Pattern of C - reactive Protein in Sudanese Patients with Acute Coronary Syndrome
Background and Objective: C-reactive protein (CRP) is an acute phase protein that is produced predominantly by hepatocytes under the influence of cytokines such as interleukin (IL-6) and tumor necrosis factor-alpha. C-reactive protein is an extensively studied inflammatory factor whose prognostic value in cardiovascular diseases in recent years has become increasingly important. This study aimed to determine pattern of C-reactive protein in patients admitted with acute coronary syndrome to the coronary care unit at Elobied Teaching Hospital. Patients and Methods: This is a prospective hospital-based study. The study included 102 patients who were consecutively admitted to the coronary care unit with the clinical diagnosis of acute coronary syndrome (ACS). The data were obtained through well-designed data sheet including age, gender, clinical presentation, risk factors together with complications and ECG findings. A written consent was obtained from each patient. Five milliliters of venous blood was withdrawn from each patient within 24 hours of admission, serum Troponin and C- reactive protein levels were measured. The data were analyzed using SPSS version18. Results: In this study, the mean age of patients was 58 ± 12 years. More than half of the patients were male (54%). Hypertension was found in 33% while 28% of patients were diabetic and 18% were smoker. In this series, STEMI was diagnosed in 40 % of patients. Mean level of serum troponin was12 ng/ ml. The level of CRP was remarkably high (Mean47 mg/l). Conclusion and Recommendation: In this study, the level of CRP was high in patients with acute coronary syndrome. Further studies are needed to evaluate the role of CRP as a predictor of cardiovascular outcome after ACS.
Introduction
C-reactive protein (CRP), an acute phase protein produced mainly by the liver in response to interleukin 6, is a marker of inflammatory processes that contribute importantly to atherogenesis, plaque disruption, and thrombosis. Indeed products of thrombosis, including thrombin and platelet derived growth factor, themselves cause vascular smooth muscle cells within the ruptured plaque to augment production of interleukin 6 (IL-6), amplifying hepatic CRP release, and completing a vicious cycle of thrombosis and inflammation in acute coronary syndromes. CRP may have additional pathogenic effects— specifically by activating the complement system and promoting tissue factor release from monocytes. Thus CRP is intimately involved with the pathogenic mechanisms that drive acute coronary syndromes, and is predictive not only of cardiovascular events in apparently healthy middle aged men and women but also of outcomes following presentation with unstable angina and myocardial infarction [1]. Joint analysis of troponin and CRP has shown that these makers are independent and additive. A simultaneous increase in the levels of both markers is associated with a very high risk, an increase in just one of them is associated with an intermediate risk, while there is good prognosis when there is no increase in either [2]. This study aimed to determine the pattern of C reactive protein in patients admitted with acute coronary syndrome to the coronary care unit at Elobied Teaching Hospital.
Patients and Methods
This is a prospective hospital-based study. The study included 102 patients who were consecutively admitted to the coronary care unit with the clinical diagnosis of acute coronary syndrome (ACS). The data were obtained through well-designed data sheet including age, gender, Clinical presentation, risk factors together with complications and ECG findings. A written consent was obtained from each patient. Five ml of venous blood was withdrawn from each patient within 24 hours of admission, serum Troponin and C- reactive protein levels were measured. The data were analyzed using SPSS version18.
Results
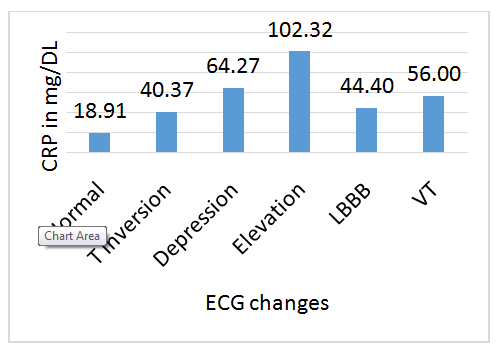
In this study, the mean age of patients was 58 ± 12 years. More than half of patients were male (54%). Hypertension was found in 33% while 28% of patients were diabetic and 18% were smoker. In this series, STEMI was found in 40 % of patients. ST segment depression was found in 12% of patients, LBBB in 4%, T wave inversion in 21%, while 23% of patients had normal ECG . The mean level of serum troponin was 12 ng/ ml. The level of CRP was remarkably high (Mean 47 mg/l). In the current study 9 % developed heart failure, arrhythmias and stroke were in 8% and 4% respectively. Three patients died with a mortality rate of 3%. In patients with heart failure means CRP was 94 mg /L. The mean levels of CRP were 44 mg/L and 10 mg/L in patients who developed arrhythmias and stroke respectively. The level of CRP was significantly high in patients with STEMI compared with other pattern of ECG changes (mean 102 mg/L). (Table 1) Mortality was associated with high level of CRP (mean 74mg/L) (Table 2).
- ECG change
- Frequency Percent %
- Normal ECG
- 23
- 22.5 %
- T wave inversion
- 21
- 20.6 %
- T wave depression
- 12
- 11.8 %
- T wave elevation
- 41
- 40.2 %
- LBBB
- 04
- 3.9 %
- Ventricular tachycardia (VT)
- 01
- 1.0 %
- Total
- 102
- 100 %
Table 1: ECG changes.
- Complication
- Frequency Percent %
- No complication
- 79
- 77.5 %
- Arrhythmias
- 08
- 7.8 %
- Heart failure
- 09
- 8.8 %
- Stroke
- 04
- 3.9 %
- Arrhythmia and heart failure
- 02
- 2.0 %
- Total
- 102
- 100 %
Table 2: Complications of ACS.
Discussion
In this study the level of CRP in patients with ACS was measured. The level of CRP was significantly high in patients with STEMI compared to other pattern of ECG changes, similar results were reported by Magdalena Krintus, et al. [3]. Patients with complications had significantly high level of CRP. Patients with heart failure had the highest level of CRP followed by arrhythmias and then stroke. The level of serum troponin, on the other hand is highest in patients with arrhythmia (mean 24ng\ml) followed by heart failure (mean 20ng\ml). The lowest level of serum troponin was found in patient with stroke (mean 4ng\l). These findings suggest that serum CRP and troponin have relatively independent prognostic significant. GUSTO IV ACS trial had demonstrated similar result [4]. This study showed that high level of CRP was associated with high in-hospital mortality. The correlation between the level of CRP in ACS and the long term risk of mortality was not addressed in this study; nevertheless some studies confirmed CRP as a predictor of one year and 20 months’ mortality [5, 6]. Another study indicated that patients presenting with ACS and high level of CRP have significant risk for death after 5 years and congestive heart failure after2 years [7]. Nevertheless, one study showed that there is no correlation between the level of CRP and ejection fraction [8]. Other studies showed weak association with the extent of coronary disease on angiography [9, 10].
Conclusion and Recommendation
In this study, the level of CRP was high in patients with acute coronary syndrome. Further studies are needed to evaluate the role of CRP as a predictor of cardiovascular outcome after ACS.
References
-
Kennon S, Timmis AD, Whitboum R, Knight C (2003) C-reactive protein for risk stratification in acute coronary syndrome? Verdict unproven. Heart 89(11): 1288-1290.
-
Bodi V, Sanchis J (2006) C-reactive protein in acute coronary syndrome. Looking Back in order to move Forward. Rev Esp Cardiol 59(5): 418-420.
-
Magdalena Krintus, Marek Kozinski, Anna Stefanska, et al. (2012) Value of C-Reactive Protein as a Risk Factor for Acute Coronary Syndrome: A Comparison with Apolipoprotein Concentrations and Lipid Profile. Hindawi Publishing Corporation 2012: 10.
-
James SK, Armstrong P, Barnathan E, Califf R, Lindahl B, et al. (2003) Troponin and C-reactive protein have different relations to subsequent mortality and myocardial infarction after acute coronary syndrome: a GUSTO-IV substudy. J Am Coll Cardiol 41(6): 916- 924.
-
Biasucci L, Liuzzo G, Grillo R, Caligiuri G, Rebuzzi A, et al. (1999) Elevated levels of C-reactive protein at discharge in patients with unstable angina predict recurrent instability. Circulation 99(7): 855-860.
-
Mueller C, Buettner H, Hodgson J, Marsch S, Perruchoud A, et al. (2002) Inflammation and long- term mortality after non-ST elevation acute coronary syndrome treated with a very early invasive strategy in 1042 consecutive patients. Circulation 105(12): 1412-1415.
-
Kavsak PA, MacRae AR, Newman AM, Lustig V, Palomaki GE, et al. (2007) Elevated C-reactive protein in acute coronary syndrome presentation is an independent predictor of long-term mortality and heart failure. Clin Biochem 40(5-6): 326-329.
-
Brunetti ND, Troccoli R, Correalale M, Pellegrino PL, Di Biase M, et al. (2006) C-reactive protein in patients with acute coronary syndrome: correlation with diagnosis, myocardial damage, ejection fraction and angiographic findings. Int j Cardio 109(2): 248-256.
-
Zebrack JS, Muhlestein JB, Horne BD, Anderson JL; Intermountain Heart Collaboration Study Group (2002) C-reactive protein and angiographic coronary artery disease: independent and additive predictors of risk in subjects with angina. J Am Coll Cardiol 39(4): 632-637.
-
Sabatine MS, Morrow DA, Jablonski KA, Rice MM, Warnica JW, et al. (2007) Prognostic significance of the Centers for Disease Control/American Heart Association high-sensitivity C-reactive protein cut points for cardiovascular and other outcomes in patients with stable coronary artery disease. Circulation 115(12): 1528-1536.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study