are still the predominant indicators for developing coronary artery disease. There is increasing interest in developing a systems biology approach of combining various biomarkers for risk stratification. As mentioned in the previous paragraph, risk markers related to atherosclerosis, alterations in the blood flow velocity and endothelial function or dysfunction, become very important factors for risk stratification. Risk markers for inflammation, oxidative stress, cardiac injury (troponin), fibrosis, and changes in the intimal thickness also play a very important role in the progress of the disease. In view of these observations, there seems to be two different approaches to the management, one aimed at using the known biomarkers for risk stratification and the other as suggested by the University of Minnesota researchers to assess the status or progress of the disease itself rather than focus on risk factors [27]. Then the major question that comes to mind is where do we begin this CVD management? We have discussed in our earlier articles that earliest risk for developing cardio metabolic diseases is during the intrauterine growth (fetal origin of adult disease, [3, 4, 5, 6, 7]. If we follow this logic then childhood obesity, oxidative stress, inflammation, endothelial dysfunction, also become part of the sequelae for CVDs. A team of experts from Sweden concluded from their studies, “that in elderly men with or without cardiovascular disease, addition of several biomarkers of CVD and renal abnormalities substantially improves the risk stratification for death from cardiovascular causes beyond that of a model that is based only on established risk factors” [36]. In a novel study Ridker and associates from Harvard University demonstrated the role of inflammation in inducing acute CVD events [37]. Dr. Paul Ridker, Director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital, at Boston, USA says that, “For the first time we have been able to definitely show that lowering inflammation independent of cholesterol, reduces cardiovascular risk. The study was conducted with over 10,000 patients, who had previously heart attack and had persistently high levels of high sensitive C-reactive protein (hsCRP), a marker of inflammation. The drug tested was Canakinumab a monoclonal antibody that neutralizes interleukin 1β signaling, thereby suppressing inflammation. Hypothesis for this approach was developed based on the fact that of the patients on high statin therapy, there were still a significant proportion of those who still had increased hsCRP. A new concept of “residual inflammatory risk” was developed based on this observation. These evidence- based observations led to the development of Cantos Trial, which represents a seminal study from biomarkers to molecular mechanism relevant for therapeutic strategies. In the Cantos Trial, using a specific antibody for interleukin 1βsignaling the role of inflammation was validated. In the HOPE study researchers studied the impact of multiple biomarkers for the prediction of recurrent cardiovascular events in the heart outcomes. They concluded that, “Although levels of various inflammatory biomarkers are significantly related to future cardiovascular risk, their incremental predictive value is modest”. In their study they found that a model consisting of simple traditional risk factors and Nt-pro BNP provided the best clinical prediction in the secondary-prevention population [38]. Researchers from Quebec, Canada based on the results of their study suggested that using two simple and inexpensive measurements triglyceride and waist circumference one can identify patients with intra-abdominal obesity, which is a characteristic feature of the South Asian phenotype [39]. A large population-based collaborative study between University of Minnesota researches and the staff of Madras Diabetes Research Foundation (MDRF), Chennai, India, also showed similar results [40]. Now that we have discussed briefly FHS defined Risk Score Functions, various Risk Score Calculators, use of non-invasive imaging technologies and biomarkers for improving risk score stratification, let us review some newer emerging technologies, which may bring further strength to the risk assessment and risk prediction. Researchers (Dr Aaron Fenster and Dr. David Spence) at the Western University’s Robarts Research Institute, Canada, have shown that 3-dimesnional ultrasound measurements of atherosclerosis can evaluate effects of therapies for atherosclerosis much more efficiently than current methodologies [41, 42]. Any device that can measure carotid plaque volume and its progression or regression is an important tool for research and patient management. David Spence and associates have shown that carotid plaque volume measurement before and after therapies (statin) using 3D ultra sound technology, show effects of therapy in as short a time as 3 months. In view of this success story, we are exploring the possibilities of developing such emerging technologies to follow the blood flow dynamics as well as subclinical atherosclerosis in peripheral arteries or regional vascular beds. If we consider the current needs in imaging technology, it becomes evident that monitoring of the blood flow at regional vascular beds seems to be superior, to monitoring the carotid artery flow and drawing conclusions that such measurement truly represents flow conditions in the entire vascular tree. Yet another method that we are trying to explore is measuring pulse flow velocity at various pulse points. There are very many flexible pressure sensors available in the market and these could be effectively employed to get the pulse wave recordings. The data obtained from such measurements can be further analyzed by plethysmography to get information on change in blood flow or blood volume related to the artery stiffness as we have done in our earlier studies using pulse Oximeter [42, 43, 44, 45] (LD- Technologies, Miami, Fl.www.ldteck.com). Use of such pressure sensors will enable us to develop wearables to collect data from various pulse points about any alterations in the regional blood flow dynamics (Figure 1).
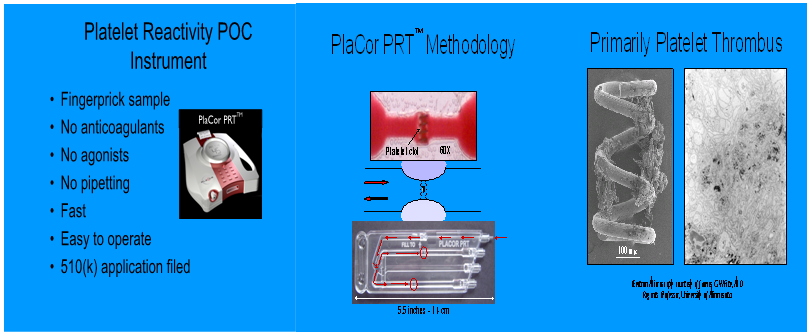
Conclusion
We have briefly described the importance of monitoring various risks for developing cardiovascular disease. Diligent work of Framingham researchers and continued funding of the NIH has resulted in the availability of a wealth of knowledge on this topic. In view of the fact, FHS is one of the longest ongoing researches, (70 years), people expect results and recommendations that will reduce, reverse, or prevent cardiovascular diseases [46]. The guidelines, guideline statements, strategies developed by policy makers, professional societies and health care organizations, have contributed significantly in the management of common risk factors for CVD. Many population-based studies conducted in different countries with various ethnic groups have validated the benefits of using Framingham Risk Score. The coronary artery disease is a complex disease of the vasculature. In view of the multiple risks involved in the precipitation of acute vascular events (heart attacks and stroke) current risk scores can only give us approximate timeline for the development of disease. Several studies have shown that adding additional risk factors, using emerging diagnostic imaging techniques further improvements can be made in the risk stratification. According to Dr. Daniel Levy, the director NHLBI, current work by the FHS group is also looking at causal genes, and pathways contributing to cardiovascular disease. They are integrating information from genetic variations with expression of genes, with production of proteins, and the elaboration of small molecules (micro RNAs?) that modulate various metabolic pathways and processes. Having said that, we would like to inform the readers, that currently available risk score calculators do not include any “values” for the newer biomarkers or to the activation status of circulating blood. In the final analysis, the thrombotic or hemorrhagic state of the blood and the factors that modulate or promote this status, become very important factors in determining outcomes of any preventive strategy. According to the Non-communicable Disease Risk Factor Collaboration Group Report (The Lancet: April 2016), “If the post-2000 trends continue in the prevalence of type-2 diabetes, the probability of meeting the Global Millennium Target of halting or reducing the rise in the prevalence of this disease by 2025 to the level of 2020 is less than one percent”. Excess weight, obesity and type-2 diabetes are major contributors for the development of vascular diseases including ischemic heart disease and cerebrovascular disease. Although major emphasis of this overview was on the risk stratification for CVD and related acute events, we will have to remind the readers, that majority of the risk score calculators by and large only use common risk factors in computing the risk analysis. In view of this fact, the prediction is only a close guess and not hundred percent accurate. We also have made a distinction between risk assessment score for developing CVD, versus risk assessment score for predicting major adverse or acute vascular events. A better understanding of the mechanisms that modulate various pathways that lead to inflammation, oxidative stress, endothelial dysfunction, metabolic syndrome, structural-biochemical changes leading to alterations in the function of blood vessels and circulating blood, will provide the clinicians new and useful information for the optimal management of these chronic metabolic diseases. In addition, appropriate strategies should be developed to reduce, reverse or prevent obesity and type-2 diabetes, the two other modifiable risk factors. Acknowledgements: Author thanks, Dr Daniel Ericson, Founder CEO, SUBc, Inc, Rochester, Minnesota and Dr. William Howard, Founder CEO, PlaCor Inc., Minneapolis, Minnesota for their collaboration on PRT development and validation studies.
References
-
Fuster V (2014) Global burden of cardiovascular disease (Editorial): J Amer Coll Cardiol 64 (5): 520- 222.
-
Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, et al. (2011) Forecasting the future of cardiovascular disease in the United States: A policy statement from the American Heart Association. Circulation 123(8): 933-944.
-
Rao GHR, Kakkar VJ (2001) Coronary Artery Disease in South Asians: Epidemiology, Risk factors, and Prevention. JP Medical Publishers.
-
Rao GHR, Thanikachalam S (2005) Coronary Artery Disease: Risk promoters, pathophysiology, and prevention. JP Medical Publishers.
-
Rao GHR (2016) Handbook of Coronary Artery Disease. Springer Healthcare.
-
Rao GHR (2018) Prevention or reversal of cardiometabolic diseases. J Clin Prevent Cardiol 7(1): 22-28.
-
Rao GHR (2012) Risk assessment, risk prediction, and effective management of risk factors for cardiovascular diseases: View Point. J Clin Prevent Cardiol 1: 9-10.
-
Artigao-Rodenas LM, Carbayo-Herencia JA, Divison- Garrote JA, Gil-Guillén VF, Massó-Orozco J, et al. (2013) Framingham risk score for prediction of cardiovascular disease: A population-based study from Southern Europe. PLoS One 8 (9): e73529.
-
Marrugat J, Baena-Diez JM, Sala GM, Ramos R, Subirana I, et al. (2011) Relative validity of the 10- year cardiovascular risk estimate in a population cohort of the REGICOR study. Rev Esp Cardiol 64(5): 385-94.
-
Riddell T, Wells S, Jackson R, Lee AW, Crengle S, et al. (2010) Performance of Framinghamcardiovascular risk scores by ethnic groups in New Zealnd: PREDICT CVD-10. N Z Med 123(1309): 50-61.
-
Eichler K, Puhan MA, Bachman LM (2007) Prediction of first coronary events with the Framingham score: a systematic review. Am Heart J 153(5): 722-731.
-
Empana JP, Ducimetiere P, Arveiler D, Ferrières J, Evans A, et al. (2003) Are the Framingham and PROCAM coronary artery heart disease risk functions applicable to different European populations? The PRIME Study. Eur Heart J 24(21): 1903-1911.
-
Hemann BA, Bimson WF, Taylor AJ (2007) The Framingham Risk Score: an appraisal of its benefits and limitations. Amer Hear Hosp J 5(2): 9-96.
-
Reissigova J, Tomeckova M (2005) State of the art coronary heart disease risk estimations based on the Framingham heart study. Cent Eur J Public Health 13(4): 180-186.
-
Abou Diwan CH, Oghlakian GO, Antonios SI, Otrock ZK, Rebeiz AG (2004) The role of high sensitivity C- relative protein in coronary artery disease risk prediction: a review. J Med Liban 52(1): 39-47.
-
Allan GM, Nouri F, Korownyk C, Kolber MR, Vandermeer B, et al. (2013) Agreement among cardiovascular disease risk calculators. Circulation 127(19): 1948-1956.
-
Cook NR, Paynter NP, Eaton CB, Manson JE, Martin LW, et al. (2012) Comparison of the Framingham and Reynolds Risk Scores for global cardiovascular risk prediction in the multiethnic women’s health Initiative. Circulation 125(14): 1748-1756.
-
Mehta SR, Eikelboom JW, Rao-Melacini P, Weitz JI, Anand SS, et al. (2016) A risk assessment tool incorporating new biomarkers for cardiovascular events in acute coronary syndromes. The organization to assess strategies in ischemic syndromes (Oasis) risk sore. Can J Cardiol 32(11): 1332-1339.
-
Fibrinogen Studies Collaboration, Danesh J, Lewington S, Thompson SG, Lowe GD, et al. (2005) Plasma fibrinogen level and the risk of major cardiovascular disease and nonvascular mortality: an individual participant meta-analysis. JAMA 294(14): 1799-1809.
-
Emerging Risk Factor Collaboration, Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, et al. (2009) Major lipids, apolipoprotien, and risk of vascular disease. JAMA 302(18): 1993-2000.
-
Emerging Risk Factor Collaboration, Kaptoge S, Di Angelantonio E, Lowe G, Pepys MB, et al. (2010) C- reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. Lancet 375(9709): 132- 140.
-
Cohn JN, Hoke L, Whitman W, Sommers PA, Taylor AL, et al. (2003) Screening for early detection of cardiovascular disease in asymptomatic individuals. Am Heart J 146(4): 679-685.
-
Cohn JN, Duprez DA, Grandits GA (2005) Arterial elasticity as a part of a comprehensive assessment of cardiovascular risk and drug treatment. Hypertension 46(1): 217-220.
-
Duprez DA, Cohn JN (2008) identifying early cardiovascular disease to target candidates for treatment. J Clin Hypertension 10(3): 1751-1776.
-
Cohn JN (2016) Slowing progression of cardiovascular disease. J Am Coll Cardiol 67(14): 1698-1700.
-
Cohn JN: Cardiovascular disease progression: A Target for therapy? The Am J Med S0002-9343(18): 30313-30319.
-
Clerc OF, Fuchs TA, Benz DC, Gräni C1, Messerli M, et al. (2018) Non-invasive screening for coronary artery disease in asymptomatic diabetic patients: a systematic review and meta-analysis of randomized controlled trials. European J Cardiovasc Imaging.
-
Han D, O’Hartaigh, Gransar H, Lee JH, Rizvi A, et al. (2018) Incremental prognostic value of coronary computed tomography angiography over coronary calcium scoring for major adverse cardiac events in elderly asymptomatic individuals. European Heart J Cardiovascular Imaging 18(6): 675-683.
-
Weir-McCall JR, Fitzgerald K, Papagiorcopulo CJ, Gandy SJ, Lambert M, et al. (2017) Prevalence of unrecognized myocardial infarction in a low- intermediate risk asymptomatic cohort and its relation to systemic atherosclerosis. European Heart J Cardiovascular Imaging 18(6): 657-662.
-
Nakazato R, Arsajani R, Achenbach S, Gransar H, Cheng VY, et al. (2014) Age-related risk for major adverse cardiac event risk and coronary artery disease extent and severity by coronary CT angiography: results from15, 187 patients from the International Multisite CONFIRM study. European Heart J Cardiovascular Imaging 15(5): 586-594.
-
Scanlon PJ, Faxon DP, Audet AM, Carabello B, Dehmer GJ, et al. (1999) ACC/AHA guidelines for coronary angiography. A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on Coronary Angiography). Developed in collaboration with the Society for Cardiac Angiography and Interventions. J Am Coll Cardiol 33(6): 1757-1824.
-
Fernanez-Friera, Fuster V, López-Melgar B, Oliva B, García-Ruiz JM, et al. (2017) Normal LDL-cholesterol levels are associated with subclinical atherosclerosis in the absence of risk factors. J Am Coll Cardiol 70(24): 2979-2991.
-
Rao GHR, Gandhi PG (2014) Need for a non-invasive diagnostic platform for early detection and management of cardiometabolic disorders. J Clin Prevent Cardiol 3(3): 93-98.
-
Rao GHR (2016) Flow velocity, fluid dynamics and vascular pathophysiology. Scientific Pages of Heart 1(1): 1-8.
-
Zethelius B, Berglund L, Sundstrom J, Ingelsson E, Basu S, et al. (2008) Use of multiple biomarkers to improve the prediction of death from cardiovascular causes. N Engl J Med 458(20): 2107-2116.
-
Ridker PM, Everett BM, Thuren T, MacFadyen JG, Chang WH, et al. (2017) Antiinflammatory therapy with Canakinumab for atherosclerotic disease. N Engl J Med 377(12): 1119-1131.
-
Blankenberg S, McQueen MJ, Siena M, Pogue J, Balion C, et al. (2006) Comparative impact of multiple biomarkers and N-Terminal Pro-Brain Natriuretic peptide in the context of conventional risk factors for the prediction of recurrent cardiovascular events in the Heart Outcomes Prevention Evaluation (HOPE) study. Circulation 114(3): 201-208.
-
Arsenault BA, Lemieux I, Despres J, Wareham NJ, Kastelein JJ, et al. (2010) The hyper triglyceridemic- wasit phenotype and the risk for coronary artery disease: results from the EPIC-Norfolk prospective population study. CMAJ 182(13): 1427-1432.
-
Bajaj HS, Pereira MA, Anjana RM, Mohan V, Mueller NT, et al. (2014) Comparison of Relative waist circumference between Asian Indian and US adults. J Obesity pp: 10.
-
Spence JD (2006) Ultrasound measurement of carotid plaque: Uses in patient management, genetic research and evaluation of new therapies. Nature Clin Pract Neurology 12(11): 611-619.
-
Ainsworth CD, Blake CC, Tamayo A, Beletsky V, Fenster A, et al. (2005) 3D Ultrasound measurement of change in carotid plaque volume: A tool for rapid evaluation of new therapies. Stroke 36(9): 1904- 1909.
-
Gandhi PG, Rao GHR (2014) The Spectral analysis of photoplethysmography to evaluate an independent cardiovascular risk factor. Int J Gen Med 7: 539-547.
-
Gandhi PG, Rao GHR (2015) Detection of neuropathy using a SudoMotor test in type-2 diabetes. Degenerative Neurological and Neuromuscular Disease 5: 1-7.
-
Maarek AA, Gandhi PG, Rao GHR (2015) Identifying Autonomic Neuropathy and Endothelial Dysfunction in Type11 Diabetic Patients. EC Neuropathy 2: 63-78.
-
Johnson GJ, Sharda A, Rao GHR, Ereth MH, Laxson DD, et al. (2012) Measurement of shear-activated platelet aggregate formation: Utility in evaluation of Clopidogrel-Aspirin-induced platelet function inhibition. J Appl Clin Thromb Hemost 18(2): 140- 149.
-
Voelker R (2018) Framingham at 70: What we’ve learned about women and heart disease. JAMA.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study