Early Diagnosis and Management of Type-2 Diabetes: A Case Study
Metabolic diseases, such as hypertension, obesity, type-2 diabetes, and vascular diseases, have reached epidemic proportions globally, contributing significantly to non-communicable disease (NCD)-related mortality. Non-communicable diseases account for 71% of global deaths annually, with cardiovascular diseases (CVDs) leading the statistics. The South Asian phenotype presents a unique set of clinical characteristics, including, typical visceral obesity, high triglycerides, increased low-density lipoprotein cholesterol (LDL-Cholesterol), insulin resistance, and high propensity for type-2 diabetes. Several clinical studies have demonstrated that risk factors such as unhealthy diets, lack of physical inactivity, tobacco use, and alcohol consumption drive the development and progression of these metabolic disorders. The Framingham Heart Study remains pivotal, identifying robust predictors of CVDs including hypertension, dyslipidemia, smoking, and diabetes. Hypertension, a widespread silent condition, stands as a significant precursor to premature mortality globally. Childhood obesity rates have escalated dramatically, correlating with the rise in unhealthy lifestyles. Type-2 diabetes, increasingly prevalent, underscores the potential reversibility through early detection and management strategies. Complications from poorly managed diabetes, including cardiovascular events and microvascular complications, emphasize the urgency for the development of effective preventive measures. The South Asian population exhibits distinct metabolic traits predisposing to insulin resistance, type-2 diabetes, and cardiovascular diseases, influenced by genetic, dietary, and lifestyle factors. Addressing these unique challenges through targeted lifestyle interventions holds promise for mitigating vascular disease risks among South Asians. This case study advocates for a proactive approach to early diagnosis of cardiometabolic risks and comprehensive management of identified risks, aiming to reduce the burden of heart disease among younger populations. Insights from current research underscore the critical need for integrated strategies encompassing genetics, lifestyle modifications, and community-based interventions to combat the escalating crisis of metabolic diseases worldwide.
Abbreviations
ABP: Ambulatory Blood Pressure; GLP: Glucagon Like Peptide; FHSG: Framingham Heart Study Group; CVDs: Cardiovascular Diseases; NCDs: Non-Communicable Diseases; SSATHI: Stanford South Asian Translational Heart Initiative; BP: Blood Pressure; ACE: Angiotensin-Converting Enzyme; LVH: Left Ventricular Hypertrophy; ICA: Internal Carotid Artery; ESV: End Systolic Volume; EDV: End Diastolic Volume; EF: Ejection Fraction.
Introduction
Metabolic diseases like hypertension, obesity, type-2 diabetes and vascular diseases, have rapidly increased to epidemic proportions worldwide [1, 2, 3]. Non-communicable diseases (NCDs) are responsible for 71% of the total number of deaths each year. The top four killers among NCDs with the highest number of deaths are cardiovascular diseases (CVDs) 17.9 million deaths annually, cancers (9 million), respiratory diseases (3.9 million) and diabetes (1.6 million). India leads the global top ten, in terms of the highest number of people with diabetes, with a current estimate of 74 million people [4]. The major risk factors contributing to the development and progress of metabolic diseases are unhealthy diets, lack of physical activity, tobacco use and alcohol consumption. Framingham Heart Study Group (FHSG) based in Framingham, Massachusetts, remains one of the longest-running and most influential epidemiological study in the world [5, 6]. Standard risk factors described by the FHSG remain strong predictors of CVDs over extended follow-up. The observed risks include; male sex, systolic blood pressure, antihypertensive treatment, high-density lipoprotein cholesterol, smoking, and diabetes [7, 8]. Hypertension is a silent medical condition, a major cause of premature death worldwide, over a billion people have this condition [9]. The number of obese children and adolescents worldwide has increased tenfold in the past four decades. The worldwide prevalence of obesity has tripled since 1975 due to unhealthy fast-food consumption and lifestyle changes [10]. Type-2 diabetes, which is on the rise worldwide, is preventable and in some cases reversible, if identified and managed early in the disease course [11]. Poorly managed diabetes condition leads to blindness, kidney failure, heart attacks, stroke and lower limb amputations [12]. Data from an international prospective study (EpiDREAM), suggests that dysglycemia is a strong risk factor for macrovascular and microvascular complications, and as such, approaching dysglycemia as a continuous risk factor, might represent a more effective preventive strategy for the management of diabetes-induced clinical complications [13].
Metabolic disease refers to a spectrum of metabolic dysregulation processes affecting obesity- linked insulin resistance, glucose homeostasis, altered lipid metabolism, and increased production of proinflammatory immune cells and cytokines [14]. Irrespective of the global efforts to halt or reduce the rising epidemic of metabolic diseases, there remain large disparities in the metabolic disease burden, especially in low-to middle-income countries. South Asians have a higher risk of developing insulin resistance, type-2 diabetes, and cardiovascular diseases than other ethnic groups. This increased risk seems to be related to a combination of risk factors, including genetics, diet, lifestyle, body composition and adverse levels of adipokines [15, 16]. According to experts at Stanford South Asian Translational Heart Initiative (SSATHI), there is a 40% higher chance of death from heart attacks among South Asians than the average population (https://stanfordhealthcare.org/ medical-clinics/stanford-south-asian-translational-heart- initiative/conditions.html). Stroke related deaths for South Asians are 55% higher than other ethnic groups. According to Kandula and associates of UC San Francisco, more than 60% of Cardiovascular disease patients worldwide belong to South Asian descent [16].
The South Asian phenotype presents a unique set of clinical characteristics, including, typical visceral obesity, high triglycerides, increased low-density lipoprotein cholesterol (LDL-Cholesterol), insulin resistance, and high propensity for type-2 diabetes [13, 17, 18]. Such metabolic alterations are closely linked to the development and progression of vascular diseases and acute vascular events. Addressing these metabolic alterations through lifestyle interventions is crucial for vascular disease prevention.
According to Dr. Amit Khera and associates at Harvard University, “Across four studies involving 55,685 participants, genetic and lifestyle factors were independently associated with susceptibility to coronary artery disease. However, among participants with high genetic risk, a favorable lifestyle was associated with a 50% lower relative risk of coronary artery disease than an unfavorable lifestyle [19]”. The purpose of presenting this case study is to share observations on this distinctive case (South Asian Phenotype), propose a road map for enhancing early diagnosis of the metabolic risks, and robust management of cardiometabolic risks. The ultimate goal is to contribute to a better understanding of the risks, development of a proactive approach to prevention and address the prevalence of heart disease among young individuals.
Case Study
The subject of this case study is of South Asian descent, who was born in India (08/23/1937), and migrated to the USA for his higher studies in 1965. The subject in question developed early signs of heart dysfunction at the age of
57. During his entire life, his health care was provided by three primary doctors, 1937-65 (India), 1972-2012 (Minneapolis, Minnesota), and 2012 to present Washington DC. The patient is a renowned researcher in the areas of cardiometabolic diseases, and as such was willing to undergo approved diagnostic tests as well as those that were in the developmental stages. In 1994, during a sightseeing tour in India, the subject noticed shortness of breath, while climbing a small hill (300 meters high). The primary physician in Minneapolis (Late Dr Azam Ansari) performed ECG tests and determined that probably left ventricular hypertrophy was the cause for the observed shortness of breath during uphill climbing. Uncontrolled hypertension is the most common cause of left ventricular hypertrophy (LVH). The blood pressure of the patient was 160/80. Thiazide diuretics and angiotensin-converting enzyme (ACE) inhibitors are the most common combination of antihypertensive medications recommended for such cases. In addition to the routine blood pressure monitoring during clinic visits, both conventional sphygmomanometers as well as ambulatory blood pressure (BP) were used to monitor BP before administering various types of medications, as well as for adjusting the dosage of anti-hypertensives. Initially, a combination of a thiazide diuretic and angiotensin-converting inhibitor was used to arrest and normalize LVH. Once this goal was achieved the use of Enalapril (Vasotec 5 Mg ) once daily was recommended.
In 2005, ambulatory blood pressure (ABP) was monitored again, for five days (24 hrs.) with a frequency of 30 minutes. Of these five-day observations, three days included post-changing of the dosage of an anti-hypertensive drug (50 Mgs of Atenolol). The quality of 24-hour ambulatory blood pressure monitoring was excellent. No abnormal symptoms were reported. Better systolic blood pressure control was achieved after adding Atenolol a first generation b-blocker. Better control of mean arterial pressure was observed. No significant fluctuations or peaks in blood pressure were observed during the day or at night.
In 2005, in addition to ABP monitoring a complete transthoracic cardiac ultrasound study was ordered to follow the progress or regression of left ventricular hypertrophy, ventricular function and valvular dysfunction. The left atrium was found enlarged at 46 mm. A mild concentric left ventricular hypertrophy was observed. The estimate of cardiac ejection fraction was 75%, which is almost normal for the age.
Experts concluded that compared to the previous echocardiographic study done at the University of Minnesota Hospitals in 1996, there seems to be definite evidence for mild left ventricular hypertrophy, mild mitral and aortic valve regurgitations, left atrial enlargement and diastolic dysfunction. Despite these findings, no stenosis or altered flow dynamics was observed.
In 1999, the patient developed a low-grade fever of unknown origin and suffered considerable loss of weight. He was administered a wide spectrum antibiotic, Levaquin. During this time, it was noticed that his fasting glucose was also considerably high (170mgs/Dl). Therefore, in addition to antibiotic, he also was administered Glucophage (750Mgs/ day). This patient had both primary hypertension, LVH and type-2 diabetes. There seems to be a close association between left ventricular diastolic dysfunction and aortic stiffness. Therefore, diagnostic studies were suggested to monitor the stiffness of the carotid and femoral arteries as well as for the presence of sub-clinical atherosclerosis. The pulse wave analysis was used for computing stiffness of the arteries using “Periscope” a newly developed “Diabetes Risk Profiler” in India (Genesis Medical Systems, Hyderabad), which uses brachial blood pressure and carotid-femoral pulse wave (PW) to find out aortic root pressure [20]. One measurement is taken at the carotid artery and one at the femoral artery and the difference is calculated by appropriate algorithms. Recommendations to measure PWV are included in the recent hypertension guidelines. PWV was determined by PeriScope in an 8-channel real-time PC- based simultaneous acquisition and analysis system. Patient (GR) blood pressure was 140/80, right brachial PWV was 1265, left brachial PWV was 1260 and pulse pressure was 50 mmHg, age-adjusted normal values.
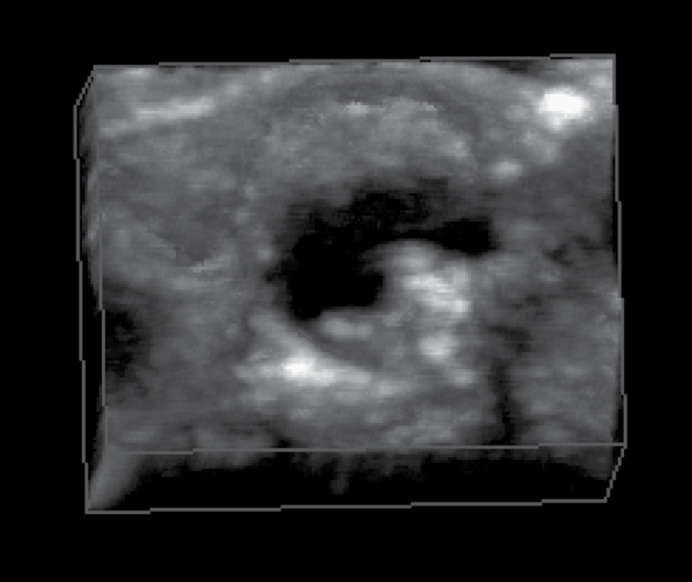
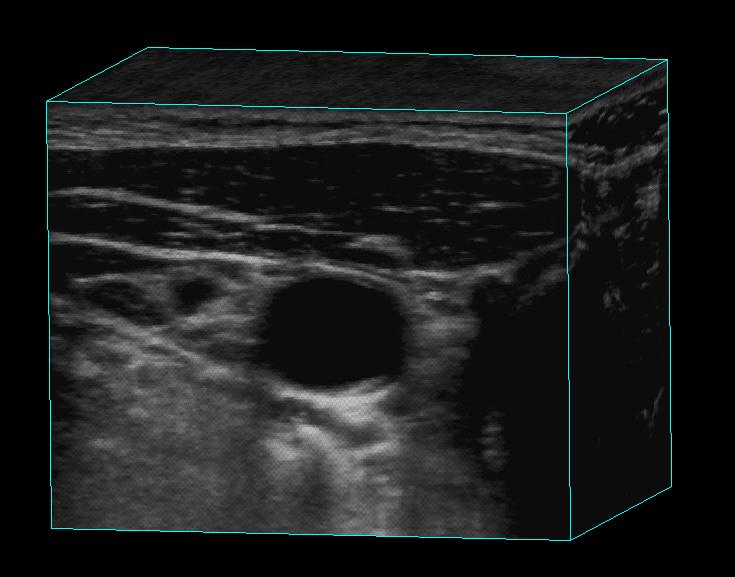
In 2005, patient (GR) visited Professor Aaron Fenster and Professor J David Spence at the Robarts Research Institute, in Ontario, Canada and got a carotid artery scan done by the experts. A 3-D scan of his carotid artery (A- GR) of the neck is shown in Figure 1. Compared to a scan of a patient with advanced atherosclerotic plaque (B), his carotid artery was relatively free of any visible plaques. In a bilateral carotid ultrasound Doppler study in 2010, minimal homogenous plaque formation was recorded without any flow disturbances (data not shown).
A
B
In 2007, blood chemistry was as follows; Cholesterol 140, Triglycerides 137, LDL- Cholesterol 76, VLDL- cholesterol 27, Cholesterol HDL ratio 3.7, Fasting glucose 164, HbA1c 7.0, Blood Pressure 140/70.
Medications included Metformin ER 500 Mg two tablets/ twice daily, Enalapril 10 Mg twice daily, Carvedilol 6.5 Mg twice daily, and Cyanocobalamin 1ml once a month. From 2007 to 2012 the blood glucose levels fluctuated and HbA1c varied from a low of 5.6 to 7.0 depending upon the anti- glycemic medications used. The patient even participated in a clinical study of twice- daily injectables, “Byetta”.
Three different Glucagon Like Peptide (GLP1) agonists were available at that time, -exenatide (Byetta) twice daily, liraglutide (Victoza) once a day, exenatide once a weak (Bydureon). Victoza seems to lower A1c more than the other two. Once a week exenatide causes less nausea than twice daily. Because of nausea caused by the drug, patient discontinued the use of exenatide and went back to the use of a combination of anti-glycemics.
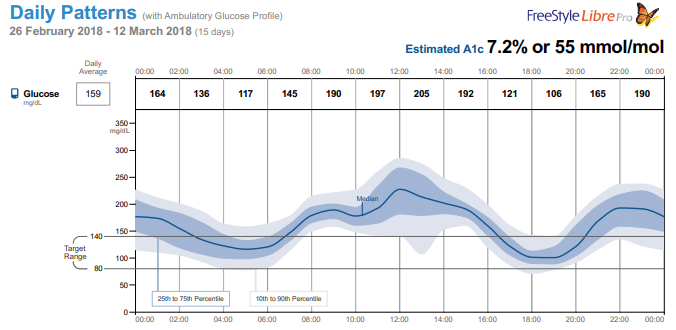
In 2012, post-retirement, the patient permanently moved to Potomac, Maryland and the medical records were transferred to the present family physician (Dr. Collin Cullen) in Washington DC. Although he continued the use of Metformin ER and blood pressure medications, Enalapril and Carvedilol, additional anti-glycemics were added as and when needed. Current medications include Metformin ER 500 Mg two tablets twice daily, Lisinopril 20 Mg Twice daily, Carvedilol 6.25 Mg twice daily, Glipizide 10 Mg twice daily, Jardiance 10 Mg once daily, Rybelsus 7Mg once daily, Atorvastatin 10 Mg once daily, Cyanocobalamin 1000mcg twice a month. Vitamin D 1000 IU daily. In 2018, continuous glucose monitor (CGM) was used to monitor interstitial glucose by the use of Abbott FreeStyleLibre. Data are presented in Figure 2. A typical glucose profile over days is shown in Figure 2. It shows a low of 117 to a high of 205 (daily average 159) with an estimated HbA1c of 7.2%.
In 2024, at the age of 87, the patient underwent the following tests to follow the progress of the atherosclerotic arterial disease of the blood vessels, as well as heart health, and vascular function or dysfunction, 1) non-invasive lower limb vascular assessment, 2) bilateral lower limb arterial doppler study, bilateral peroneal and posterior tibial nerve conduction study, 3) carotid artery calcium score, 4) bilateral carotid (neck) Doppler studies, and 5) echocardiography of the heart. Bilateral iliac, common femoral, and popliteal arteries showed diffuse wall thickening, and calcification with mild narrowing of the lumen. Despite these lesions, blood flow studies showed normal velocity waveforms. The left femoral artery showed wall irregularity and calcified plaques causing 20-30% luminal stenosis. Bilateral anterior tibial and dorsalis pedis arteries showed biphasic waveform, diffused wall thickening, and calcification with mild narrowing of the lumen. In the motor nerve, bilateral common peroneal nerve studies showed mildly prolonged latency with mildly reduced compound muscle action potential (CMAP) amplitude and reduced motor conduction velocity. Bilateral posterior tibial nerve studies showed mildly prolonged latency with reduced motor conduction velocity and normal CMAP amplitude. These studies indicate electrophysiological evidence of bilateral lower limb mild sensorimotor axonal with secondary demyelinating neuropathy.
Risk assessment of coronary artery calcium (CAC) score showed significant calcification of the coronary arteries. The number of calcifications in the right coronary artery was 3 Agatston Score (AS) 1007, left main coronary artery 0, left anterior descending artery 2 (AS 54), left circumflex artery 2 (AS 1748).
According to the American College of Cardiology, a CAC (AS) score of 100-400 relative risk of 4.3; a CAC score of 400-999-relative risk of 7.2, and a CAC score > 1000 relative risk of 10.8 [21]. Carotid Doppler studies on the other hand, showed multiple eccentric plaques in the internal carotid artery (ICA), external carotid artery (ECA), and right carotid bulb. The largest plaques measured 5.6x2.2 mm at the right carotid bulb causing no limiting stenosis. Multiple eccentric calcified plaques were seen in the left ICA, ECA and left carotid bulb, the largest plaque measured 3.6x1.4 mm at the left carotid bulb causing no flow limiting stenosis. Thickened intima-media was noted on both sides (1.4 mm on the right side 1.2 mm on the left side). Conclusions of the observation was that spectral waveforms including flow patterns and velocities in the above-mentioned vessels appeared normal with no evidence of significant stenosis of vessels.
2-D Echo and Doppler findings of the heart revealed a sclerotic aortic valve, trivial mitral valve and tricuspid valve regurgitation, suggesting a type of valve disease, where the valve’s flaps do not close properly. Left ventricle, mild concentric LVH. Normal LV systolic function. Grade 1 left ventricular diastolic dysfunction. Left atrium normal. The right ventricle and right atrium are normal in size, with normal right ventricular function. No LV/LA masses, vegetation or thrombus. The main pulmonary artery and aorta are normal. No pericardial thickening or effusion. Ejection fraction 60%. Ejection fraction in a healthy heart is 50% to 70%. However, it is worth noting that ejection fraction can vary with age. An ejection factor of 55 to 65 is considered normal regardless of age, but studies have shown that there can be age-related changes in ventricular volumes and ejection fraction. With advanced age a slight but significant decrease in end systolic volume (ESV), end diastolic volume (EDV) and ejection fraction (EF) has been observed. These findings underline the importance of using age-adapted values as the standard of reference when evaluating such studies (31). His blood chemistry was as follows; Cholesterol 99, HDL cholesterol 43, LDL cholesterol 33, Chol/HDL-C 23, Triglycerides 133, HbA1c 7.5.
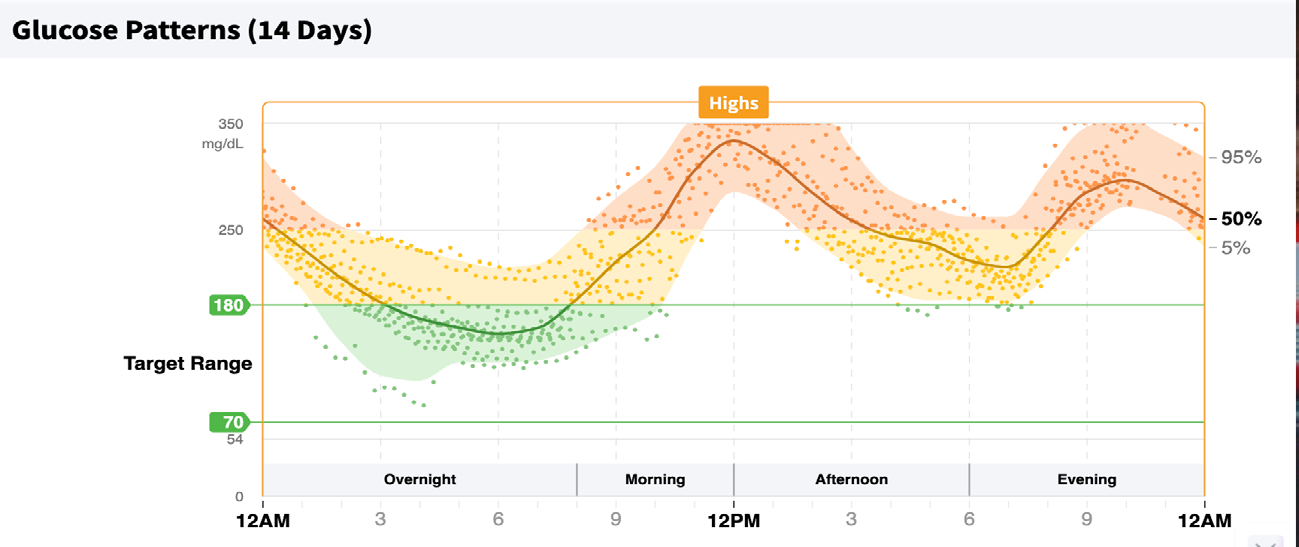
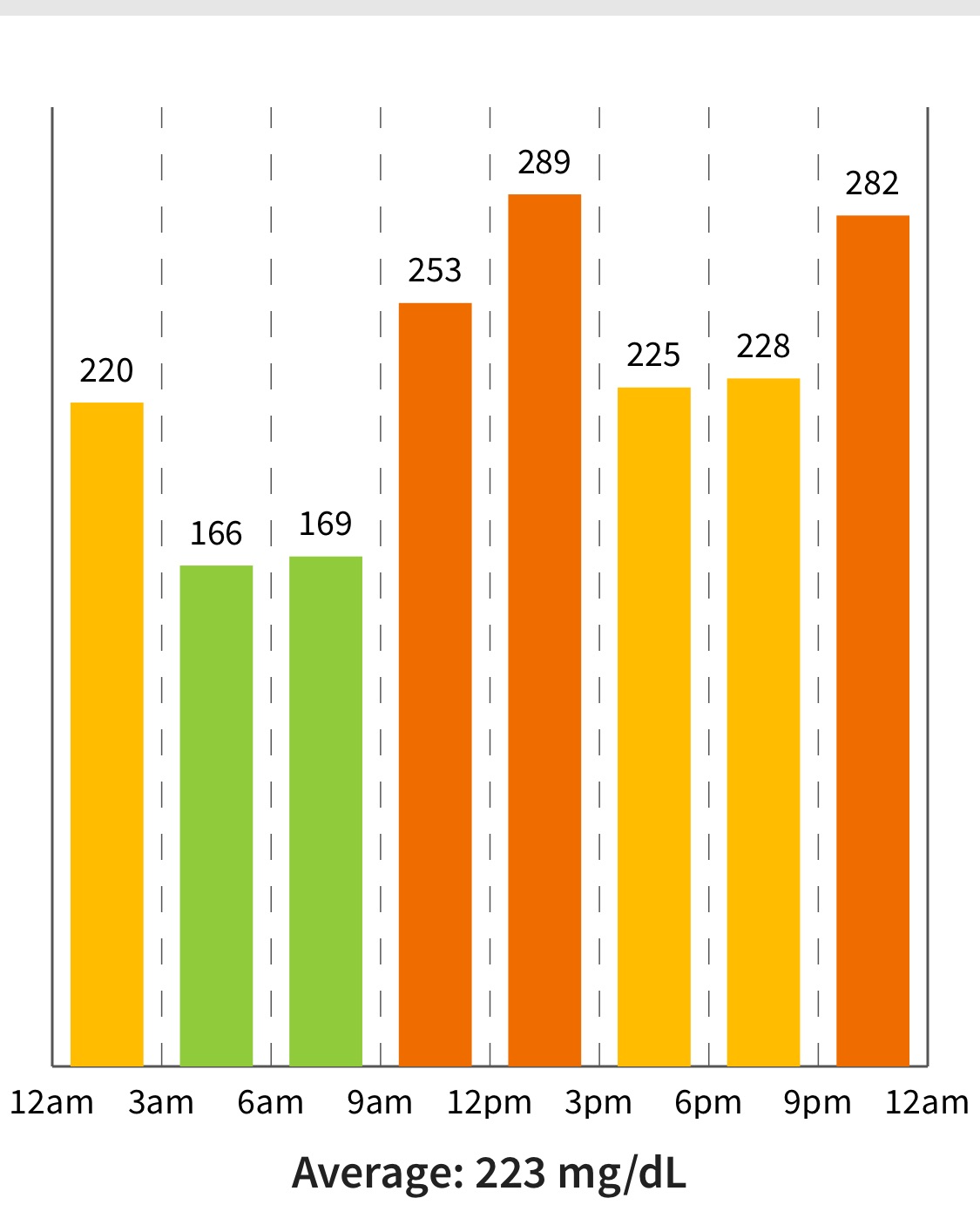
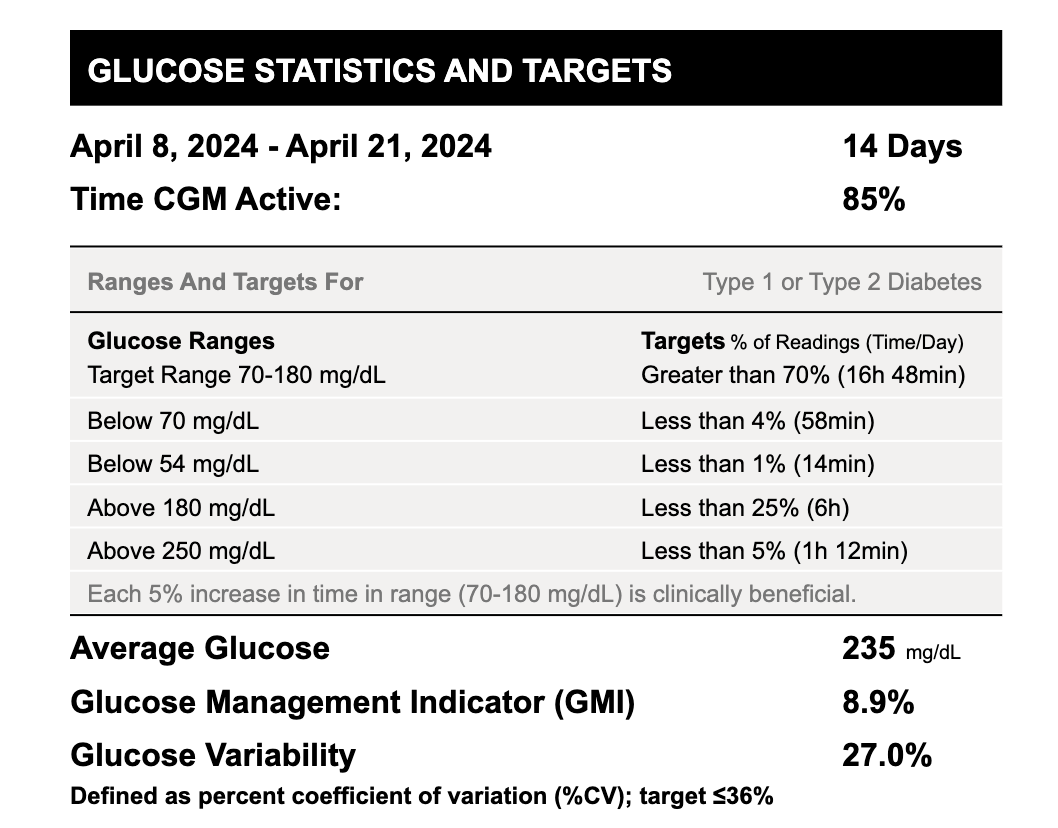
In April of 2024, the blood chemistry was as follows; EGR 59, Protein in urine (Trace), Hemoglobin 10.7, Fasting Glucose 168, HbA1c 8.1. Lipid Panel; Total Cholesterol 86, HDL- Cholesterol 42, Triglycerides 148, LDL- Cholesterol 21, Chol/HDLC ratio 2.0, Non-HDL Cholesterol 44. Because the patient had started developing age-related vascular lesions, signs of demyelinating neuropathy, Mitral valve and Tricuspid valve dysfunction and increased calcium scores in the right coronary artery, and left circumflex artery, the primary physician recommended the use of once-daily 30 units of long-acting insulin (Glargine, Lantus, Sanofi) to manage glycemic dysfunction better. The results of a daily glucose profile before the insulin administration are shown in Figure 3. The data shows that 95 % of the time, interstitial glucose as monitored by Abbott Freestyle Libre (Figures 3 & 4) was at the high-level zone. The glucose level was at the safe level only 5% of the time. Glucose Management Indicator (GMI: equivalent of HbA1c) was 8.9% and the average glucose was 235 mg/dl. Therefore, the intervention goals were to bring down the average glucose to a ‘safe zone’ so that the interstitial glucose stays in the safe zone for greater than 75% of the time.
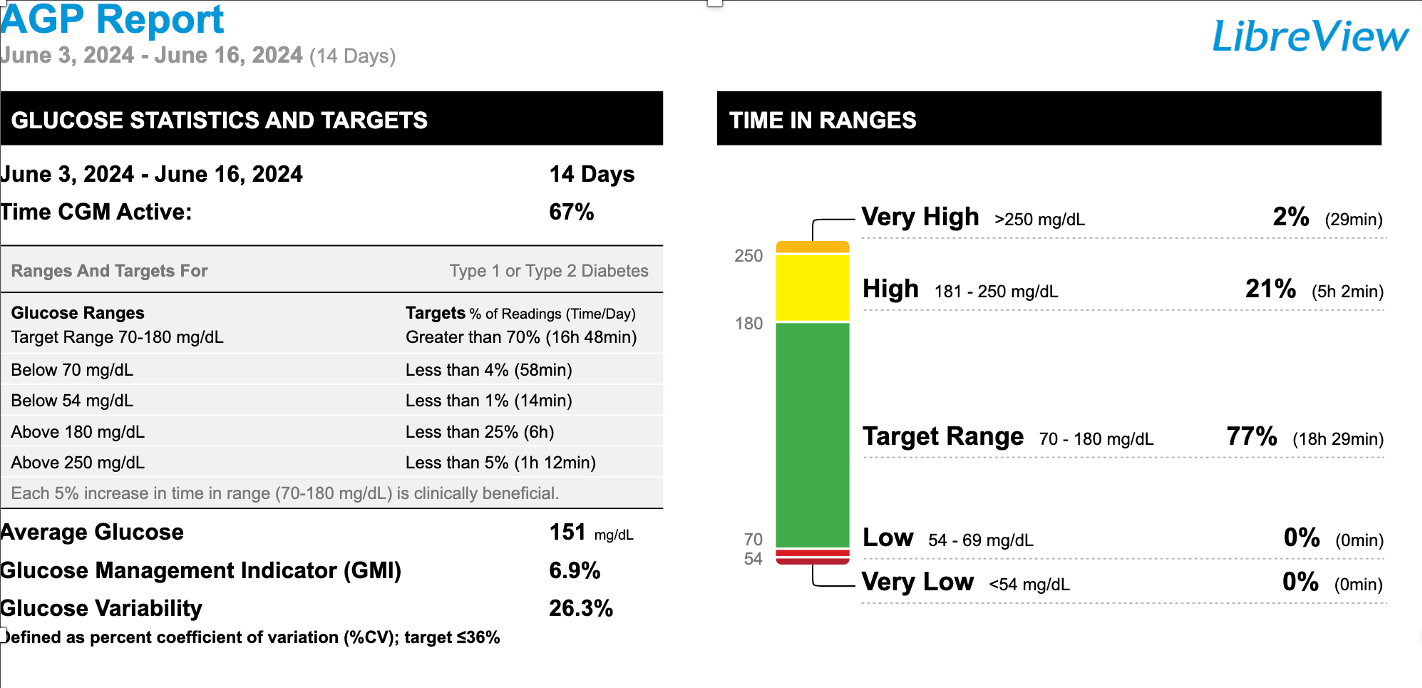
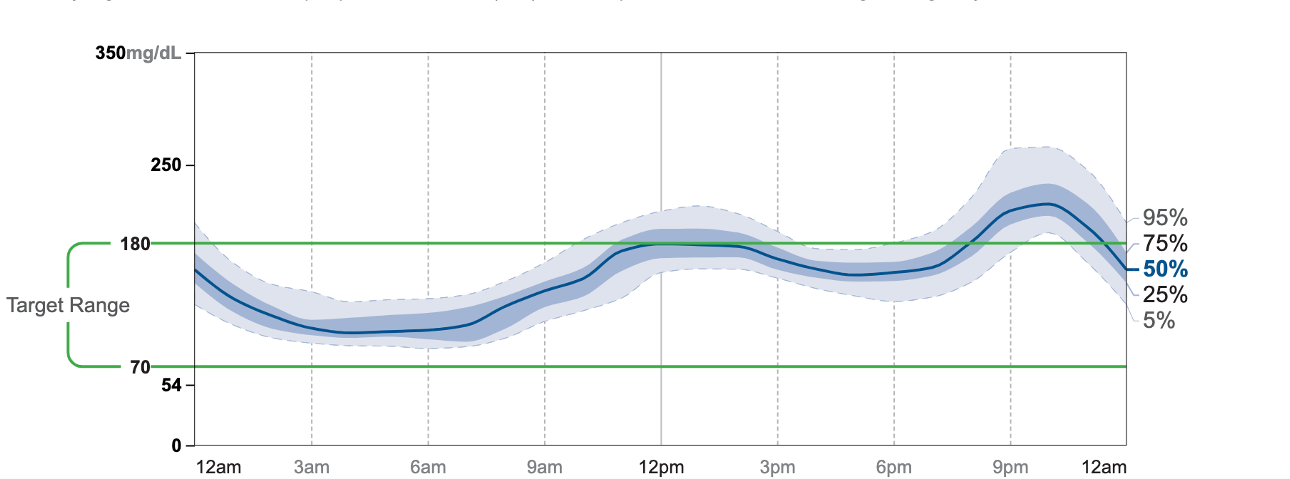
The results of administering long-acting insulin for 30- days are shown in Figures 5 & 6. The target range for glucose was 70-180mg/dl. Daily glucose profile was monitored for a 14-day period. Time in range was,-very high 2%, high 21%, Target range 77%. The Glucose Management Indicator was 6.9% and the daily average was 151mg/dl for the fourteen- day period.
The long-acting insulin effectively reduced the daily glucose levels to the desired target zones. Occasionally the glucose levels went to low levels during early morning hours (1AM to 6AM).
Since the patient is fond of international travel, he wanted to try higher dose insulin preparation so that he can take a smaller number of insulin pens while travelling. Therefore, patient was recommended to use Touejo-SoloStar, a Sanofi generic version of long-acting insulin, that contains 300 units/ per ml. Results on daily glucose profile post the generic version of long-acting insulin are presented in Figures 7 & 8.
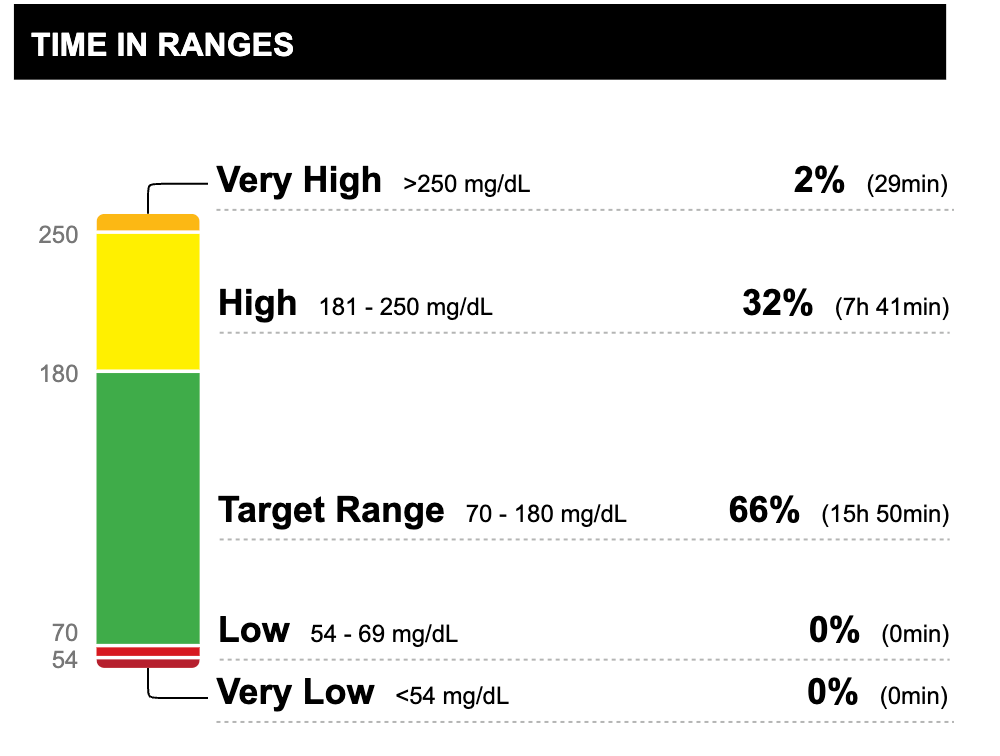
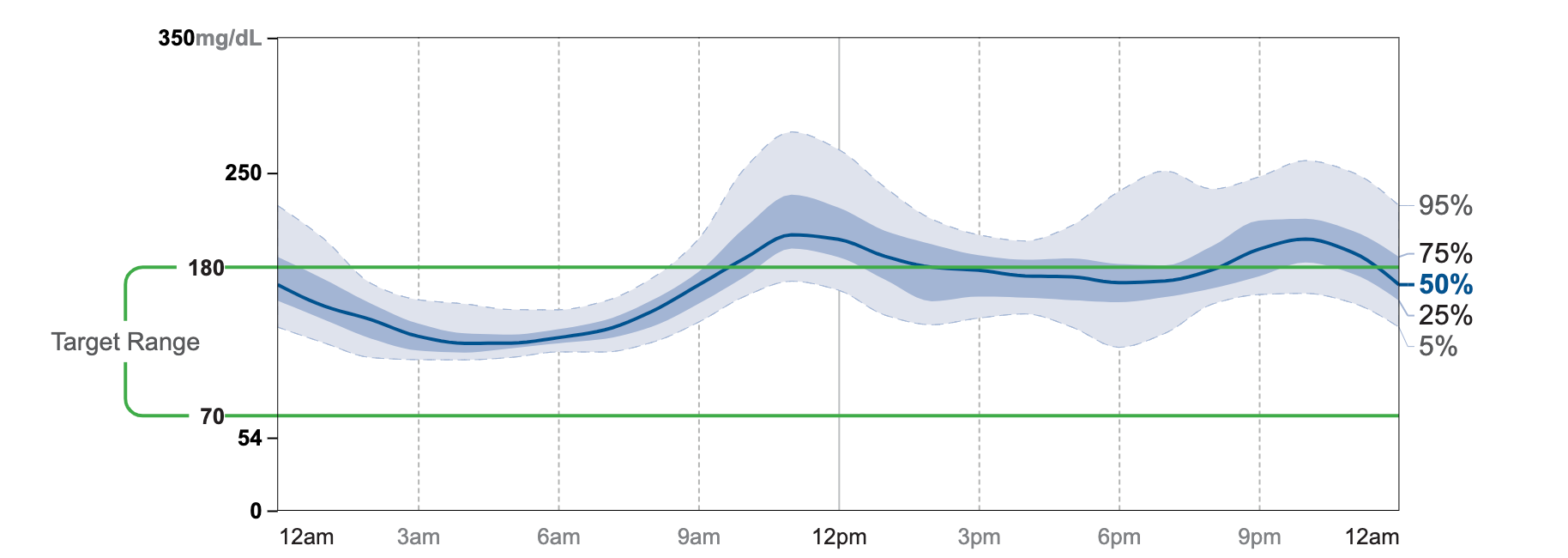
Glucose target range with the use of 30 units per day of Lantus insulin was 2% at a very high range, 21% at a high range 77% at the target range, average glucose was 151mg/ dl and a GMI of 6.9%, whereas, with 32 units per day of Touejo a generic version of long-acting insulin, glucose target range was 2% very high, 32% high and 66% at target range with a mean value of 168mg/dl and a GMI of 7.3%. Compared to the prior insulin values of 235mg/dl of glucose and a GMI of 8.9% these values are well within the age-adjusted normal values.
Discussion
Metabolic syndrome, which includes abdominal obesity, hypertension, dyslipidemia and impaired glucose tolerance is more common among South Asians and increases their risk of chronic vascular diseases. South Asian immigrants are disproportionately more at risk of developing cardiovascular diseases than other ethnic groups [22, 23, 24, 25, 26, 27, 28]. In a one-of- a-kind multicenter INTERHEART study, Professor Yusuf and Associates concluded that “Abnormal lipids, smoking, hypertension, diabetes, abdominal obesity, psychosocial factors, consumption of fruits, vegetables and alcohol, and regular physical activity account for most of the risk of myocardial infarction worldwide in both sexes and at all ages in all regions [28]”.
Based on the results of this study in 52 countries, they recommended that ‘approaches to prevention can be based on similar principles worldwide and have the potential to prevent most premature cases of myocardial infarction’. This case study highlights the increased risk of metabolic diseases in South Asian immigrants, emphasizing the importance of early diagnosis of metabolic risks, robust intervention of identified risks, and prevention of premature mortality in this population.
The subject for this case study is a South Asian immigrant, with an increased risk of developing cardiovascular disease at an earlier age. He arrived in the USA, at the young age of 27, with a desire to get advanced training in grain science technology. He was healthy, weighed 125 lbs., with a BMI of less than 21. Over the years he gained weight and developed hypertension at the age of 57. From the clinical history recorded, it is not certain as to how long the hypertension was unregulated. Uncontrolled hypertension led to the precipitation of left ventricular hypertrophy and as a result valve dysfunction and regurgitation. However, for the past two decades with a combination of Lisinopril (20 Mg daily) and Carvedilol (6.25 Mg daily), the blood pressure is in control. Most recent echocardiography of the heart function showed, grade-1 diastolic dysfunction, no LV/LA masses, and an ejection fraction of 60%. At the age of 61 the subject developed impaired glucose tolerance, which resulted in the diagnosis of maturity onset type-2 diabetes. Since then, he has been on anti-glycemic drugs and the fasting blood glucose and HbA1c levels have been monitored once in six months. The HbA1c levels have been fluctuating between 6.0 to 7.5 depending upon the combination of anti-glycemic medications used.
At the University of Minnesota, Professor Jay Cohn and associates developed a hypothesis that relied on treating the disease rather than focusing management of risk factors [29]. This novel method relies on performing a number of diagnostic tests and scoring the disease development and progress. Similar concepts were developed at the Robarts Research Institute, Guelph, Ontario, Canada for monitoring the coronary artery plaque volume [30, 31]. The subject of this study underwent several diagnostic tests to validate this hypothesis [29, 30, 31, 32, 33]. The results of such diagnostic studies have been reported in an earlier article [33]. In 2005, patient visited Robarts Research Institute, in Ontario, Canada and got a carotid scan done by the experts. At that time, there were no visible signs of intimal thickens, narrowing of the arteries or any visible subclinical atherosclerosis. However, over the years his vessels have developed intimal thickness, narrowing of the arteries, accumulation of calcium and visible atherosclerotic plaques.
According to the most recent studies he has developed demyelinating neuropathy, and dysfunction of the heart valves and visible regurgitation. However, he has no signs of stenosis or altered blood flow in any of the vascular beds imaged and has an ejection fraction of 60%. As for the management of dysglycemia, current studies have demonstrated that with an appropriate dose of long-acting insulin, HbA1c could be maintained between 6.5 to 7.3%. Even though all of the cardiometabolic risk factors are monitored regularly and maintained at expected normal levels, the patient has signs of peripheral demyelinating neuropathy. Microvascular complications of diabetes are those long-term complications that affect small blood vessels. These typically include retinopathy, nephropathy and neuropathy [34]. While there are established approaches for early diagnosis and managing retinopathy and nephropathy, the search results suggest treatment options for demyelinating peripheral polyneuropathy appear to be more limited compared to other diabetic complications [35]. Peripheral mechanisms that underlie neuropathic pain include altered gene/protein expression in sensory neurons, inflammatory responses involving Schwann cells, macrophages, degeneration of small nerve fibers and central sensitization in the spinal cord and brain. One of the mechanisms by which peripheral nerve injury is induced seems to be through Schwann cells and macrophages releasing arachidonic acid and facilitating synthesis of its derivatives, prostaglandins [36].
The common features of neuropathic pain include spontaneous or evoked burning, shooting pain, allodynia, hyperalgesia or sensory loss, suggesting a shared underlying pathology [32, 33, 34, 35, 36]. Peripheral neuropathy is probably the earliest and most common clinical complication of dysglycemia. It is indeed a large disease burden and needs greater attention than what currently exists. There are hardly any diagnostic tools available at present to monitor the microvascular flow of vascular beds of lower limbs, especially the sole. Yet another important area is the therapy of this condition. There is an immediate and urgent need for new therapies based on known mechanisms that cause this condition [37].
Conclusion
This case study underscores the multifaceted challenges faced by South Asian immigrants in managing cardiovascular and metabolic health. Despite having his risk factors— such as hypertension, impaired glucose tolerance, and dysglycemia—well-controlled through medication and lifestyle adjustments, the subject has developed significant complications, including peripheral demyelinating neuropathy and atherosclerosis. South Asian immigrants are at a heightened risk of developing cardiovascular diseases and metabolic disorders due to genetic predispositions and lifestyle changes after migration. Early and continuous monitoring of risk factors is crucial in managing their health. While the subject’s hypertension and blood glucose levels have been managed effectively with medication, the emergence of additional complications highlights the limitations of current management strategies. This emphasizes the need for a more holistic approach that integrates risk factor control with targeted interventions for complications.
The development of atherosclerotic plaques and peripheral neuropathy despite controlled risk factors illustrates the complexity of metabolic syndrome and its long- term impacts. This case suggests that managing individual risk factors alone may not be sufficient to prevent or fully address vascular disease-related clinical complications.
The progression from subclinical atherosclerosis to visible plaques and neuropathy indicates a gap in early diagnostic capabilities. Improved diagnostic tools and methods for monitoring microvascular health, especially in the lower limbs, are urgently needed to detect and address complications before they become severe. The current therapies for neuropathy and microvascular complications are inadequate.
There is an immediate need for innovative treatments that target the underlying mechanisms of these conditions, such as inflammatory responses and nerve fiber degeneration. The findings align with the recommendations from the INTERHEART study and other research, emphasizing preventive measures based on global principles. Early diagnosis, robust intervention, and preventive strategies are essential in reducing the burden of cardiovascular and metabolic diseases among high-risk populations. In summary, this case study highlights the ongoing need for improved diagnostic and therapeutic approaches for managing the long-term complications of metabolic syndrome. Enhanced research, tailored interventions, and comprehensive management strategies are vital to improving outcomes for individuals at high risk of cardiovascular and metabolic diseases.
References
-
Chew NE, Ng CH, Tan DJH, Kong G, Lin C, et al. (2023) The global burden of metabolic disease: Data from 2000- 2019. Cell Metab 35(3): 414-428.
-
Zhang K, Ma Y, Luo Y, Song Y, Xiong G, et al. (2023) Metabolic diseases and healthy aging: identifying environmental and behavioral risk factors and promoting public health. Front Publ Health 11:1253506.
-
Chong B, Kong G, Shankar K, Chew HSJ, Lin C, et al. (2023) The global syndemic of metabolic diseases in the young adult population: A consortium of trends and projections form the Global Burden of Disease 2000- 2019. Metabolism 141: 155402.
-
Budreviciute A, Damiati S, Sabir KD, Onder K, Schuller- Goetzburg P, et al. (2020) Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front Publ Health (8): 574111.
-
Andersson, C, Nayor M, Tsao CW, Levy D, Vasan RS (2021) Framingham Heart Study. JACC Focus Seminar 77(21): 2680-2692.
-
van Daalen KR, Zhang D, Kaptoge S, Paige E, Angelantonio ED, et al. (2024) Risk estimation for the primary prevention of cardiovascular disease: considerations for appropriate risk prediction model selection. Lancet 12(8): E1343-E1358.
-
Abohelwa M, Kopel J, Shurmur S, Ansari MM, Awasthi Y, et al. (2023) The Framingham study on cardiovascular disease risk and stress-defenses: A historical review J Vasc Dis 2(1): 122-164.
-
Pencina MJ, Agostino RBD, Larson MG, Massaro JM, Vasan RS (2009) Predicting the 30-year risk of cardiovascular disease. The Framingham Heart Study Circ 119(24): 3078-3084.
-
Mills KT, Stefanescu A, He J (2020) the global epidemiology of hypertension. Nat Rev Nephrol 16(4): 223-237.
-
Boutari C, Mantzoros CS (2022) A 2022 update on the epidemiology of obesity and a call to the action: as its twin COVID-19 pandemic appears to be receding, the obesity and dysmetabolism pandemic continues to rage on. Metabolism 133: 155217.
-
GBD 2021 Diabetes Collaborators (2023) Global, regional and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Diseases Study 2021. Lancet 402(10397): P203-234.
-
Canto ED, Ceriello A, Ryden L, Ferrini M, Hansen TB, et al. (2020) Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. Euro J Prevent Cardiol 26(2): 25-32.
-
Anand SS, Dagenais GR, Mohan V, et al. (2012) Glucose levels are associated with cardiovascular disease and death in an international cohort of normal glycemic and disglycemic men and women. The EpiDREAM cohort study. Euro J Prev Cardiol 19: 755-764.
-
Chew NWS, Ng CH, Tan DJH, et al. (2023) The global burden of metabolic disease: Data from 2000 to 2019. Clin and Transl Rep 3: 414-428.
-
Unnikrishnan R, Anjana RM, Mohan V (2014) Diabetes in South Asians: Is the phenotype different. Diabetes 63(1): 3-55.
-
Patel M, Abatcha S, Uthman O (2022) Ethnic differences between South Asians and White Caucasians in cardiovascular disease-related mortality in developed countries: a systematic literature review. System Rev 11: 207.
-
Kandula NR Kanaya AM, Liu K, Lee JY, Herrington D, et al. (2014) Association of 10-yearand lifetime predicted cardiovascular disease risk with subclinical atherosclerosis in South Asians living in America (MASALA) study. J Am Heart Assoc 3(5): e001117.
-
Gerstein HC (1997) Dysglycemia, not just diabetes, is a continuous risk factor for cardio vascular disease. Evid Based Cardiovasc Med 1(4): 87-88.
-
Khera AV, Emdin CA, Drake I, Natarajan P, Bick AB, et al. (2016) Genetic risk, adherence to a healthy lifestyle, and coronary disease. New Engl J Med 375(24): 2349-2358.
-
Sridhar Y, Naidu MUR, Usharani P, Raju YSN (2007) Non- invasive evaluation of arterial stiffness in patients with increased risk of cardiovascular morbidity: A cross- sectional study. Ind J Pharmacol 39(6): 294-298.
-
Landry A, Spence JD, Fenster A (2004) Measurement of Carotid Plaque Volume by 3-Dimensional Ultrasound. Stroke 35(4): 864-869.
-
Deshpande A. Shah NS, Kandula NR (203) Obesity and cardiovascular risk among South Asian Americans. Curr Cardiovasc Risk Rep 17(3): 73-82.
-
Dod R, Rajendran A, Kathrotia, Clarke A, Dodani S (2023) Cardiovascular disease in South Asian Immigrants: a review of dysfunctional HDL as a promoter marker. J Racial Ethn Health Disp 10(3): 1194-1200.
-
Taylor R (2024) Understanding the cause of type 2 diabetes. Lancet Dain & Endocrinology 12(9): p664-673.
-
Volgman AS, Palaniappan LS, Aggarwal NT, Gupta M, Khandelwal A, et al. (2018) Atherosclerotic cardiovascular disease in South Asians in the United States: epidemiology, risk factors, and treatments: a scientific statement from the American Heart Association. Circ 138(1): e1-e34.
-
Ahmed ST, Rehman R, Akeroyd JM, Alam M, Shah T, et al. (2018) Premature coronary heart disease in South Asians; burden and determinants. Curr Atheorscler Rep 20(1): 6.
-
Rao GHR, Kakkar VJ (2001) Coronary Artery Disease in South Asians: Epidemiology, Risk Factors and Prevention. Jaypee Med Publishers.
-
Yusuf S, Hawken S, Ounpuu S, et al. (2004) Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. The Lancet 364(9438): 937- 952.
-
Duprez DA, Duval S, Hoke L, Florea N, Grandits G, et al. (2021) Early cardiovascular structural and functional abnormalities as guide to future morbid events. Euro J Prevent Cardiol 28(11): 1214-1221.
-
Divani AA, Luft AR, Flaherty, Rao GHR (2012) Direct diagnosis is superior to risk factor prediction tools for management of vessel wall disease. Front Neuro 3: 36.
-
Spence JD, Eliaswiz M, Hackman DG, Galil R, Lohmann T (2002) Carotid plaque area: a tool for targeting and evaluating vascular preventive therapy. Stroke 33(12): 2916-2922.
-
Maarek A, Gandhi PG, Rao GHR (2015) Identifying autonomic neuropathy and endothelial dysfunction in type 11 diabetic individuals. EC Neuro 2: 63-78.
-
Rao GHR (2024) Early diagnosis of Risks and management of Cardiometabolic Diseases: A Case Study. Open Access J of Cardiol 8(1): 000199.
-
Fowler MJ (2008) Microvascualr and Macrovascular complications of diabetes. Clin Diab 26(2): 77-82.
-
Kocot-Kepska M, Zajackowska R, Mika J, Wordliczek J, Dobrogowski J, et al. (2012) Peripheral mechanisms of neuropathic pain-The role of neuronal and non-neuronal interactions and their implications for tropical treatment of neuropathic pain. Pharmaceuticals (Basel) 14(2): 77.
-
Li Y, Liu Y, Gao M, Haung L, Chen K, et al. (2023) Diabetic vascular diseases: molecular mechanisms and therapeutic strategies. Nature Signl Trans and Targ Ther 8: 152.
-
Pacifico, P, Coy-Dibley JS, Miller RJ, Menichella DM (2023) Peripheral mechanisms peripheral neuropathic pain. Front Mol Sci 16: 1252442.
- Anomalous Origin of the Left Coronary System from the Right Coronary Cusp: A Rare Coronary Anomaly in a Patient Undergoing Aortic Stenosis Workup
- Optimizing the Therapeutic Potential of Sacubitril/Valsartan: The Promise of Co-Crystal Engineering
- Association between Mortality and Topography of Peripheral Arterial Disease due to Atherosclerosis Obliterans
- Mitral Valve Replacement vs Mitral Valve Repair
- Characteristics and Evolution of Patients with Heart Failure Hospitalized in the Cardiology Department of Dalal Jamm Hospital
- Distribution of Association between Basic Knowledge of Chest Pain and Myocardial Infarction (Heart Attack) and Demographic Variables: A Survey-Based Study